| Computers, Materials & Continua DOI:10.32604/cmc.2022.029365 | |
| Article |
A Prototype for Diagnosis of Psoriasis in Traditional Chinese Medicine
1Institute of Medical Informatics, Statistics and Epidemiology, University of Leipzig, Leipzig, 04107, Germany
2Zhejiang Academy of Traditional Chinese Medicine, Hangzhou, 310007, China
3Tongde Hospital of Zhejiang Province, Hangzhou, 310007, China
4Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, 100053, China
5Institute of Information on Traditional Chinese Medicine, China Academy of Chinese Medical Sciences, Beijing, 100700, China
*Corresponding Author: Yan Zhu. Email: zhuyan166@126.com
Received: 02 March 2022; Accepted: 27 May 2022
Abstract: Psoriasis is a chronic, non-communicable, painful, disfiguring and disabling disease for which there is no cure, with great negative impact on patients’ quality of life (QoL). Diagnosis and treatment with traditional Chinese medical technique based on syndrome differentiation has been used in practice for a long time and proven effective, though, up to now, there are only a few available studies about the use of semantic technologies and the knowledge systems that use Traditional Chinese Medicine (TCM)-syndrome differentiation for information retrieval and automated reasoning. In this paper we use semantic techniques based on ontologies to develop a prototypical system for the diagnosis of Psoriasis. For this purpose, a domain ontology is developed for syndrome differentiation of psoriasis vulgaris (PV). This ontology is founded on an adapted version of the general formal ontology (GFO), with the evidence-based clinical practice guideline of TCM for psoriasis vulgaris (Guideline 2013) as the primary data sources. The implemented prototype, called ONTOPV, contains this domain ontology and is aimed at a decision support system for diagnosis and treatment of PV. This system uses a case-database for Case Based Reasoning (CBR), combined with fuzzy pattern recognition. Experimental results show that the ONTOPV realizes the basic functionalities of data collection, querying, browsing and navigation, and supports rule-based knowledge reasoning, and integrates fuzzy pattern recognition. It can provide users with clinical decision support for TCM syndrome differentiation in diagnosis of psoriasis.
Keywords: Clinical guideline; knowledge base; GFO; ontology; TCM; CBR; fuzzy pattern recognition; psoriasis vulgaris
Ontology plays an increasing role in the field of knowledge representation. Actually, it presents the most advanced techniques to analyze, conceptualize and axiomatize the knowledge of a domain of interest. Knowledge exhibits various levels of abstraction. We may distinguish general knowledge that is presented often by rules and formal axioms from knowledge about individual cases. Furthermore, ontology is increasingly adopted to combine with other methods of artificial intelligence, notably with techniques of machine learning. A particularly interesting method is case-based reasoning, which originated from cognitive psychology and is now a relevant subtopic of artificial intelligence. Case-based reasoning is a form of analogical reasoning. When encountering a novel problem, one searches for an already solved case that is closest to the problem. Then, the solution of the known case is adapted to a solution of a new problem. After the new problem is solved, the revised case will be recorded and added as an experience [1]. This paper is a contribution to a longstanding research program that has, among others, following aims: (a) preserving the rich heritage of the traditional Chinese medicine by transforming the content of documents and of the informal experiential knowledge of the doctors into formal computer-processable knowledge systems; (b) provision of the developed systems for the usage in the practice of TCM; (c) comparative study of the principles of Western medicine and of TCM and the attempt to integrate both into a framework of integrative medicine. This paper is related to (a) and (b): we explored the possibility of using modern techniques based on ontologies to develop a system for the diagnosis of Psoriasis. Compared with using western medicine, the diagnosis and treatment with TCM pursues a personalized approach. According to a patient’s behavior of yin and yang, cold and heat, as well as the course of the disease, a corresponding interventional plan can be proposed, using a large number of typical and distinct cases. The CBR’s process is similar to that of TCM diagnosis process, which uses previous experience [2] and is based on the thinking way in terms of imagery and analogical reasoning [3,4]. Therefore, the unique characteristics of TCM about personalized diagnosis and treatment is more adequate for applications of CBR. Now, CBR has been gradually applied into the field of TCM, particularly focusing on the design of expert systems and clinical decision support systems (CDSS). For example, Yang et al. [5] established a TCM expert system based on CBR. Peng et al. [6] developed a syndrome differentiation and treatment system with traditional Chinese medicine methods. Wang et al. [7] proposed a CBR-based TCM expert system combined with fuzzy rule-based reasoning. These works show that the reasoning mechanisms for CDSS of TCM based on CBR are becoming increasingly mature. However, due to the deficiency of cases, poor quality of data and limited clinical applications, most of these systems cannot provide sufficient support for an accurate clinical decision-making in TCM. In summary, we claim that CBR together with fuzzy reasoning are essential aspects of TCM-diagnosis of PV, and we believe that the developed prototype supports this thesis.
Psoriasis, classified by the World Health Organization (WHO) as a severe disease [8], is a chronic, non-communicable, painful, disfiguring and disabling disease for which there is no cure, with great negative impact on patients’ QoL. However, the diagnosis and treatment with TCM based on syndrome differentiation has a long practical history and has also proven effective [9–11]. According to TCM theory, psoriasis is caused by many factors, such as blood deficiency, blood heat, dryness and wind, as well as lack of nutrition, which can be divided into different syndrome types, based on characteristics of clinical symptoms. Accordingly, different treatment principles and methods shall be applied. The TCM diagnosis is based on the combination of manifestation of pulse, tongue coating, complexion, physical constitution and other signs and symptoms. Some of them are certain, while many are fuzzy, ambiguous, nonlinear and uncertain [12]. In the process of diagnosis, TCM doctors often rely more on their own knowledge and experience to find solutions, rather than using logical reasoning. Therefore, it is difficult to establish a TCM expert system, due to uncertainty of knowledge representation, data acquisition and the lack of logic reasoning. The complexity and fuzziness of TCM-knowledge also leads to new challenges because there is the need for developing new forms of knowledge representation and reasoning mechanism.
In clinical practice, TCM doctors make the diagnosis of psoriasis mainly by their professional knowledge and clinical experience. Young and inexperienced doctors are prone to make a misdiagnosis or a missed diagnosis, resulting in a lower-than-expected curative effect. In this paper, a prototype for diagnosing and treating of psoriasis, called ONTOPV, is proposed, which is based on a domain ontology and uses CBR combined with fuzzy pattern recognition. This system exploits the valuable and extensive heritage of TCM knowledge.
Up to now, there is still little research on the use of automated reasoning and semantic-technologies for the adjunctive diagnostic aspects of TCM psoriasis, and the mature TCM psoriasis diagnostic decision support systems. On the other hand, a number of CDSS based on semantic technologies, especially on ontology and fuzzy logic and automated reasoning have been developed and used in a wide range of scientific fields, particularly in clinical medicine practice, with convincing results. We have carefully researched and reviewed some of this relevant literature by searching for keywords. For example: Riaño et al. [13] in 2012 introduced an ontology to the care of chronically ill patients and implemented two personalization processes and a decision support tool to effectively support managing patients and automatically transform intervention plans describing health-care general treatments into individual intervention plans, as well as to detect anomalous circumstance such as misdiagnosis, unobserved comorbidities, unobserved related diseases, etc. Martínez-Romero et al. [14] in 2013 introduced an ontology-based system, iOSC3, which is constituted by an OWL (ontology web language) ontology and a set of SWRL (semantic web rule language) rules representing experts’ knowledge into intelligent supervision and treatment of critical patients with acute cardiac disorders. Bau et al. [15] in 2014 constructed a CDSS for surgery based on domain ontology and rules reasoning in the setting of hospitalized diabetic patients. The system could help clinicians to control the glycemic of diabetic patients in surgery for avoiding hypoglycemia. Alfonse et al. [16] in 2014 presented an ontology-based system for cancer diseases knowledge management, which could be used to determine types and stages of the cancer for patients, and then recommend treatment options. Zhang et al. [17] in 2014 proposed an ontology-driven decision support method, which was an automated procedure for diagnosing mild cognitive impairment (MGI) by using magnetic resonance imaging (MRI). This approach was realized by means of encoding specialized MRI knowledge into ontology and constructing a rule set using machine learning algorithms. Kalra et al. [18] in 2021 proposed a driving style recognition system based on fuzzy logic which was designed to classify different driving styles and control reckless driving by taking the longitudinal/lateral acceleration and speed as input parameters, results indicated that the proposed system could classify reckless driving and reduce the number of accidents. M. Aly and H. Rezk [19] in 2021 proposed a fuzzy logic-based fault detection and identification method for open-circuit switch fault in grid-tied photovoltaic inverters. Bucci et al. [20] in 2011 presented an approach to the use of ontologies and Bayesian Networks (BNs) in medical diagnosis, based on the adoption of predefined structures for the BNs, leading to reduced extensions to the domain ontology and allowing probabilistic analysis. Fujita et al. [21] in 2012 presented a fuzzy reasoning approach by applying aggregate function for medical decision into making a diagnosis. A. Velu and M. Thangavelu [22] in 2022 presented a climatic information data model dependent on OWL ontology by coordinating satellite information using the semantic web for ocean applications, which was intended to predict the climate marvel through ontology models by presenting information about different climate conditions influenced by weather attributes. Jayalakshmi et al. [23] in 2021 proposed a context-aware health monitoring system to monitor the health and psychological condition of the affected or quarantined elderly patients due to COVID-19, the framework was developed with a fuzzy-reasoning mechanism to make a prediction/decision about the patient’s status using the event and medical context. Uciteli et al. [24] in 2019 presented an innovative ontology-based approach to support the specification of search queries and the preparation of the document corpus, with intent to vigilantly observe medical devices during post-market surveillance (PMS) for identifying safety-relevant incidents. El-Sappagh et al. [25,26] in 2015 & 2018 proposed a fuzzy ontology-based CBR framework by means of constructing a fuzzy case base OWL2 ontology and a fuzzy semantic retrieval algorithm for semantic diabetes diagnosis. Palanikkumar et al. [27] in 2022 presented a fuzzy logic approach, which was used for selecting a mining method for different deposit characteristics. As the underground minerals extraction was a difficult multi criteria decision making problem, the proposed model yielded suitable mining method for minerals extraction at the specified Indian mines and are used by the mine authorities.
The study of the above literature has inspired the design of a prototype system. This system should contain at least three variables, 1) an ontology module on the diagnosis of psoriasis in Chinese medicine; 2) an automated reasoning module for diagnostic decisions based on the SWRL rule base; and 3) a CBR module based on fuzzy logic for similar case studies.
