DOI:10.32604/cmc.2021.014813
| Computers, Materials & Continua DOI:10.32604/cmc.2021.014813 | |
| Article |
Tele-COVID: A Telemedicine SOA-Based Architectural Design for COVID-19 Patients
Department of Information Systems, Najran University, Najran, 61441, Saudi Arabia
*Corresponding Author: Asadullah Shaikh. Email: asshaikh@nu.edu.sa
Received: 19 October 2020; Accepted: 05 November 2020
Abstract: In Wuhan, China, a novel Corona Virus (COVID-19) was detected in December 2019; it has changed the entire world and to date, the number of diagnosed cases is 38,756,2891 and 1,095,2161 people have died. This happened because a large number of people got affected and there is a lack of hospitals for COVID-19 patients. One of the precautionary measures for COVID-19 patients is isolation. To support this, there is an urgent need for a platform that makes treatment possible from a distance. Telemedicine systems have been drastically increasing in number and size over recent years. This increasing number intensifies the extensive need for telemedicine for the national healthcare system. In this paper, we present Tele-COVID which is a telemedicine application to treat COVID-19 patients from a distance. Tele-COVID is uniquely designed and implemented in Service-Oriented Architecture (SOA) to avoid the problem of interoperability, vendor lock-in, and data interchange. With the help of Tele-COVID, the treatment of patients at a distance is possible without the need for them to visit hospitals; in case of emergency, necessary services can also be provided.
Keywords: Tele-COVID; telemedicine architectural design; COVID-19 system design; service oriented architecture; second wave of COVID-19
The COVID-19 outbreak, which started in Wuhan, China, in December 2019, has spread to 203 nations as of March 30, 2020; it has authoritatively been declared a worldwide pandemic. Due to the high number of deaths, people began to realize the severity of the pandemic. With increasing numbers of cases, hospitals were lacking the necessary space for COVID-19 patients and in some countries, hospitals even had to turn COVID-19 patients away due to a shortage of space. It has been noticed that COVID-19 is not dangerous until or unless it is transmitted to the lungs. Once people have a positive COVID-19 diagnosis, many rush to hospitals out of fear, which could be a physiological effect as well. However, it is not usually necessary to hospitalize COVID-19 patients if the disease is not severe.
The first case of COVID-19 was diagnosed on January 19, 2020 [1] and the incidence slowly increased up to March 2020. After March 2020, there was a sudden hike in cases until mid-September 2020. Fig. 1 shows the increase in the COVID-19 worldwide infection rate on a monthly basis [2]. After mid-September 2020, some decline in cases can be noticed but in early October, a slight increase in COVID-19 infection can be seen and this could indicate the start of a ‘Second wave’ [3]. Furthermore, Fig. 2 supported this behavior of COVID-19 in Saudi Arabia where it can be seen a sudden hike in mid of June followed by a sudden decline at the end of the same month, followed by another sudden hike at the beginning of July.

Figure 1: COVID-19 daily cases chart from January 2020 to October 2020 [2]

Figure 2: COVID-19 daily cases chart in Saudi Arabia from January 2020 to October 2020 [7]
To overcome the second wave of the COVID-19 pandemic, telemedicine systems could provide effective solutions to stop its spread. Telemedicine applications are based on technologies that are part of telehealth; they establish a secure communication platform between health professionals and patients.
Extensive work has been published and proposed to describe the need for telemedicine and its potential in crisis and public health emergencies [4]. During the COVID-19 crisis, an essential factor to slow virus transmission is ‘social distancing’ which means lower person-to-person contact. Thus, telemedicine would help in this situation by allowing physicians to examine patients remotely. Telemedicine systems have been developed and used to overcome difficulties of communication between medical professionals and patients using online platforms [5]. Nowadays, the use of telemedicine systems has become essential due to COVID-19 pandemic. Leveraging safe interaction between hospitals and patients through online telemedical applications would be helpful in reducing physical attendance for unnecessary appointments to receive medical support [6]. The proposed Tele-COVID telemedicine application is different from existing architectures as it is integrated with an SOA for every single function. Therefore, all Tele-COVID components are easily extendable to any existing telemedicine application, whether it is similar or dissimilar, and this ensures there is no gap between information transfer from one telemedicine application to another.
The goal of this paper is to propose a new architecture for COVID-19 patients and to investigate possible ways to create the Tele-COVID system architecture for the telemedicine system along with a preferred design selection. The motivation for this paper is the lack of previously published system architectures in this area. In addition, this paper aims to design and develop an algorithm that establishes interconnectivity between current telemedicine applications. Tele-COVID will be an SOA-based system architecture that suggests vendor lock-in, and allows data integration, and interoperability in the area of telemedicine [8,9]. SOA has been suggested as effective in telemedical applications. SOA provides a practical approach to implementing a telemedical system by overcoming the usual technical problems such as interoperability, vendor lock-in, and online interaction. A common way to implement current telemedicine systems is through a web-based application. This involves considering utility and usability requirements in order to design a reliable and secure system.
SOA integrates multiple parts where applications and different technologies and services are implemented in one model as mentioned in [10], for which 50 articles on SOA in telemedicine were selected and analyzed. The research concluded that a typical architecture consists of two subsystems. The first subsystem is placed in the patient’s home and the second subsystem is placed in the hospital or with the healthcare provider. For cases where the healthcare provider may be located in different places, necessary requirements should be considered. For instance, the healthcare provider may be located at the hospital where services can be offered with the necessary equipment. If the healthcare provider is located at home, medical requirements should be able to be met and equipment should be easy to use from home; data and medical services must be able to be delivered. The paper also found that the proper capability of health SOA is related to the use of information technology. SOA as a system considers the heterogeneous interaction between the various components and subsystems, providing interoperability as a typical requirement. SOA is deemed as a useful approach for integrating diverse systems, enabling fixable communication between different applications and systems through the Internet securely [11].
In this paper, we present Tele-COVID telemedicine application, which is based on SOA to avoid the problem of interoperability, vendor lock-in, and data interchange. The proposed Tele-COVID telemedicine application consists of four ends (1) Physician/Doctor (2) Patient (3) Hospital (4) Pharmacy. The first end Physician/Doctor has multiple physicians who are available online via the Tele-COVID application to take a medical history from the patient and decide the severity of the case. In addition, this end provides many services using SOA for example physicians can approve the appointment, notify the patient, notify the hospital, issue a medical prescription, notify the pharmacy, and request an ambulance to transport the patient from home to hospital. The second end allows patients to request an appointment, establish a voice or video conversation, and ask for medication. The third end of the proposed Tele-COVID telemedicine application is Hospital which is integrated to arrange the pickup and admission date for the patients. Finally, the last end of Tele-COVID telemedicine application is Pharmacy which can receive a prescription from the physician for a particular patient with a patient ID, receive payment online or from the patient, and deliver medicines. The communications between all ends are fully protected and secure. Nevertheless, in this paper we also investigate possible ways to develop telemedicine systems for COVID-19 patients to provide recommendation and guidance for healthcare providers. Each service provided by Tele-COVID is SOA-based and we did not use any other services than SOA.
The rest of the paper is structured as follows. Section 2 presents the related work. Section 3 focuses on the requirements for the Tele-COVID application while Section 4 explores the research method used in the study. Section 5 presents the core implementation of Tele-COVID with two main parts, i.e., the implementation of SOA in Tele-COVID and the role of SOA in Tele-COVID. Section 6 discusses the evaluation of the proposed architecture. Security implementation in Tele-COVID is elaborated on in Section 7. Finally, Section 8 offers conclusions and future directions.
When a disease outbreak occurs, there is a lot of pressure and emergency departments may be overwhelmed and relatively chaotic. Many patients seek help at local health care facilities. The uncontrolled flow of sick people seeking medical help poses a critical challenge for ensuring that quality of care is maintained, particularly during a pandemic or particular crisis. Importantly, forward triage is defined as the process of determining what the patient’s condition requires before admission to an emergency department. Developing a telemedicine program requires resources, sufficient funding, and executable guidelines. With Telemedicine, several challenges that are faced in health care relating to a patient’s condition can be solved. It not only offers a way to overcome excessive patient flow, but it can also make the work of the healthcare providers more manageable and less risky [12]. Medical practitioners hoping to provide clinical care services via telemedicine have encountered several regulatory and legal challenges including multijurisdictional issues, challenges with getting reimbursement for services, and licensure issues.
Research [13] proposes the need to implement telemedicine systems which focus on handling the needs of poor-acuity of patients with disease exposure concerns. It also includes new insights into a rapidly changing epidemic, taking into account the radius of its infection and secondary sources that relay information on mortality and health care. It is apparent that telemedicine is well suited and prepared to address several devastating situations arising due to the COVID-19 outbreak, and it has been suggested that telemedicine systems should be considered as a tool for health care providers. Some regard the utilization of telemedicine as being restricted to addressing the current pandemic; there is a view that telemedicine’s utility will be negligible once the pandemic comes to an end. The massive use of telemedicine lacks randomization and speed. Challenges in providing health care services are not only apparent for those affected by COVID-19; they are also discernible for patients with trauma, patients diagnosed with depression, and people diagnosed with an acute illness requiring doctors and nurses to be safeguarded, and other related health practitioners. Researchers in [14] examined the lessons learned by various telemedicine community service providers and adopted the right measures. Studies have also considered the huge implications of conversion to the telemedicine concept its usefulness as an efficient intervention to support social distancing in a healthcare setup. Results have suggested that service providers involved in telemedicine practice should stop regarding telemedicine simply as a connectivity tool. In broadening the concept, future healthcare systems will learn lessons from today’s bad experiences.
The research [15] has pinpointed feasibility data and also highlighted how video-enabled telemedicine can impact patients and providers. It has analyzed how COVID-19-affected individuals have been impacted by telemedicine, through a case study of a large health system. Another goal has been to illustrate the transformational impacts of the COVID-19 pandemic on telemedicine-driven healthcare services at the center of this pandemic. Major obstacles to wider adoption included the fact that telemedicine technologies do not feel comfortable to patients, there is limited reimbursement, and there are few providers. Basically, outside rural-based medicine, there were limited compelling situations for the replacement of what the report referred to as in-person care. Paper [16] assessed the use of telemedicine on patients and determined if it can help minimize COVID-19 transmission. It also assessed if medical instruments used remotely for telemedical treatments are good enough. Moreover, the research properly examined if telemedicine can work as a safer option for non-infected patients who cannot physically come to hospitals for checkups. The use of telemedicine for optimal care can provide a powerful source ‘multiplier’; that is, telemedicine can effectively attend to patients much more quickly than when patients are physically present. Specific medical instruments, such as thermometer pressure instruments, can be used remotely by patients without a medical personnel’s physical presence.