In this paper, a prototype named ONTOPV is introduced, which is based on ontology of TCM-diagnostic knowledge of psoriasis vulgaris, uses a SWRL rules base for automated reasoning and a case-database for CBR. This prototype is intended to help TCM practitioners to diagnose psoriasis-related syndromes, and to provide clinical decision support if necessary. The prototype of the ONTOPV-system can realize at least the following three procedures:
1) Diagnosis of PV: A doctor gathers the required information by querying and observing the patient, about age, gender, lifestyle, family history, signs and symptoms. Then, based on the patient’s main complaint, the acquired information is put into a template, with the content transformed as input to the rule basis and diagnosis ontology. The inference engine derives possible diagnoses, which are provided to the doctor as advice for diagnosis and treatment.
2) Development of intervention plans: according to the recommended diagnostic results, an intervention plan is (semi-) automatically generated for the patient diagnosed, including some TCM treatments and/or common therapies of Western medicine, like topic-and photo therapy, etc. Furthermore, a personalized care plan on demand will be recommended for the patients.
3) Information Retrieval: with a semantic querying mechanism, users may access the system to ask questions about the information or required data that are stored in the ontology and in the CBR-based Knowledge Base of PV. Then, the answers together with relevant graphic displays will be returned to the user.
Fig. 1 shows that the diagnostic information collected by a doctor from the patient, such as symptoms, signs, skin lesion area, pulse and tongue manifestation, chief complaint, among other diagnostic information, is put into the knowledge-based system as input parameters, compared with the basic syndrome types defined in the guideline 2013 [28], stored in the ontology and matched against the customized reasoning rules in the SWRL rule base. If the given prerequisites are met, one or more inference rules are triggered to obtain the corresponding diagnosis result and the related treatment plan. The input is also compared with the past cases in the case database. If there are matched case records, the cases with higher similarity are extracted as reference cases and provided to the user for comparative analysis and diagnostic decision making.
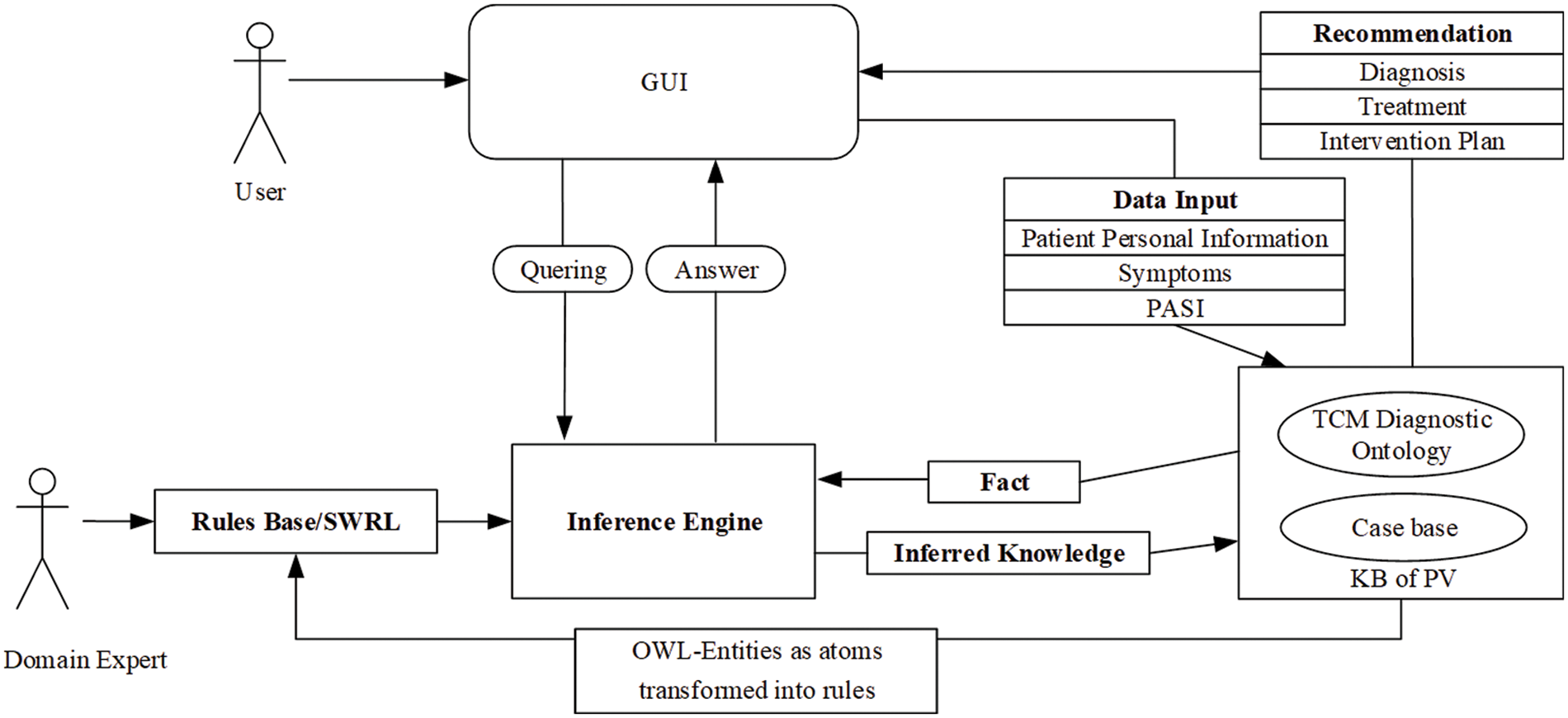
Figure 1: Architecture of ONTOPV
3 Construction of ONTOPV Prototype
3.1 Construction of Domain Ontology for Syndrome Differentiation of Psoriasis Vulgaris
To build this prototype, a domain ontology for syndrome differentiation of psoriasis vulgaris was firstly developed. Various documents were used for the construction of the basic conceptual hierarchy, such as evidence-based clinical practice guideline of TCM for psoriasis vulgaris (2013) [28] (hereafter referred to Guideline 2013), which was jointly compiled by the Dermatology Branch of the China Association of Chinese Medicine, the Dermatology Committee of the Beijing Association of Traditional Chinese Medicine, and the Dermatological and Venereal Diseases Committee of the Beijing Association of Integrative Chinese and Western Medicine in 2013, and published in the Journal of Traditional Chinese Medicine, acting as the latest Chinese medicine evidence-based clinical practice guideline for psoriasis vulgaris, and focusing on the identification and classification of psoriasis vulgaris in Chinese medicine and Chinese medicine treatment. Furthermore, the WHO Global Report on Psoriasis (2016) [8] focusing on the public health impact of psoriasis was also utilized. The aim is to encourage member states to make efforts to raise awareness and eliminate stigma around psoriasis. The Guideline for the diagnosis and treatment of psoriasis in China (2018 simplified edition) [29], the latest version of the Chinese psoriasis diagnosis and treatment guidelines compiled by the Committee on Psoriasis of the Chinese Society of Dermatology and Venereology, published in the Chinese Journal of Dermatology, further standardizes the diagnosis and treatment of psoriasis in China mainly on the basis of the two previous editions of the Chinese psoriasis diagnosis and treatment guidelines, with the aim of improving the efficiency of diagnosis and treatment and improving the quality of life of patients. Additionally, TCM-related documents about psoriasis vulgaris are used to provide information about the classification of psoriasis, symptoms (primary symptoms, secondary symptoms, and combined symptoms), syndrome types, diagnosis, treatment methods, prescriptions, drug ingredients, drug compatibility, etc. Some basic semantic types (equivalent to class in OWL) have been obtained from the guidelines and other related literature, such as disease name, basic syndrome types, blood heat syndrome, blood dryness syndrome, blood stasis syndrome; simultaneous syndromes; basic symptoms including main symptoms, minor symptoms; methods of treatment; recommended formulas and drugs; pharmaceutical ingredients and so on. We used the ontology-editor Protégé and applied a top-down approach which adopts the framework of general formal ontology (GFO) and its middle-level core ontology GFO-TCM described in [30,31]. The basic semantic types of psoriasis vulgaris are listed below:
• Health Problems: The psoriasis-related health problems are mainly divided into 3 categories, namely, disease, symptom, (incl. main symptoms, minor symptoms, accompanied symptoms), and syndrome or pattern. It is believed that one could introduce a class of “disease” as a subclass of process in GFO; hence, any disease, in particular PV, can be considered as a process. The patient is integrated into this process, he “participates” in this process. This approach is justified by the integration law of GFO, which postulates that for any material object, in particular a patient P, there exists a process Proc(P) so that P and Proc(P) are connected in a particular way [32]. Symptoms, signs, and syndromes can then be understood as properties/attributes of a disease. This approach allows a further classification in various sub-classes of disease, as functional diseases, anatomical diseases; actually, the disease classification of the ICD can be reconstructed within this framework.
• Formula: A formula or prescription usually contains some medicinal components, used for treating an illness, such as psoriasis vulgaris.
• Drug/Medicinal: Usually referring to those medicinal substances recorded in Chinese Materia Medica, but also to some medicaments of western medicine.
• TCM Diagnose for syndrome differentiation: According to the Guideline (2013), each type of syndrome of psoriasis vulgaris has a set of corresponding symptoms, which can provide a guideline for the diagnosis of TCM syndrome differentiation.
• Method of treatment: The method of treatment is composed of the conventional therapies with TCM and western medicine, such as: TCM prescriptions and drugs, medicated bath, biological therapy, topical therapy, systemic therapy, phototherapy, etc.
• Participant/Person: Such as doctors, patients, etc.
• Compatibility and Caution: the medicinal composition and dosage of prescriptions, special instructions, and contraindications between certain medicinal or chemical ingredients.
In general, our ontology has two levels of abstraction: a core ontology that describes some basic notions of TCM domain as health problem, formula, drugs, person, etc. and a particular domain ontology for psoriasis vulgaris that specializes the basic notions as basic syndrome types, symptoms, etc. which are adapted to the disease PV in this way. The ontology includes 99 classes, 64 properties (incl. Object-and Data-properties), 1622 axioms, 285 annotation assertion. The OWL ontology is available now in the ONTOPV project website at GitHub: https://github.com/haibinich/ontopv. as shown in Fig. 2. The relevant concepts have been explicitly introduced in [29,30].