There are specific examples of utilizing telemedicine to treat patients with some diseases. One example is mentioned in [17] where researchers examined whether the pandemic’s public health issues can increase the national conversations regarding a wider integration of telemedicine for medical care routines even in non-crisis situations. It also tried to critically examine whether telemedicine can be used for liver-related diseases, particularly for those living in less populated areas. The results showed that: (a) the outbreak of severe respiratory diseases such as COVID-19 has improved delivery of telemedicine, making it a safe practice for public health and maintaining social distancing measures; (b) although presently limited in use due to licensing restrictions, patients with liver-related diseases can still be adequately cared for through telemedicine. Other research is presented in [18]; it concerns the risk factors that predispose urological patients to a severe outcome from COVID-19 and possible contact-free continuity of care. It can be deduced that most urology patients prefer telemedicine consultations as a solution for continuity of care in the face of COVID-19, as they are at risk of a poor outcome if they catch the disease.
Further, the challenges faced with ophthalmology relate to staffing, triage, and maintenance of patient-physician engagement. In setting up a teleophthalmology program, the workflow-visit cycle needs to be well integrated. Here, the research advocates for a conceptualized future state, then the establishment of the right technology for workplace workflow [19]. Besides this, early diagnosis can lead to reduced burden of the disease, as well as reducing death rates and fostering quality of life in general. This research explored text messaging and images through social media for instant communication for early diagnosis and subsequent follow-up to bring about effective oral treatment for Covid-19 patients. The novel coronavirus has catalyzed the adoption of telehealth for the transformation of health care delivery systems. This telehealth approach is ideal for meeting the demands of in-patient care while also reducing the spread of the virus [20].
Paper [21] investigated the need for a robust telemedicine program to maintain safe, efficient, and effective orthopedic care during the pandemic. The qualitative approach was employed to assess effective treatment in the orthopedic division by creating a checklist to establish which patients require in-person visitation and which can be managed using telemedicine. There were two goals of this study: (1) to provide practical tips and identify barriers for doctors when implementing telemedicine in the context of a pandemic; (2) to identify factors related to telemedicine’s high rates of adoption for successful orthopedic care continuation even during Covid-19. Telemedicine can help healthcare providers attain almost fifty percent of the expected standard clinical volume in just two weeks. It can be said that telemedicine is important to facilitate the safe and effective progression of orthopedic care even during such a challenging period while focusing on decreasing infection risks and the burden of disease for the already loaded healthcare system. The authors in [22] state that virtual orthopedic examination is limited, as palpation and dynamic testing are absent. There were reported challenges with the implementation of virtual orthopedic appointments, especially among the elderly population. A similar study was carried out in Norway and limitations of virtual orthopedic examinations, in terms of, for example, palpation, were identified. The proposed solution in this research would be to conduct a virtual orthopedic examination through Magnetic Resonance Imaging (MRI).
There is an increasing need for the adoption and operation of telemedicine services in offering palliative care to COVID-19 patients. This research provided relevant insights for supporting palliative care practitioners and relevant program leaders in providing optimal care via telemedicine. It also offers detailed insights to guide health caregivers in areas relating to the nature of telemedicine, patient factors, and clinician factors, majorly in outpatient settings. Telemedicine is an established method for delivering palliative care to people classified as vulnerable. Proper preparation, practice, and patience will allow for effective implementation of telemedicine [23]. Research in [24] studied the lack of innovation and digitalization in Italy’s health care system and the impact of poor management during the pandemic. The study summarized how there is a need for the Italian Health service system to evolve and adopt a modern health care model that will be effective for future emergencies. Findings from paper [25] indicate that health care professionals and organizations have successfully adopted telemedicine practices. The presence and use of Telemedicine apps have helped to reduce the spread of the virus by indicating likely infections and providing verifiable evidence and updates on the COVID-19 pandemic.
Service-oriented architecture presents a software design where several services can be used as components by application components with the help of communication protocols. SOA is also used in the telemedicine monitoring system which is the combination of wireless monitoring devices, and health services information platforms. This monitoring system also adopts the open services gateway initiative (OSGi) platform which can offer several services like automatic dynamic adjustment of patients. Hence, patients with chronic diseases can be treated 24/7 [26].
Article [8] explains the importance of SOA in the area of telemedicine. The major idea in the research is that by using SOA and also external web services, the aspects relating to the interoperability of different systems and technologies involved in telemedicine can be resolved. This paper establishes that, currently, telemedicine systems require networking technologies to be integrated with health care processes. However, this raises interoperability challenges for these systems, which is evident in in-patient monitoring, diagnosis, decision support, and in terms of the communication system needed at the healthcare facility’s point of care (PoC). In addition, this problem is seen when a given clinic ‘A’ cannot interoperate with clinic ‘B’. As such, retrieving the patients’ history can be a challenge. Telemedicine systems have been noted not to easily allow integration of the clinical data as required by other organizations’ infrastructures. This problem is a result of differences in the technical standards and information interchange used by various vendors in making their telemedicine systems. The architecture design of the system was developed with the support of the .Net layer presentation, the data layer, and the business logic layer.
Article [4] extends previous work on ‘The Role of SOA in Telemedicine Healthcare Systems’ by looking into how users can address the issue of vender locking, interoperability, and data integration for telemedicine systems. The authors of the article considered the next-generation Tele-wound architecture system in their implementation. According to these researchers, the Tele-wound application follows critical procedures that are fundamental in healing leg ulcers using a multimedia messaging service (MMS). The nurse takes pictures of the wound or leg ulcer and uses MMS to send it to the database. The patient can interact with the nurse by contacting the facility where the Tele-wound application is utilized or by opening the Tele-wound website for him/herself to book an appointment. There are two main parts to the Tele-wound system, and these relate to the user’s side and the physician’s end. From the patient’s end, the application is responsible for data collection; images are collected and transmitted to the doctor’s end. The contact of these two ends is complete when the MMS or email is sent and received.
Paper [27] presented experiences from a collaborative, integrated, distributed, large-scale enterprise healthcare information system (HIS) that was executed in the infrastructure of the National Taiwan University Hospital (NTUH). The new healthcare system (HIS) should be able to integrate all the required components and be able to accommodate changes and technological advancements. Therefore, in NTUH, the focus of the designers of the health information system focused on a system that could avail of an educational healthcare environment in an electronic format. Therefore, the HIS focused on IIS development and implementation since the new version of IIS has unlimited scalability, was low cost, and could be compatible with future systems that could make it easier to undertake upgrades and improvements. The multitier IIS had a superior design and was robust in terms of its performance index, CPU, and economies on memory.
Paper [28] introduced telemedicine as the opportunity for the health sector to develop information and communication technology (ICT) that makes healthcare service delivery easier and faster. It adopted a methodology that integrated Model Driven Architecture (MDA) with SOA to foster telemedicine in a promising way in some third world countries and the focus was to ensure that a large amount of functionality was transported to web services. Telemedicine applications could interoperate with other applications and it could allow remote connections to access less-developed communities. Being based on the MDA concept allowed the designers to capitalize on the telemedicine business process and this facilitated interoperability with several other applications on platforms such as tablets and cell phones in some remote areas, to involve technical platforms, different health personnel, conduct analyses, and operations. The collaboration between health care providers and users was significantly improved via telemedicine services to remote areas even in developing countries and this kind of development is strategic to address epidemics such as the Ebola virus in African countries.
Electrical impulses stimulate the regular functioning of the human heart, i.e., how ventricles and atria rhythmically contract, to facilitate oxygenation of other organs, as mentioned in [29]. These impulses need to be monitored to prevent cardiac activity from possible faults leading to arrhythmias and heart failures. Medical equipment includes the electrocardiogram (ECG) which collects relevant data with the use of skin electrodes that are placed on the chest and limbs. The information is transmitted to the specialist through a web service and a real-time diagnosis is provided along with medication. The main focus is to ensure that heart activity is controlled and there is an emergency service in case there is any form of cardiac pathology. The experimental results show good performance and the measurement system is valid for use in practice due to the expected results. The researchers concluded that the system’s fault-tolerant diagnosis algorithm allowed the system to acquire information regarding the reliability of the final results that comply with the correct detection capability of the ECG system.
Researchers in [30] came up with an ontological approach in which they designed an integrated approach for mobile telemedicine (MTM) services based on SOA. This ontological approach has a common platform and the meta-ontology integrates common procedures and vocabulary to register and describe the MTM services. This eliminates the necessity for mediation and challenges related to semantic heterogeneity allowing for interoperability between different MTM services regardless of the implementation of the underlying structure. Meta-ontology is the key component of this platform because it is responsible for the service registration process and discovery between applications operating in a covered environment that can be medical, mobile, or environmental dynamic traits. The authors highlighted that SOA deals with web service implementation, but they noted that it can support the main infrastructure for a complete MTM platform. However, SOA would fail to satisfy the full automation and interoperability requirements. SOA provides a low-quality syntactic service description since it relies on traditional web services and these would impede the automation of the system’s service interaction and discover when addressing difficult terms. Therefore, these SOA limitations necessitated a merger between semantic web and web services architecture to form semantic web services. In this platform, all service users are registered, and the platform allows bidirectional service discovery. The services that one requests are well-described with the use of an SWS description framework because it allows optimization of the process of service to meet the standards of the described MTM platform.
Paper [31] introduced a proposal to integrate an information system that has a robotic device in its control system. The proposal is aimed at accessing the use of telemedicine for physiotherapy rehabilitation. Telemedicine has been reported to be effective in training, and the querying and diagnosis of patients. However, a telemedicine process through which a specialist synchronously facilitates physical rehabilitation for clients has not been evaluated. The article assessed an SOA approach. SOA is used to implement health care services that are teleoperated applications using physical devices that monitor the system. Therefore, the process of rehabilitation is monitored, not just by training or querying but through the physical implementation of the rehabilitation processes. The SOA system in this research had a multi-degree-of-freedom (DOF) motion assistance robot, a VR interface to support the clients/patients, and importantly, there was an asymmetrical master-slave motion assistance training strategy that was referred to as self-motion control.