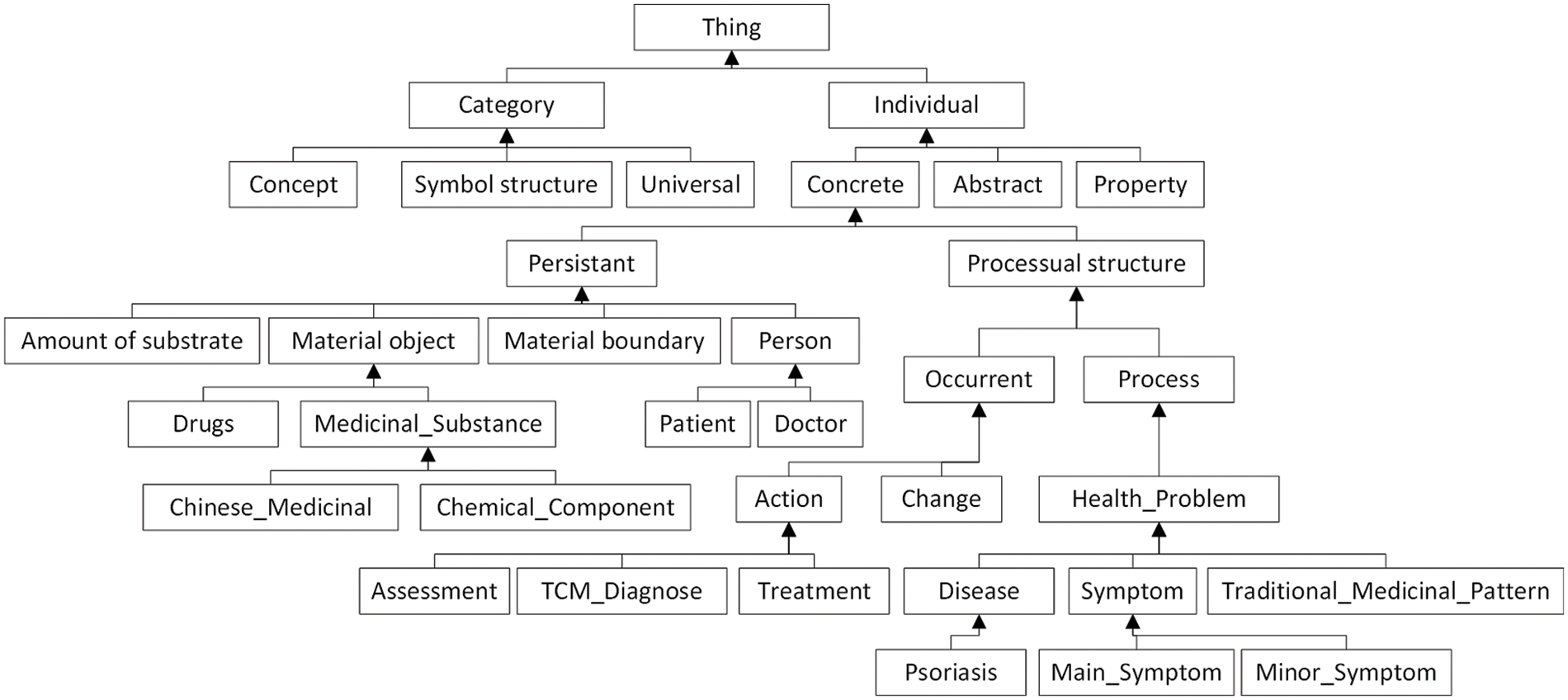
Figure 2: Basic hierarchy of the ontology
According to the instructions in the Guideline (2013), the corresponding instantiated entities are established for the basic semantic types from the classification in the ontology, such as instances for major symptoms, minor symptoms, combined symptoms, prescriptions, drugs, pharmaceutical ingredients, treatment methods, etc. These types establish the classes of the core ontology and below the core classes, there are subclasses, which are associated to the disease PV, for example, PV-symptoms, PV-combined-symptoms, PV-treatment methods etc. The instances of the PV-classes are stipulated, depending on context, relevance, and usability. For example, the instances of PV-symptoms are various concrete symptoms, being relevant and typical for PV. There is, for example, an instance of “bright red lesion” in the class PV-main symptom, an instance of “dry mouth” in the class PV-minor symptom. Furthermore, the relationships between instances of different classes can be defined by introducing object properties.
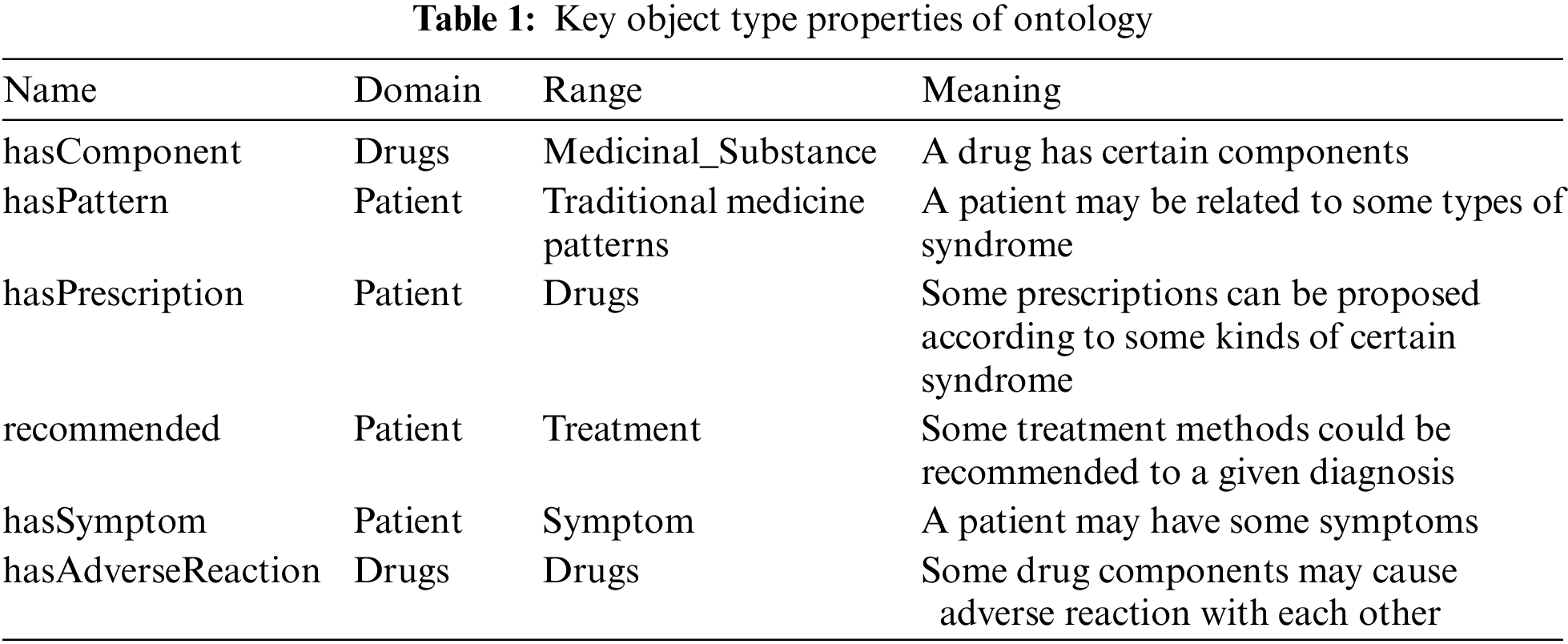
Finally, the relationship between different entities in the TCM diagnosis ontology for psoriasis vulgaris needs to be clarified. About 20 common binary object properties that relate individuals to individuals have been specified, including annotation. According to the Guideline 2013, PV can be annotated by several zheng/syndromes, including some basic zhengs and combined zhengs, due to its different onset processes or observed symptoms. Some key object properties are: hasComponent, hasPattern, hasPrescription, recommended; and hasSymptom etc., as shown in Tab. 1.
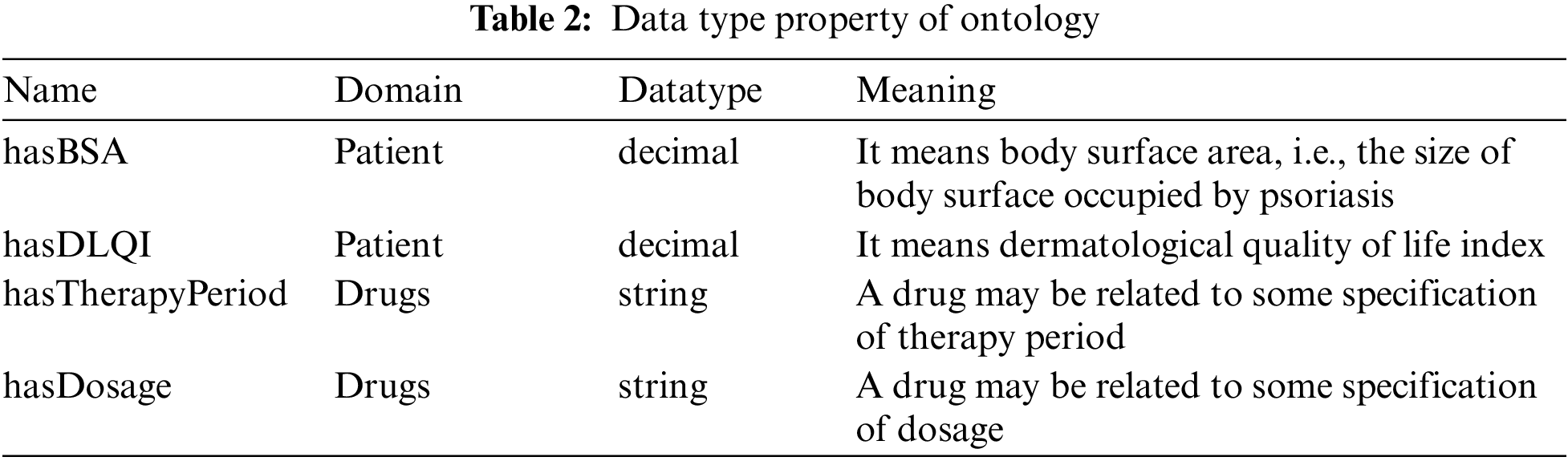
Through these built-in object properties, individuals that belong to different concepts in the ontology are correlated to each other, and stored in the OWL ontology in the form of RDF triple as object property assertions. Then, some basic datatype properties that relate individuals to literal data are built as well, such as hasBSA (domain: Patient, data type: decimal) that means Body Surface Area, i.e., the size of body surface occupied by psoriasis; hasDLQI (domain: Patient, data type: decimal) that means Dermatological Quality of Life Index; hasTherapyPeriode (domain: Drugs, data type: string); hasDosage (domain: Drugs, data type: string); as shown in Tab. 2.