The literature explained above presents SOA with several services, however, data interchange, interoperability, and automatic transmission of data from one telemedicine architecture to another architecture is always an important concern that is hardly addressed in the literature. Tele-COVID architecture is equipped with services that are uniquely designed with SOA services that can easily handle the transmission of data from one telemedicine to another telemedicine architecture that can be heterogeneous or homogenous. In addition, the treatment of COVID-19 patients is available round the clock with help of Tele-COVID which is available in the form of web and mobile applications.
3 Tele-COVID-19 Application Requirements
Coronavirus is a pandemic and it has two phases: (1) the Interpandemic Phase, and (2) the Pandemic Alert Phase. In the Interpandemic Phase, there is an animal transmission and very little human transmission. Meanwhile, in the Pandemic Alert Phase there is disease transmission from human to human which can go on to become widespread from human to human; this intense period represents the peak and after that there may be a post-peak period and a post-pandemic period. In this section, we discuss the requirement specifications for our developed mobile and web based Tele-COVID application which will work for Phase Two, i.e., the Pandemic Alert Phase. The Tele-COVID application can help coronavirus patients to seek medical help without visiting a hospital. The first and foremost requirement of the Tele-COVID application is the home test.
A patient needs to go through some basic questions using the home test functionality. The answers given in the home test will ascertain whether the patient needs further medical care or not. The results of the home test will be in the form of ‘Negative’ or ‘Positive.’ If the result is negative, the application will advise the patient to stay at home or self-quarantine. Alternatively, the option to book an appointment with the doctor will be enabled automatically. Fig. 3 shows the basic flow chart for the application.

Figure 3: Tele-COVID-19 basic flow chart
Tele-COVID is consists of four ends (1) Physician/Doctor (2) Patient (3) Hospital (4) Pharmacy and it will be deployed in all four ends, therefore, every communication will be undertaken through Tele-COVID-19 telemedicine application. The requirements are divided into functional and non-functional requirements.
3.1 Tele-COVID Functional and Data Requirements
• Patients will fill in the questionnaire through a home test to establish the severity of the infection.
• The patient will request an appointment.
• The physician will approve the appointment and the patient will be notified through the application.
• The patient will start discussing the symptoms with the physician.
• The discussion above could be done using a video or voice meeting.
• The physician will decide if the patient can be treated at home. If the patient does not have serious symptoms, then the physician will advise the patient to stay at home and issue him some basic medication if required through a medical prescription.
• The medical prescription will be sent to the pharmacy, where Tele-COVID is installed and the pharmacy will deliver the medication through a delivery service arranged by the pharmacy. Medical prescriptions will be paid online.
• If the patient is in a serious condition due to coronavirus, the physician will issue a request for a hospital to deploy an ambulance to transport the patient to the hospital.
3.2 Tele-COVID Non-Functional Requirements
• The Tele-COVID application is equipped with a rich user interface that is very easy to use for the actors of the system, i.e., physician, patient, and pharmacy representative, allowing them to communicate with each other smoothly.
• The Tele-COVID application gives a fast response, has good throughput, and responds in a timely manner.
• The Tele-COVID application has the ability to maintain an optimal level of performance if any fault or problem occurs.
• The Tele-COVID application provides an error-free environment to its users, so the application contains the capability to re-establish the connection after the error occurs.
3.3 Testing of Functional and Non-Functional Requirements of Tele-COVID
Functional requirements are associated with the functions of the system that often shows the expectations on the testability that further needs to produce input and output to generate the test data. To ensure the functional requirement of Tele-COVID, Test-driven development (TDD) has been used since it relies on the recurrence of the short development cycle. Several test cases were developed that were specific to each SOA-based service, then the code was amended so that the results can be seen about the pass test cases. Furthermore, Tele-COVID was deployed to all four ends for functional testing, where each end submitted feedback regarding services offered to them. Hence, the functional requirement was tested and evaluated thoroughly before the tele-COVID came into practice.
The measurement of non-functional requirements is the most critical part of any architectural design and the success or failure is entirely dependent on it. In order to ensure the non-functional requirement of tele-COVID, several approaches were selected that are requirement elicitation, requirement quantification, requirement prioritization, and requirements assessment. The first and foremost important non-functional requirement of tele-COVID is availability, where we ensure that tele-COVID is available 24/7 to COVID patients as the second wave is approaching. The second non-functional requirement is reliability, which shows the trust of the patient, so they can enter their private information to approach the physician. Since tele-COVID is registered with a national ID, therefore, the reliability is well achieved. The third requirement is performance, which shows how fast COVID patients can receive the response and get an appointment. The final requirement is safety, which optimizes system safety in design, development, and maintenance. All these required are tested and evaluated against approaches as shown in Fig. 4. Each approach is evaluated against each tele-COVID non-functional requirement to gain the trust of the users. This complete process is shown in Fig. 4. Moreover, the application was also deployed to all four ends to submit their feedback the same as functional requirements.

Figure 4: Tele-COVID approaches for non-functional requirements
An initial bibliographical research approach was conducted in conjunction with a review of the literature. Subsequently, both qualitative and design research methods were employed. First, a survey was conducted with the primary aim of aggregating data to be used for a comparison between our proposed system architecture and various preexisting architectures. This allowed the analysis of vendor locking, integration of data, and interoperability in the domain of telemedicine systems. Enhancing the system of telemedicine architecture was adopted through a quantitative approach such that it:
• Identifies related telemedicine systems
• Examines specific Tele-COVID applications if they are available
• Proposes a novel architecture for telemedicine systems that solve the problems of vendor locking, data integration, and interoperability
Additionally, we adopted design research, an approach to problem-solving that helps address vendor locking, data integration, and interoperability through designing a telemedicine architecture solution. Therefore, the following design research procedures, as shown in Fig. 5 were employed:
• Knowledge Flows: The knowledge flows in our domain stem from previous studies on telemedicine system architectures that have addressed problems with vendor locking. That prior knowledge helps lead to innovation in this field.
• Process Steps: Mechanisms that aid in creating innovation through design research, which are as follows.
Awareness of Problems: The problem of data interoperability, especially with the increase of distributed telemedicine systems, is apparent after a thorough literature review in the field of telemedicine.
• Suggestion: At this stage of the process, we introduced a solution based on services-oriented (SOA) architecture and web services for telemedicine application that is significant for analysis of Tele-COVID systems through employing integration and platform connectivity.
• Development: At this stage, our application will be published to the web as well as being compiled for Android devices. It will collect a patient’s description and store that as text into databases.
• Evaluation: The Tele-COVID system will be deployed in a hospital so that its quality can be determined.
• Conclusion: The results before and after the Tele-COVID system has been deployed will be compared.
Outputs: Each step in the process produces a unique output. A researcher can transition from development (3rd step) to awareness (1st step), altering the output at any point in the process as a result of this methodology.

Figure 5: Design research methodology
5 Implementation of Tele-COVID’19
In the world of telemedicine, there are thousands of telemedicine applications currently functioning in the market, and similar architectures are also proposed for patient monitoring and treatment systems but Tele-COVID is somewhat different to the existing architectures as it is integrated with an SOA for every single function. To ensure a robust and flexible telemedicine architectural design, we reviewed and analyzed several existing applications and came to the conclusion that there are only a few that are based on SOA [32–34]. When using an SOA-based design, Tele-COVID components are easily extendable to any existing telemedicine application, whether it is similar or dissimilar, and this ensures there is no gap between information transfer from one telemedicine application to another. The Tele-COVID architectural design makes the problems of interpretability, vendor lock-in, and data integration obsolete. The problem of consistency that may occur due to data interchange with another telemedicine network was also addressed. Fig. 6 gives the main architectural design of Tele-COVID. Since it is only designed to treat the COVID-19 patients, the target audience will be limited to corona virus.

Figure 6: SOA-based Tele-COVID-19 architectural design
Tele-COVID has two modes of communication: as a mobile application for android phones or as a web-based application that can be used through a browser. Both modes are fully equipped with compatibility, i.e., the connection can be established from mobile to mobile and mobile to web-based application or vice versa. The mobile and web-based architectures use telecommunication (GSM/4G) and Internet technology and their significant segments are subject to service availability. The design also assures the availability of medical staff all the time through internet access. If a physician is on duty, it is mandatory for him/her to remain logged in to Tele-COVID while he/she is on duty and his/her location can also be tracked. This facility is required to help COVID patients in any part of the world.
The Tele-COVID design was divided into two different layers, i.e., the presentation layer and the business layer. The presentation layer addresses the presentation logic, the point at which the data/information is exchanged between the physician and the patient. The patient will request an appointment with the physician through the Tele-COVID application. Once approved, the 4G or internet web-based connection will be established between the physician and the patient. A number of physicians will be available and online via the Tele-COVID application. The physician will take a medical history from the patient and decide the severity of the case; if necessary, the physician may request an ambulance from the hospital to transport the patient from home to a COVID ward. Alternatively, if the condition is not serious, the physician may advise the patient to self-isolate. Simultaneously, the physician can write a medical prescription to the patient through the Tele-COVID application which will automatically be received by a pharmacy; the pharmacy can then arrange delivery. Payment for the medication can be made online or through a delivery agent.
The second layer is a business logic layer which relates to the communication between several modules, i.e., external web services and 4G providers. Tele-COVID is deployed for smart phones using the android operating system and for a web-based application. The web-based application is programmed using the Visual Studio.Net framework with the Internet Information Server (IIS) and MySql as a database. Once the connection is established between a physician and a patient, their entire voice/video conversation will be recorded and stored in the database and physicians may look at the patient’s history at any time in order to be able to provide proper medical care.