3.2 Construction of Rules Base
The rules of diagnosis-based syndrome differentiation and treatment must take into account specific regulations for diagnosis and medication in the evidence-based guidelines of TCM for psoriasis vulgaris [28]. For example, a corresponding treatment mechanism is established for the patients’ observed symptoms as defined by the guidelines to ensure compliance with the standard operation required by the guidelines. In the ONTOPV related TCM diagnosis ontology, there are 30 well-defined reasoning rules constructed for diagnosing certain syndrome types in terms of corresponding sets of symptoms, or used to check the compatibility of drug components and to query whether some given components may cause side effects due to drug interactions. Using the rule base, a reasoning process can be performed, and the obtained results can be useful in giving diagnoses and/or treatment suggestions according to the patient’s symptoms. There are 3 examples and explanations of rules written in SWRL:
(1) Rule example 1 for the assessment of PV:
(2) Rule example 2 for syndrome differentiation of PV:
this rule means if a patient (a) of psoriasis vulgaris has main symptoms of bright red lesions and rash continuously increased, and also has a minor symptom of yellow urine, then the pattern assigned to the patient is “syndrome of blood heat”.
(3) Rule example 3 for prescription:
this rule means a patient (a) of psoriasis vulgaris who has been ascribed to have a syndrome of heat in blood would be prescribed a recipe named “blood-cooling and toxin-resolving decoction”.
3.3 Case-Based Reasoning Using Fuzzy Logic
As mentioned above, a diagnosis of TCM is usually based on the comprehension of manifestation of pulse, tongue coating, complexion, physical constitution and other signs and symptoms. Some of them are certain, but more of them are uncertain, fuzzy, ambiguous, and nonlinear. Hence, in the process of diagnosis, TCM doctors often rely much on their own knowledge and experience rather than on logical reasoning to find solutions. Therefore, the difficulty in establishing a TCM expert system lies in the uncertainty of knowledge representation, data acquisition and logic reasoning. The complexity and fuzziness of knowledge pose new challenges and requirements to knowledge representation and reasoning mechanism.
In the case of psoriasis vulgaris, for any possible diagnosis and treatment in view of syndrome differentiation, TCM doctors must firstly identify the patient’s symptoms to obtain the corresponding diagnosis results. This could be considered as a kind of pattern recognition. According to M. Friedman and A. Kandel [33], a pattern is an abstract object, which is inspected for the recognition process. And we usually regard a pattern as a schematic description of an object that we want to recognize. A schematic description can be understood as a type that can be instantiated, and this type can be specified by some selected features. Thus, recognizing an object (Obj) with respect to a pattern (P) means to capture/understand Obj as an instance of P. We may introduce a number of standard patters P1, …, Pn and recognize an object (Obj) as an instance of one of the standard patterns P1, …, Pn. If the patterns are exhaustive, then we achieve a classification procedure: given an object we determine which pattern or type the object (Obj) belongs to.
To achieve a clinical diagnosis of psoriasis vulgaris, a doctor acquires symptoms reported by patients as subjective chief complaint, and objectively observes signs. For some cases, these gathered information cannot be used to determine exactly which pattern the patient belongs to. As for such cases, we must introduce a degree of belonging to a standard pattern. This procedure is called fuzzy pattern recognition. An example is taken from the evidence-based clinical guidelines for psoriasis vulgaris in TCM (2013), according to the diagnostic criterion of blood-heat syndrome, which may have two main symptoms of bright red lesions and continuously increased rashes, as well as four minor symptoms, including irritability, upset, yellow urine, red tongue and rapid pulse. As long as a patient has all major symptoms and at least one minor symptom, the syndrome of blood-heat can be determined. The same principle could be applied to the identification of blood dryness syndrome, except that the latter symptoms can be expressed as major symptoms of pink lesions, dry scales and minor symptoms of dry mouth, pale tongue, thready pulse. If a patient is observed with some symptoms of blood heat syndrome, in combination with some symptoms of blood dryness syndrome, then how to identify this patient. This case can be observed quite often in practice, because the onset of this disease is a gradual process according to the theory of TCM. At the early stage of this disease, it is mostly manifested as blood heat syndrome and as blood dryness syndrome at the middle stage, but mostly as blood stasis syndrome at the late stage. It can also be manifested as other types of combined syndrome simultaneously. Sometimes, decisions cannot be easily made by TCM doctors on the basis of two-valued logic. Hence, the problem about pattern recognition in a process of syndrome differentiation can be considered as a more-or-less type rather than yes-or-no type, which pertains to the topic of fuzzy pattern recognition [34].
Some methods in this paper are inspired by Zadeh’s fuzzy set theory [35,36], which is a generalization of crisp set theory. A fuzzy set consists of objects and their respective grades of membership in the set. The grade of membership of an object in the fuzzy set is given by a subjectively defined membership function, ranging from 0 to 1, where the grade 1 denotes full membership, and the closer the value is to 0, the weaker the object’s membership in the fuzzy set [34] is.
A mechanism of information retrieval is proposed, which integrates ontology and CBR using fuzzy pattern recognition. The integration provides automatic reasoning and semantic retrieval in line with the norms of TCM evidence-based clinical guidance for psoriasis vulgaris, and also simulates the thinking mode of experts based on fuzzy logic. Meanwhile, a solution is carried out to find a similar case from the case base using the proposed method of lattice degree of nearness [33,37]. In the ONTOPV prototype, the user can input data that are collected from patients as input parameters into the system. Such data include main symptoms, minor symptoms, personal information (age, gender, past history, family history, etc.), chief complaint (all subjective description of the patient), etc.
Then the system processes these data by searching for rules included in the SWRL rules base. If the given preconditions are met, one or more rules are triggered, and subsequently the corresponding standard diagnosis results and treatment scheme will be obtained. At the same time, it can also be compared with the past cases stored in the case database. If there is a matched case record, the case with higher similarity will be extracted as the reference case and provided to the user for comparative analysis. The workflow of case retrieval in ONTOPV is shown in Fig. 3.
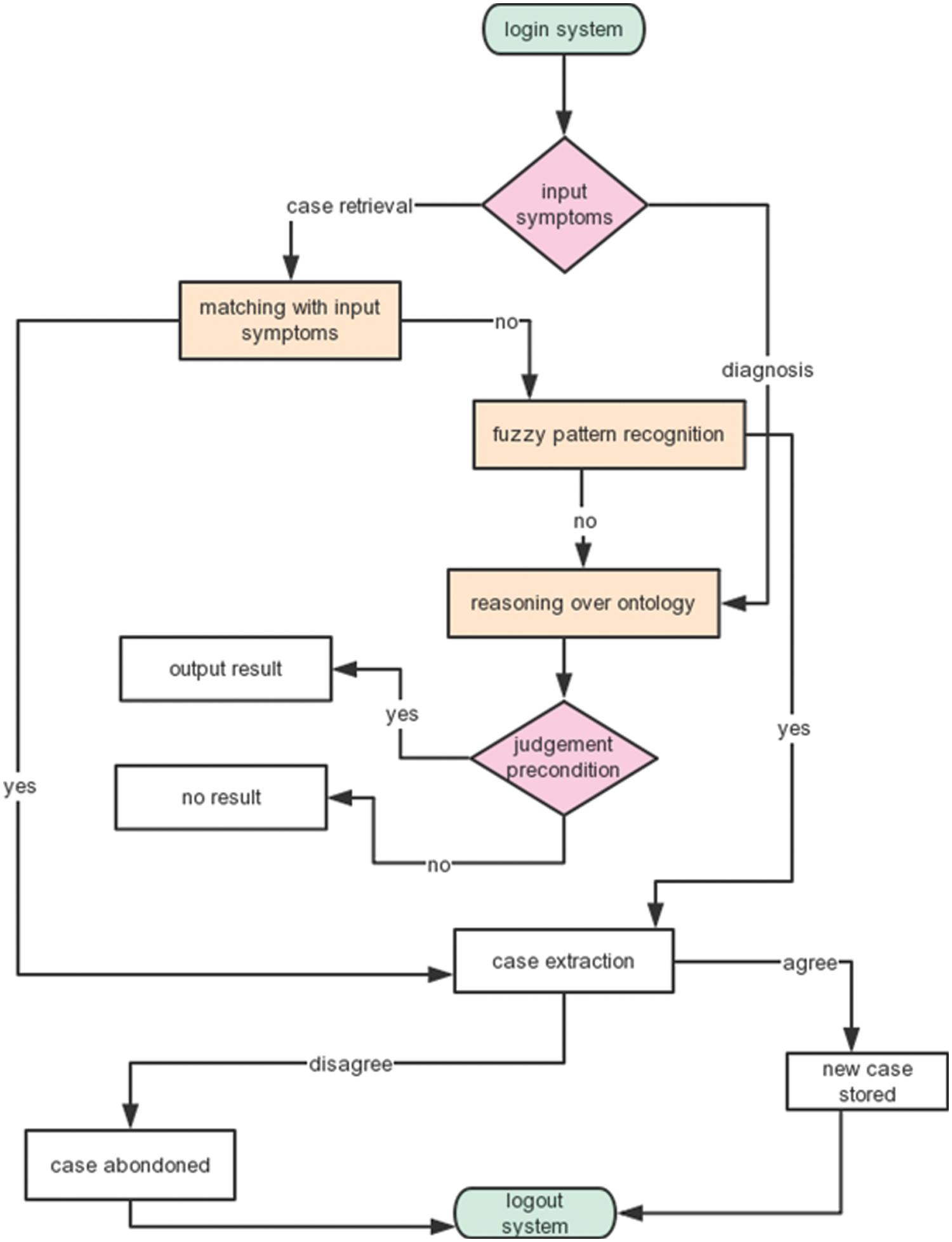
Figure 3: Workflow of case retrieval in ONTOPV prototype
Here presents an example to illustrate this workflow. Assume P be a patient who has some symptoms, such as “continuously increased rashes, pink lesions, dry scales, yellow urine, dry mouth, red tongue, rapid pulse”, among which “continuously increased rashes, yellow urine, red tongue, rapid pulse” are typical symptoms of blood heat syndrome, and “pink lesions, dry scales, dry mouth” are typical symptoms of blood dryness syndrome, in the meantime “red tongue, rapid pulse” can also be interpreted as symptoms of the combined syndrome of heat-toxin according to the guideline 2013. In order to determine which type/syndrome this patient should be ascribed to, all the data are put into the system ONTOPV as parameters for the purpose of diagnosis. If there is a SWRL rule matching one of the standard criteria for the blood dryness syndrome, then this rule can be triggered. From this, we know the basic syndrome of this patient is blood dryness. But the question is still open for the doctor, how the patient can be interpreted with the combined symptoms of blood heat and of heat-toxin? And what is the most adequate prescription he may recommend for this patient? Thus, we can search the case base, looking for some cases of patients with similar symptoms. If the doctor succeeds, he may find at least one case similar to the patient, then he could extract this case as a comparable reference for his clinical diagnostic decision. Finally, the updated case can also be stored in the case base if the doctor agrees with the extracted case, or the extracted case may be ignored if the doctor disagrees with the case record. However, this system is still considered to just provide some auxiliary decision support, and in any case, the final clinical decision must be made by the doctor.