The application offers two main services: ‘InsertData’ and ‘GetData.’ ‘InsertData’ is utilized to enter the information into the relevant databases (physician prescription) and ‘GetData’ is utilized to collect the information. In order to utilize these services, the doctor needs to log in first. After logging in a medical prescription can be added into the application. The same information can be accessed and altered from some other telemedicine application with specific limitations. This methodology resolves the issue of interoperability as the information can be exchanged between comparable and unique telemedicine applications. The proposed Tele-COVID architecture removes the location barrier and can be used from any part of the world. This will improve the proficiency of medical services for COVID patients, normalizing electronic data exchange.
5.1 Implementation of SOA in Tele-COVID
SOA provides different services and through these services, communication can be established in order to exchange data from one system to another without affecting any data attribute or entity. There are several web service standards available in the literature, such as Hypertext Markup Language (HTTP), Simple Object Access Protocol, Universal Description, Discovery and Integration (UDDI), Extensible Markup Language (XML), and Web Services Description Language (WSDL).
In the Tele-COVID architecture, several web services were created for four described ends, i.e., physician/doctor, patient, hospital, and pharmacy. Tab. 1 shows four SOA services for patients with the server response. Using these SOA services, patients can request an appointment, establish a voice or video conversation, and ask for medication. Tab. 2 describes the services for the physician where they can physically approve the appointment, notify the patient, notify the hospital, issue a medical prescription, notify the pharmacy, and request an ambulance to transport the patient from home to hospital. Tab. 3 explores the services for the hospital which include patient pickup from home to the hospital, inserting the date in the Tele-COVID application, and admitting the patient to the COVID-19 ward. Finally, Tab. 4 elaborates on the integrated SOA services for the pharmacy. The pharmacy can receive a prescription from the physician for a particular patient with patient ID, receive payment online or from the patient, and deliver medicines.
Table 1: Integrated SOA service in Tele-COVID for COVID patient

Table 2: Integrated SOA service in Tele-COVID for physician

Table 3: Integrated SOA service in Tele-COVID for hospital

Table 4: Integrated SOA service in Tele-COVID for pharmacy

Each service will be activated automatically with the proper server response by the designed application. External web services were used in our designed application to avoid the issue of interoperability for heterogenous telemedicine applications. SOAP is used for the XML message binding protocol to transport the secure message.
5.2 The Role of SOA in Tele-COVID
Most telemedicine applications are designed for heterogeneous environments and due to their diverse nature, data interchange between dissimilar telemedicine applications is a challenging task. For example, there are two clinics, clinic ‘X’ and clinic ‘Y’. Clinic ‘X’ is not able to retrieve the data through telemedicine applications due to interoperability issues and physicians are forced to start the process from scratch with patients. This increases the cost of physically examining the patient and requires the physician to spend time understanding the history of the patient. Currently, most hospitals and clinics maintain their patient records locally and do not trust physical investigations undertaken anywhere else. Hence, there is a need for a telemedicine system that can specifically be used for COVID patients which integrates, arranges, and organizes the data in such a way that individuals working in healthcare services can obtain information regardless of the environmental factors. As per the medical handbook [35], communication between dissimilar organizations must be managed in a decent and proper manner and there should be a method for integrating the patient’s data, so the physicians can access the patient’s history even when an investigation has been undertaken in a different hospital.
SOA plays a vital role in addressing the concerns discussed above. By using SOA in tele-COVID, the design is integrated with technical goals and common business drivers. The interface has been programmed so that it is compatible with interoperability protocol and therefore, the first and foremost benefit that is offered is ‘Reuse.’ All created services listed in Tabs. 1–4 are reusable in any other heterogenous telemedicine application. The second benefit is ‘Efficiency’ that helps Tele-COVID allow its SOA services to integrate with or be implemented in any new or old telemedicine application. This feature allows the data to be joined up instead of requiring it to be created from scratch. The final benefit is ‘loose coupling’ and through this feature, Tele-COVID interconnects its features, services, and components to any other system, so those features, services, and components can be used by different heterogenous telemedicine applications.
The services utilized in our design are fundamentally executed as a software component that depends on an instance and furthermore, interrelates with Tele-COVID through a loosely coupled message-based correspondence model. The concept behind SOA services is, moreover, the same as the concept for Component-Based Software Development (CBSE); however, each component is integrated as an independent web service. Fig. 7 illustrates the interaction of tele-COVID services with WSDL through messaging protocols using SOAP, HTTP, MIME, and SSL.

Figure 7: Tele-COVID-19 requested web services through WSDL
In this section, the advantages of the Tele-COVID architecture are described along with its features. Since Tele-COVID is an SOA-based application, the main advantage is the reuse of components among organizations without adopting any expensive technologies. The use of WSDL enables the communication protocol and messaging formats to standardize the communication between external web services and Tele-COVID applications. To undertake successful communication between two different telemedicine applications, both ends need to comprehend XML to corroborate information at various stages. Web services-metadata exchange helps to identify the data and its substance type from another telemedicine application. By utilizing these web services, it is possible to determine and resolve data exchange issues; on the other hand, at least two diverse telemedicine applications from different vendors utilize these services, and thus, the application is ready to communicate and exchange the data. With this phenomenon, the user is not reliant on a single vendor. Each service provided by Tele-COVID is SOA-based and we did not use any other services than SOA.