Below is the elaboration on how the above process of case retrieval is performed. Firstly, cases of patients can be considered as a pattern space A = (a1, a2 … am), where ai, 1 ≤ i ≤ m are vectors in Rn, i.e.,: each pattern is characterized by n features. For example, each case can be characterized by gender, age, patient’s chief complaint, symptoms, Western medicine diagnosis, TCM diagnosis, syndrome type, treatment method, recommended medication, and quantitative score of each syndrome type based on the comprehensive score according to the membership function defined.
Assuming a universe of discourse U = {several patient cases}; the diagnostic features of the patient-cases include several symptoms, which need to be diagnosed and classified according to the color of the lesion, the nature of the lesion, tongue and pulse manifestation, urination, complexion, and chief complaint. Thus, the pattern space of syndrome S = {blood heat syndrome, blood stasis syndrome, blood dryness syndrome, combined syndrome} can be obtained, and the combined syndromes can be further divided into wind, dampness and heat toxin, etc. according to guideline 2013. Among them, the pattern of blood heat-, blood stasis-, blood dryness-, and combined syndrome can be considered as fuzzy sets. To determine the type syndrome that the patient exhibits, a TCM doctor must firstly determine which features or symptoms go to this classification. This problem can be measured by using the degree of membership and similarity between two fuzzy sets A and B, which is discussed below.
With the principle of maximum membership in a fuzzy set, a simple membership function can be firstly established to determine which basic syndrome type a patient has. According to the guideline, a basic syndrome type can be defined. If a patient exhibits two major symptoms and at least one minor symptom, then the diagnosis is true, which means the patient’s symptoms have full membership degree with this syndrome type. Accordingly, a simple membership function can be established.
A weight value has been assigned to each symptom, including the main and the minor symptom. For example, there are altogether 2 main symptoms and 4 minor symptoms in the blood-heat syndrome. Then a weight value of 0.3 is assigned to each main symptom and 0.1 to each minor symptom. Similarly, a weight value has been assigned to each symptom in every syndrome type, so that a simple membership function can be established to judge a given case of a patient, membership degree of this patient’s syndrome type. Then the weights of the patient’s symptoms just need to be added up to estimate the degree of membership in the class of a syndrome type he may have.
Supposing we have a fuzzy set of symptoms and syndrome of a patient in the case database P = {blood fever, bright red lesions, dry scales, slow pulses, pale tongue, yellow urine, heavy head} corresponding to each basic syndrome of blood heat, blood dryness, combined syndrome wet due to the defined membership function above, a fuzzy vector of the patient p = (1, 0.5, 0.3), which may be interpreted as the patient’s symptom set with respective grade of membership: 1(true) for blood heat syndrome, 0.5 (possible) for blood dryness syndrome and 0.3 (less possible) for the combined syndrome wet.
Assume there are two reference cases A and B in the case base, and both correspond to the above-mentioned three syndrome types in terms of a grade of membership:
Given fuzzy vector a = (0.6, 0.4, 0.2), with the symptom set {Qi deficiency, bright red lesions, upset, red tongue, string pulse, dry scales, dry mouth, dizziness}
And fuzzy vector b = (0.7, 0.1, 0.1) with the symptom set {blood heat accumulation, white scales, red skin lesions, thin and white tongue fur, dry mouth, slippery pulse}
Using the method of lattice degree of nearness proposed by P. Z. Wang [37], the similarity between two fuzzy sets can be defined by the following expression:
where
then the inner product and the outer product of p and a are 0.6 and 0.3 respectively; while the inner product and the outer product of p and b are 0.7 and 0.3 respectively. The lattice distance between the two is 0.65 and 0.7. Obviously, the case of P and B is closer. Therefore, B can be taken as an approximate case.
In this section, several experiments were designed to evaluate the performance of ONTOPV, and conducted by 3 voluntary domain experts. The evaluation is made with the following three aspects taken into consideration: the structural design of the prototype, the knowledge extraction of the knowledge base and the user interface.
4.1 The Experiment of System Structure and Design
1) Rationality of designed conceptual hierarchy
Task 1.1: the rationality of concept classification refers to verifying whether the classification for the ontology concept classification is basically consistent with the terminology system in the Guideline 2013 and/or whether it is consistent or compatible with the terminology system of other relevant literature. Experts confirm by comparing the ontology concept hierarchy with the terminology of the literature collected, for example, comparing and confirming that the concepts of diseases, syndromes, and symptoms in terms of terminology component (TBox) in the ontology. In this task, three domain experts, after checking the terminologies used for domain ontology and the conceptual hierarchy, all confirmed that the conceptual hierarchy of ontology was consistent and/or compatible with the terminology in TCM theory.
2) Rationality of designed semantic relationship
Task 1.2: the rationality of the semantic relationship means whether the semantic relationship designed in the ontology can reflect the diagnosis process based on syndrome differentiation in the TCM clinical guidelines of psoriasis, and whether the semantic modeling is reasonable. Experts confirmed by randomly calling a triple related to the object attributes and data attributes in the ontology. Fig. 4 illustrates an example of a semantic relationship, namely, experts confirm by randomly extracting the triples related to the object-and data-properties in the assertion component (ABox) of the ontology which has been uploaded and displayed on a local Fuseki server. During the evaluation process, the following triple was extracted, the experts checked and verified this triple and confirmed the definition of this triple was accurate and effective.

Figure 4: An example of triple extraction
“:decoction_of_nourishing_blood_and_toxin_resolving :hasComponent :danshen_root”
Fig. 4 shows that an extracted prescription named “decoction of nourishing blood and toxin resolving” has the component “danshen root”.
3) Rationality of designed reasoning rules
Task 1.3: the rationality of reasoning rules refers to verifying whether the description of the reasoning rules in the ontology can correctly reflect the diagnostic criteria in accordance with the Guideline 2013 and conform to the doctors’ clinical experience. Experts run the PELLET inference engine through the OWL ontology and randomly select a certain inference result to confirm whether the result is accurate. In this task, the rule example 2 described in the Section 3.2 was extracted and verified by experts. After inspection, the experts unanimously confirmed that this inference rule was reasonable and effective. Fig. 5 illustrates the inference results of the diagnostic TCM pattern and recommended prescriptions based on patient p1’s presenting symptoms.
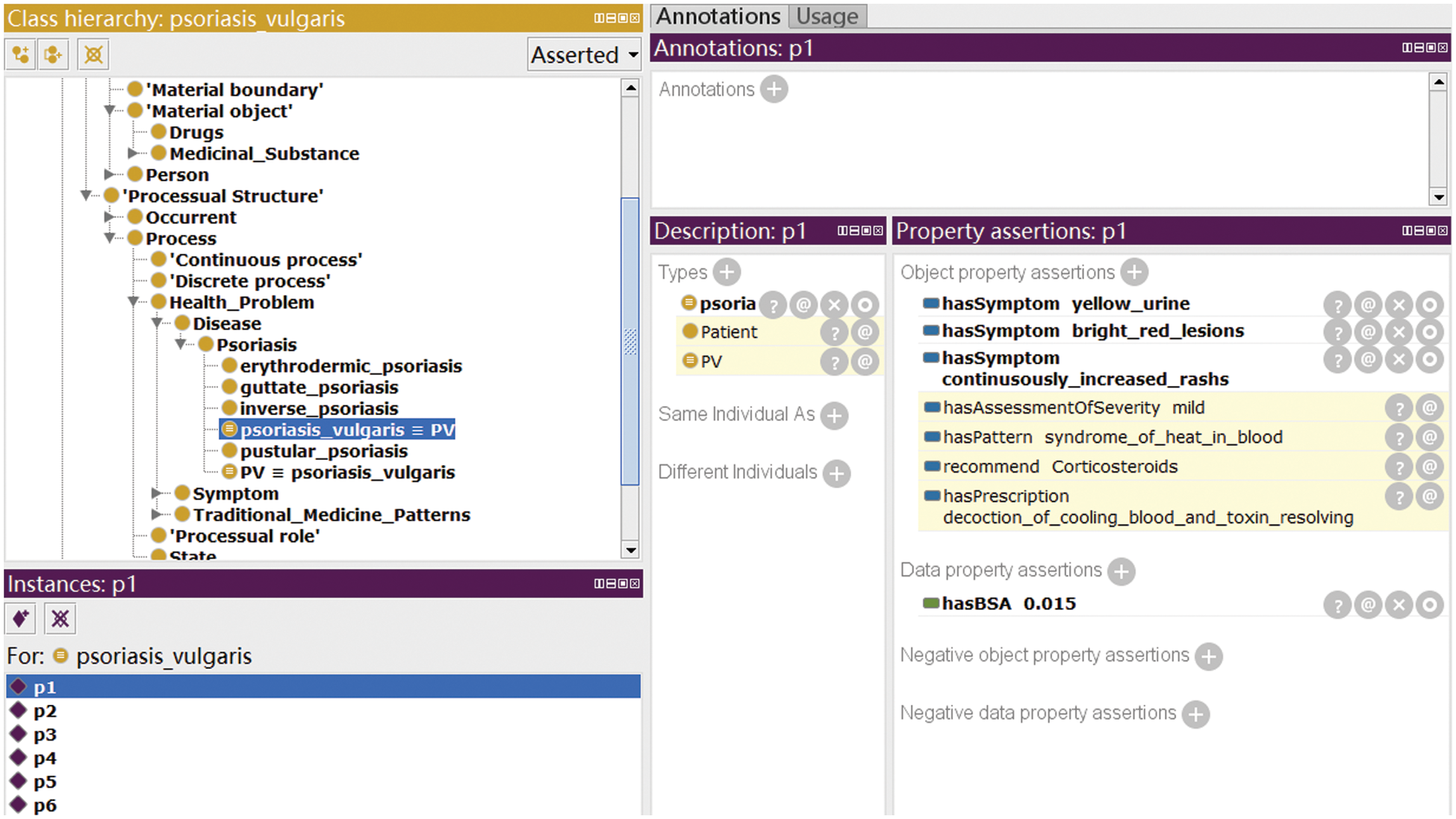
Figure 5: An example of illustration of rules-based reasoning according to patient’s symptoms
4) Rationality of designed case template
Task 1.4: the rationality of the designed case template means that experts randomly select and evaluate a case template in the case base to confirm whether the designed template structure is reasonable.
In this task, a patient’s case record was extracted as a case template and described according to this template’s case number, personal information, past history, chief complaint, symptoms, diagnosis information, TCM patterns, treatment principle, prescription, recommendation, outcome, scoring, etc. After examination, the experts agreed that the design of the case template was reasonable and valid.
4.2 The Experiment of Knowledge Extraction
1) Evaluate the accuracy of knowledge extraction related to the search items
Task 2.1: After entering a search item, experts confirmed whether the relevant knowledge of the extracted item was accurate and/or applicable.
2) Similarity and applicability of extracted cases
Task 2.2: Based on comparing and evaluating an input case with the extracted case, experts confirmed whether the extracted cases had applicability and reference value.
3) Integrity of the database
Task 2.3: After evaluating the coverage integrity of the database, experts randomly input certain search terms related to the field to query, and saw if they could find the corresponding return results.
In this task, experts tried to find 4 prescription by imputing the search terms, namely, the decoction of cooling blood and toxin resolving; the cooling blood and activating blood compound; the decoction of xiao yin; the compound capsules of qing dai; the correct results were returned for two of them, but the decoction of xiao yin and the compound capsules of qing dai hadn’t got expected results returned. Based on these results, experts hold that the database must be further expanded to cover more query possibilities.
4.3 The Evaluation of User Interface
1) Rationality of the layout and functional design of the user interface
Task 3.1: experts, after completing the above tasks, especially passing the tasks 1.3, 2.1–2.3, evaluated whether the user interface layout and functional design are reasonable.
2) User experience and user-friendliness
Task 3.2: experts evaluated their user experience and the convenience of operation upon the user interface through the operational process of the above tasks 1.3, 2.1–2.3.
3) Real-time response speed
Task 3.3: experts evaluated and confirmed the response time from input parameters to output results through the operation process of task 1.3 and tasks 2.1–2.3.
Fig. 6 shows an example of Ontology reasoning according to the task 1.3 after imputing the main symptoms of a patient, including bright red lesion, continuously increased rashes, and the minor symptoms, including irritability and upset, yellow urine. The system provides the inferred results of a syndrome of heat in blood-heat with the corresponding medication recommendations.
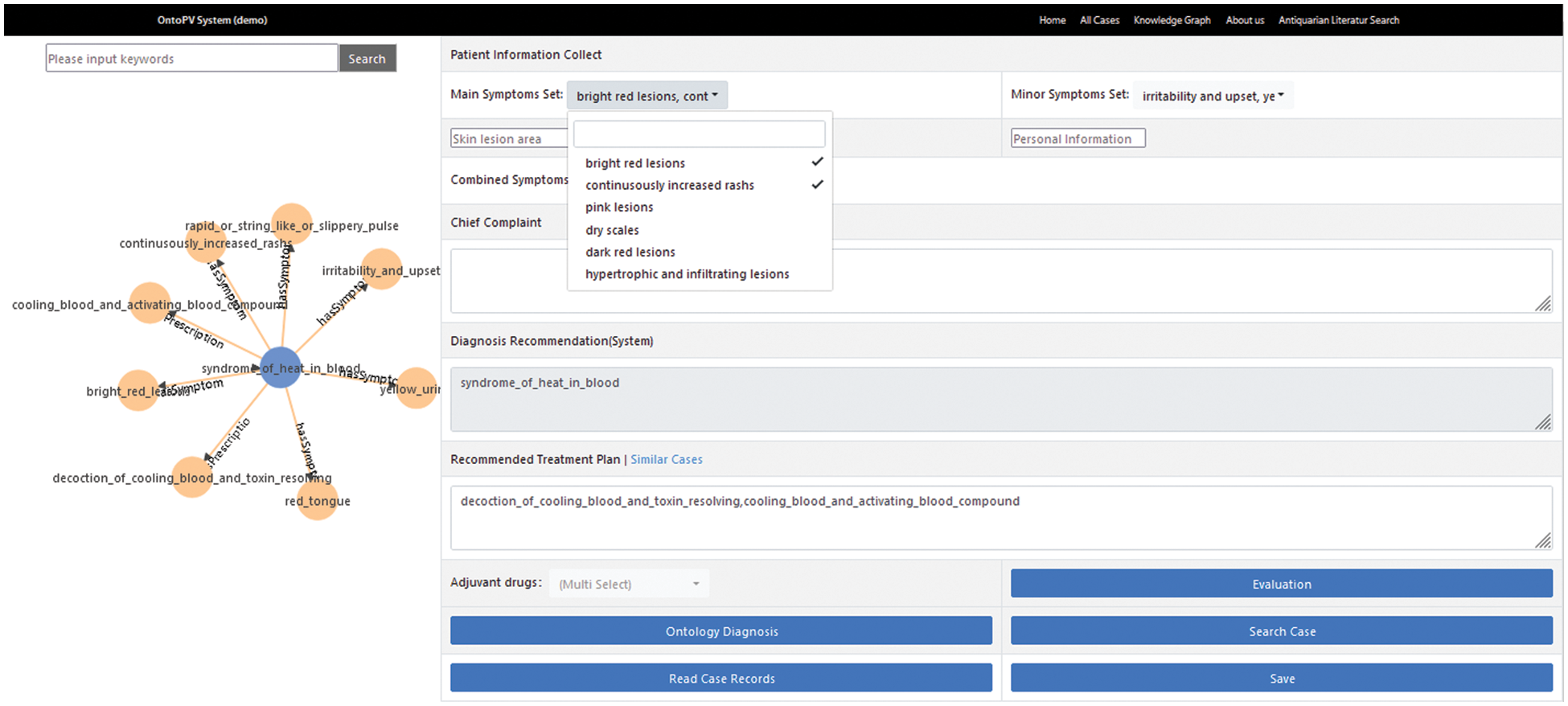
Figure 6: An example of ontology reasoning according to the task 1.3
According to the task 2.2, the same example mentioned in the Fig. 6 for case retrieval is further tested, the no.16-case is matched with maximal similarity and output as the query results, shown in Fig. 7.
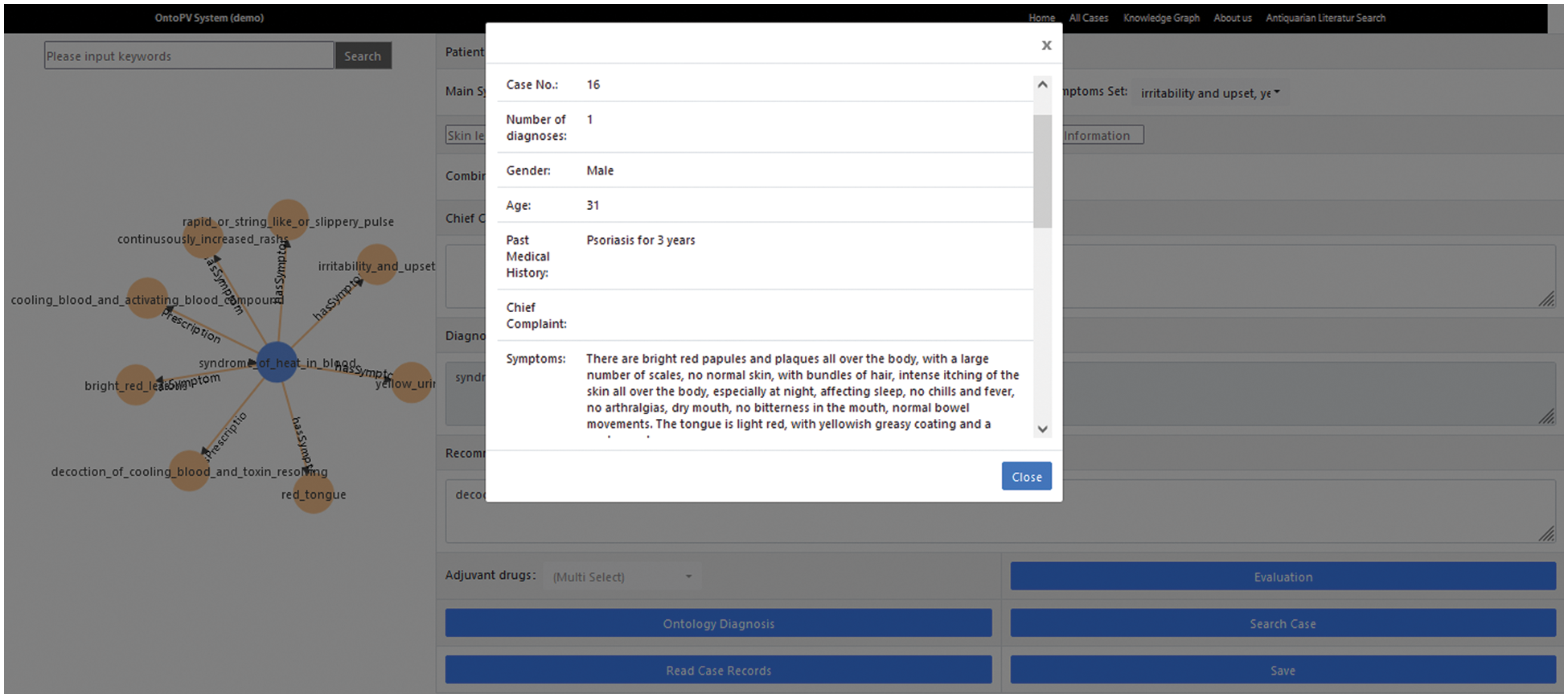
Figure 7: An example for case retrieval
According to tasks 2.1 and 2.3 shown on the left of Fig. 8, another example of reasoning of medication alert according to tasks 1.3 and 2.1 shown on the right, which means if a doctor prescribes a combined drug product of zi dan yin xie capsule with ingredients of danshen root and gastropin for a patient suffering from indigestion, the system will give a prompt. These two drugs may bring about adverse reactions due to having ingredient of aluminum hydroxide, and should be used cautiously. The results are shown in Fig. 8.