Moreover, the Tele-COVID application has number of features that are very easy to use for corona virus patients. Fig. 8 shows the front menu of the application with all the features available to a COVID patient. The first and foremost feature of the application is the ‘Home Test.’ With this feature, a patient who suspects they may have COVID needs to fill out a questionnaire using the ‘Home Test’ feature and the application will suggest whether or not they need to seek an appointment. Fig. 9 shows the ‘Home Test’ feature integrated in the Tele-COVID application. This feature provides reassurance to the patient at the initial stage if the result is negative and the application does not recommend an appointment. The second feature is to book an appointment with the doctor through the feature ‘Book a doctor,’ if the patient has symptoms, and the Tele-COVID application suggests seeking the advice of a doctor. To book an appointment, the user needs to enter all the details required by the application and then a list of doctors becomes available for potential selection. Fig. 10 shows the feature for booking an appointment with the desired doctor. Since the doctors are allocated according to area in the city, the closest doctor is notified for an appointment, based on the patient’s location. Fig. 11 shows the location of doctors according to area and each doctor is capable of handling a number of patients. If the doctor is busy with other patients, then the next available doctor is assigned for an appointment by the application automatically. The third feature is to ‘Track Medicine’; this feature is available to a patient if the doctor has prescribed medication to the patient. Once the doctor issues a medical prescription, the details are entered into the Tele-COVID application and the pharmacy is notified. The last feature allows the doctor to call an ‘Ambulance’ if the patient’s condition is serious and requires hospitalization. The patient can check through Tele-COVID application about the ambulance service ordered for possible pick up from the patient’s residence.

Figure 8: Front menu for the Tele-COVID-19 application

Figure 9: Tele-COVID-19 ‘Home Test’ feature

Figure 10: Tele-COVID-19 ‘Book an Appointment’ feature
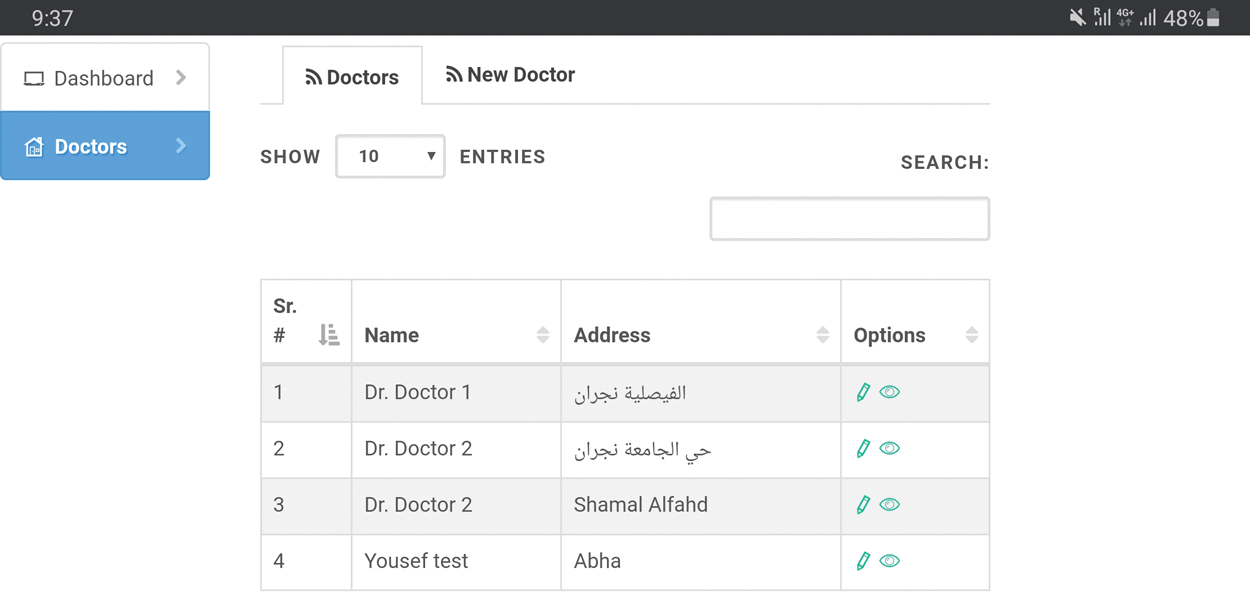
Figure 11: Tele-COVID-19 doctor location
Tele-COVID was deployed to all four ends: (1) physician/doctor; (3) patient; (4) hospital; (2) pharmacy to test the application in a city hospital. Tab. 5 shows the Tele-COVID input data response for the first 20 patients where Tele-COVID response time, hospital response time, and pharmacy response time can be observed. However, due to privacy issues, it is not possible to disclose the personal data of these 20 patients. Tele-COVID provided quite a rapid response at all four ends; for example, patient P101 requested an appointment on Mon 24 Aug 2020 7:23 AM and the appointment was approved on the same day, Mon 24 Aug 2020, at 11:50 AM. Patient P101 communicated with the doctor the next day, Tues 25 Aug 2020, at 9:06 AM. The column ‘Tele-COVID response time’ is a connection establish time between patient and the doctor. The hospital response time was also on the same day, Tues 25 Aug 2020, at 09:25 AM, given that the patient required an ambulance or admission to the hospital.
Table 5: Tele-COVID input data response