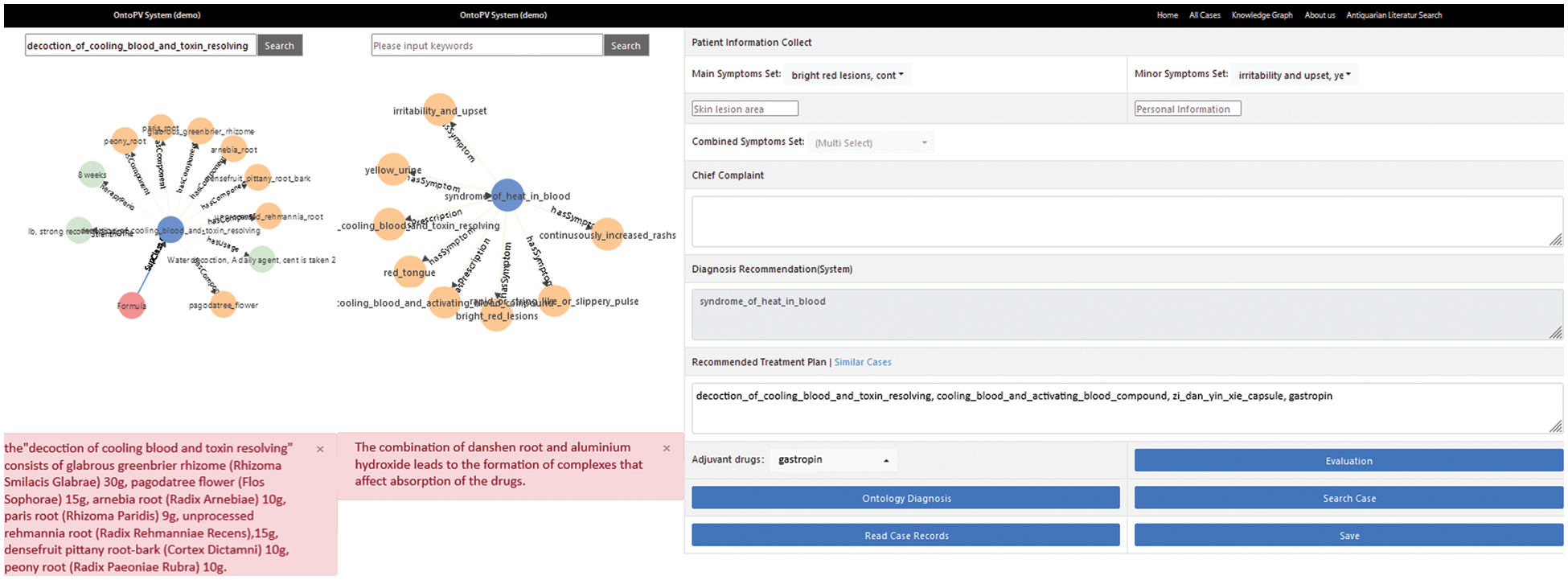
Figure 8: An example of querying the prescription of decoction for blood cooling and toxin resolving
In the experiments, all tasks have been successful performed by 3 experts (senior TCM dermatologists from the Guang’anmen Hospital, China Academy of Chinese Medical Sciences, in Beijing,). They are satisfied with the output results and user experience in task 1.1–1.3, task 2.1, task 3.1–3.3, and agree with the results. Task 2.2–2.3 are assessed as partial approval or as insufficiency, thus it is recommended that system should include more data in the future work. The results are recorded in the following Tab. 3.
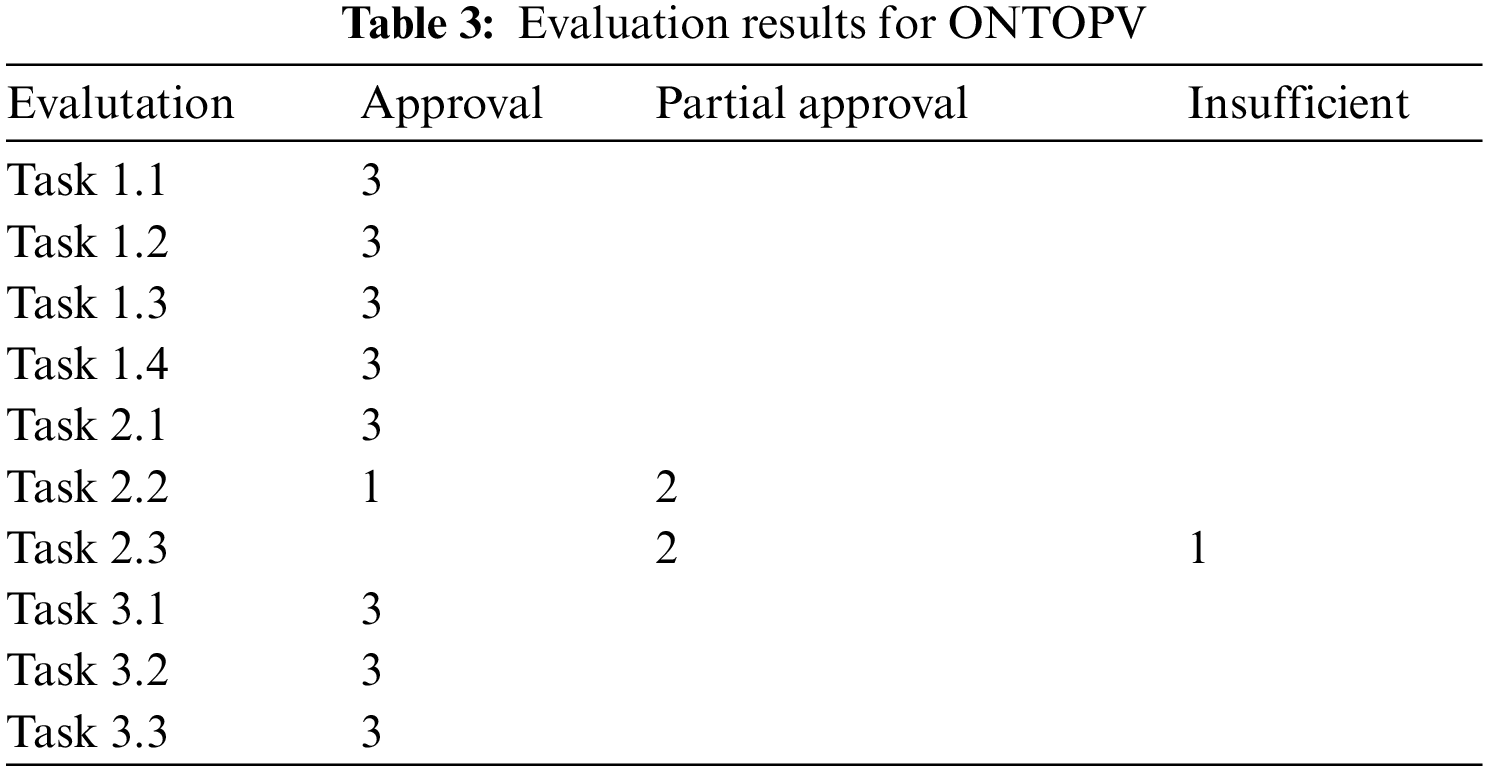
In Tab. 3, “Approval” means the expected effect is achieved or the designed requirements are met; “Partial Approval” means the expected effect is partially achieved or the designed requirements are met to some extent, but additional support or update is needed; “Insufficiency” means the expected effect is not achieved or the designed requirements are not met at all; The number “3” in the table above means: all three experts agreed on the result; The number “2” means: two of three experts agreed on the result; The number “1” in the table above means only one of three experts agreed the result.
According to the assessment results, the future work will mainly be carried out from the following aspects.
The ONTOPV should be extended and upgraded continuously. Firstly, it needs to collect more electronic medical records and cases as well as a drug prescription database, to increase its practicality. Secondly, it needs to extend query and reasoning for all syndromes of psoriasis, as well as to integrate the clinical diagnosis and treatment knowledge of TCM and Western medicine. Finally, this method will be extended to other complications related to psoriasis and other TCM syndromes, for which ontology of Zheng-types and tools are needed to organize and analyze syndromes/Zheng and to extract semantic information from EHR (electronic health care records), according to A. Uciteli, etc. [38].
In the follow-up study, in addition to the above-mentioned points, we are considering to introduce other technologies to strengthen clinical decision-making functions, such as deep learning, combined with the ontology-based knowledge graph to improve the practicality of the system. We will also add some new modules on the existing basis. A module of adverse drug reaction (ADR) has been implemented, and this ADR-module is planned to be used for further research in the future. Besides, we are also considering addition of some new features to ONTOPV, such as a Q&A system based on the knowledge base of psoriasis.
In this paper, a detailed report about a designed and implemented prototype of a decision support system for psoriasis diagnosis based on syndrome differentiation is presented. The system can realize the basic functionalities of data collection, querying, browsing, and navigation, but also support rule-based knowledge reasoning and fuzzy pattern recognition through fuzzy logic. The ONTOPV is intended to provide TCM practitioners with clinical decision support for TCM syndrome differentiation in diagnosis of psoriasis. In addition, it comprises a domain knowledge base of psoriasis, which is developed in the GFO framework with good extensibility. Due to visualization of the knowledge graph and the query interface, doctors can quickly retrieve the needed information from the knowledge base. Furthermore, the system can also provide a module for detection of medication conflicts based on knowledge-based reasoning, which can assist doctors to ensure drug-use safety and reduce drug-induced risks. However, ONTOPV is still at the early stage of development. It is only a preliminary implementation of a conceptual system and not yet a true CDSS. Undoubtedly, there is still a lot of room for growth and we will continue to refine and improve its functionality and usability.
Funding Statement: This work was partially supported by the National Natural Science Foundation of China (No. 82174534), the China Academy of Chinese Medical Sciences Innovation Fund (No. CI2021A05306), and the Fundamental Research Funds for the Central Public Welfare Research Institutes (Nos. ZZ13-YQ-021, ZZ13-YQ-126, ZZ150314).
Conflicts of Interest: The authors declare that they have no conflicts of interest to the report of the present study.
References
1. M. M. Richter, “Introduction,” in The Case-Based Reasoning Technology: From Foundations to Applications,Lecture Notes in Computer Science and Lecture Notes in Artificial Intelligence, Berlin,Heidelberg, New York: Springer-Verlag, vol. 1400, pp. 4–15, 1998. [Google Scholar]
2. J. K. Anastasi, L. M. Currie and G. H. Kim, “Understanding diagnostic reasoning in TCM practice: Tongue diagnosis,” Alternative Therapies in Health and Medicine, vol. 15, no. 3, pp. 18–28, 2009. [Google Scholar]
3. F. L. Lan, “Globalization of TCM: Cultural differences between TCM and western medicine,” in Culture and Knowledge, the Way of Thinking in Chinese Medicine-Theory, Methodology and Structure of Chinese Medicine, Frankfurt a.M., Berlin, Bern, Bruxelles, New York, Oxford, Wien: Peter Lang Internationaler Verlag der Wissenschaften, vol. 13, pp. 24–44, 2010. [Google Scholar]
4. M. Cui, H. Li, X. Hu, L. Jia and S. Yang, “Imagery and traditional Chinese medicine,” Chinese Journal of Library and Information Science for Traditional Chinese Medicine, vol. 38, no. 3, pp. 1–4, 2014. [Google Scholar]
5. L. Yang, X. Z. Zhou, X. Q. Bi, R. S. Zhang, H. Y. Wang et al., “Clinical decision support system on basis of case-based reasoning for traditional Chinese medicine,” Modernization of Traditional Chinese Medicine and Materia Medica-World Science and Technology, vol. 16, no. 3, pp. 474–480, 2014. [Google Scholar]
6. M. D. Peng and T. Peng, “Application of case-based reasoning in the TCM record distribution system,” Modernization of Traditional Chinese Medicine and Materia Medica-World Science and Technology, vol. 11, no. 5, pp. 698–701, 2009. [Google Scholar]
7. Y. Wang, Y. M. Xia, L. Yan, G. K. Wu and J. S. Wang, “Research of Chinese medicine expert system integrated CBR and fuzzy rule-based reasoning,” Journal of Yunan University, vol. 30, no. 2, pp. 195–197, 2008. [Google Scholar]
8. World Health Organization, “Global report on psoriasis,” in WHO Library Cataloguing in Publication Data, Geneva, Switzerland: WHO Press, pp. 1–36, 2016. [Google Scholar]
9. H. Fan, Y. Yan, Y. Zeng and Q. Tian, “Treatment according to syndrome differentiation and external use medicine in the treatment of psoriasis,” Clinical Observation of Shaanxi Traditional Chinese Medicine, vol. 31, no. 8, pp. 1029–1030, 2010. [Google Scholar]
10. Z. M. Li and X. L. Sun, “Traditional Chinese medicine treatment of psoriasis vulgaris with 575 cases of efficacy analysis,” Jilin Journal of Tradition Chinese Medicine, vol. 30, no. 8, pp. 693–694, 2010. [Google Scholar]
11. Y. W. Li, “Dialectic treatment of psoriasis,” Chinese General Practice, vol. 8, no. 12, pp. 956–957, 2005. [Google Scholar]
12. C. Zhou, “Research and application of Chinese medical diagnosis expert system,” M.S. dissertation, Huazhong University of Science and Technology, China, 2005. [Google Scholar]
13. D. Riaño, F. Real, J. A. López-Vallverdú, F. Campana, S. Ercolani et al., “An ontology-based personalization of health-care knowledge to support clinical decisions for chronically ill patients,” Journal of Biomedical Informatics, vol. 45, no. 3, pp. 429–446, 2012. [Google Scholar]
14. M. Martinez-Romero, J. M. Vázquez-Naya, J. Pereira, M. Pereira, A. Pazos et al., “The iOSC3 system: Using ontologies and SWRL rules for intelligent supervision and care of patients with acute cardiac disorders,” Computational and Mathematical Methods in Medicine, vol. 2013, no. 650671. Methods and Models for Diagnosis and Prognosis in Medical Systems, pp. 1–13, 2013. [Google Scholar]
15. C. T. Bau, R. C. Chen and C. Y. Huang, “Construction of a clinical decision support system for undergoing surgery based on domain ontology and rules reasoning,” Telemedicine and e-Health, vol. 20, no. 5, pp. 460–472. 2014. [Google Scholar]
16. M. Alfonse, M. M. Aref and A. B. M. Salem, “An ontology-based system for cancer diseases knowledge management,” International Journal of Information Engineering and Electronic Business, vol. 6, no. 6, pp. 55–63, 2014. [Google Scholar]
17. X. Zhang, B. Hu, X. Ma, P. Moore and J. Chen, “Ontology driven decision support for the diagnosis of mild cognitive impairment,” Comput Methods Programs Biomed, vol. 113, no. 3, pp. 781–791, 2014. [Google Scholar]
18. N. Kalra, R. K. Goyal, A. Parashar, J. Singh and G. Singla, “Driving style recognition system using smartphone sensors based on fuzzy logic,” Computers, Materials & Continua, vol. 69, no. 2, pp. 1967–1978, 2021. [Google Scholar]
19. M. Aly and H. Rezk, “An efficient fuzzy logic fault detection and identification method of photovoltaic inverters,” Computers, Materials & Continua, vol. 67, no. 2, pp. 2283–2299, 2021. [Google Scholar]
20. G. Bucci, V. Sandrucci and E. Vicario, “Ontologies and Bayesian networks in medical diagnosis,” in Proc. 44th Hawaii Int. Conf. on System Sciences, Kauai, HI, USA, pp. 1–8, 2011. [Google Scholar]
21. H. Fujita, I. J. Rudas, J. Fodor, M. Kurematsu and J. Hakura, “Fuzzy reasoning for medical diagnosis-based aggregation on different ontologies,” in 2012 Proc. 7th IEEE Int. Symp. on Applied Computational Intelligence and Informatics (SACI), Timisoara, Romania, pp. 137–146, 2012. [Google Scholar]
22. A. Velu and M. Thangavelu, “Ontology based ocean knowledge representation for semantic information retrieval,” Computers, Materials & Continua, vol. 70, no. 3, pp. 4707–4724, 2022. [Google Scholar]
23. M. Jayalakshmi, L. Garg, K. Maharajan, K. Jayakumar, K. Srinivasan et al., “Fuzzy logic-based health monitoring system for COVID’19 patients,” Computers, Materials & Continua, vol. 67, no. 2, pp. 2431–2447, 2021. [Google Scholar]
24. A. Uciteli, S. Kropf, T. Weiland, S. Meese, K. Graef et al., “Ontology-based specification and generation of search queries for post-market surveillance,” Journal of Biomedical Semantics, vol. 10, no. 1, pp. 1–13, 2019. [Google Scholar]
25. S. El-Sappagh, M. Elmogy and A. M. Riad, “A fuzzy-ontology-oriented case-based reasoning framework for semantic diabetes diagnosis,” Artificial Intelligence in Medicine, vol. 65, no. 3, pp. 179–208, ISSN 0933–3657, 2015. [Google Scholar]
26. S. El-Sappagh, J. M. Alonso, F. Ali, A. Ali, J. H. Jang et al., “An ontology-based interpretable fuzzy decision support system for diabetes diagnosis,” IEEE Access, vol. 6, pp. 37371–37394, 2018. [Google Scholar]
27. D. Palanikkumar, K. Upreti, S. Venkatraman, J. R. Suganthi, S. Kannan et al., “Fuzzy logic for underground mining method selection,” Intelligent Automation & Soft Computing, vol. 32, no. 3, pp. 1843–1854, 2022. [Google Scholar]
28. China Association of Traditional Chinese Medicine Department of Dermatology, “Psoriasis vulgaris (white crust) TCM evidence-based clinical practice guidelines,” Journal of Traditional Chinese Medicine, vol. 55, no. 1, pp. 76–82, 2014. [Google Scholar]
29. Psoriasis Committee of Dermatology and Venereology branch of Chinese Medical Association, “China psoriasis diagnosis and treatment guide,” Chinese Journal of Dermatology, vol. 52, no. 4, pp. 223–230, 2019. [Google Scholar]
30. H. Herre, “General Formal Ontology (GFOA foundational ontology for conceptual modelling,” in Theory and Applications of Ontology-Computer Applications, Springer: Dordrecht, Netherland, pp. 297–345, 2010. [Google Scholar]
31. H. Long, Y. Zhu, L. Jia, B. Gao, J. Liu et al., “An ontological framework for the formalization, organization and usage of TCM-knowledge,” BMC Medical Informatics and Decision Making, vol. 19, no. suppl 2, pp. 79–89, 2019. [Google Scholar]
32. H. Herre, “GFO-Data: Towards an ontological foundation of an integrated data semantics,” in Informatik und Gesellschaft, Frankfurt a. M., Bern, Bruxelles, New York, Oxford, Warszawa, Wien: Peter Lang Internationaler Verlag der Wissenschaften, pp. 1–10, 2016. [Google Scholar]
33. M. Friedman and A. Kandel, “Fuzzy classification and pattern recognition,” in Introduction to Pattern Recognition Statistical, StructuralNeural and Fuzzy Logic Approaches, Series in Machine Perception Artificial Intelligence, London, UK: Imperial College Press, vol. 32, pp. 1–11, 167–217, 1999. [Google Scholar]
34. H. J. Zimmermann, “Introduction to fuzzy sets,” in Fuzzy Set Theory and Its Applications, 4th ed., Boston: Kluwer Academic Publishers, vol. 8, pp. 1–8, 2011. [Google Scholar]
35. L. A. Zadeh, “Fuzzy sets,” Information and Control, vol. 8, no. 3, pp. 338–353, 1965. [Google Scholar]
36. L. A. Zadeh, “Fuzzy logic and approximate reasoning-in memory of Grigore Moisil,” in Synthese, on the Logic Semantics of Vagueness, Dordrecht, Holland: D. Reidel Publishing Company, vol. 30, no. 3–4, pp. 407–428, 1975. [Google Scholar]
37. P. Z. Wang and L. Y. Han, “Applied fuzzy mathematics,” 2nd ed., in Press of Capital University of Economics and Trade Beijing, Beijing, China: Capital Economic and Trade University Press, pp. 1–340, 1998. [Google Scholar]
38. A. Uciteli, C. Beger, T. Kirsten, F. A. Meineke and H. Herre, “Ontological modelling and reasoning of phenotypes,” in Proc. of the Joint Ontology Workshops (JOWO) 2019, Episode V: The Styrian Autumn of Ontology, Graz, Austria, 2019, CEUR Workshop Proceedings, vol. 2518, pp. 1–12, 2019. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |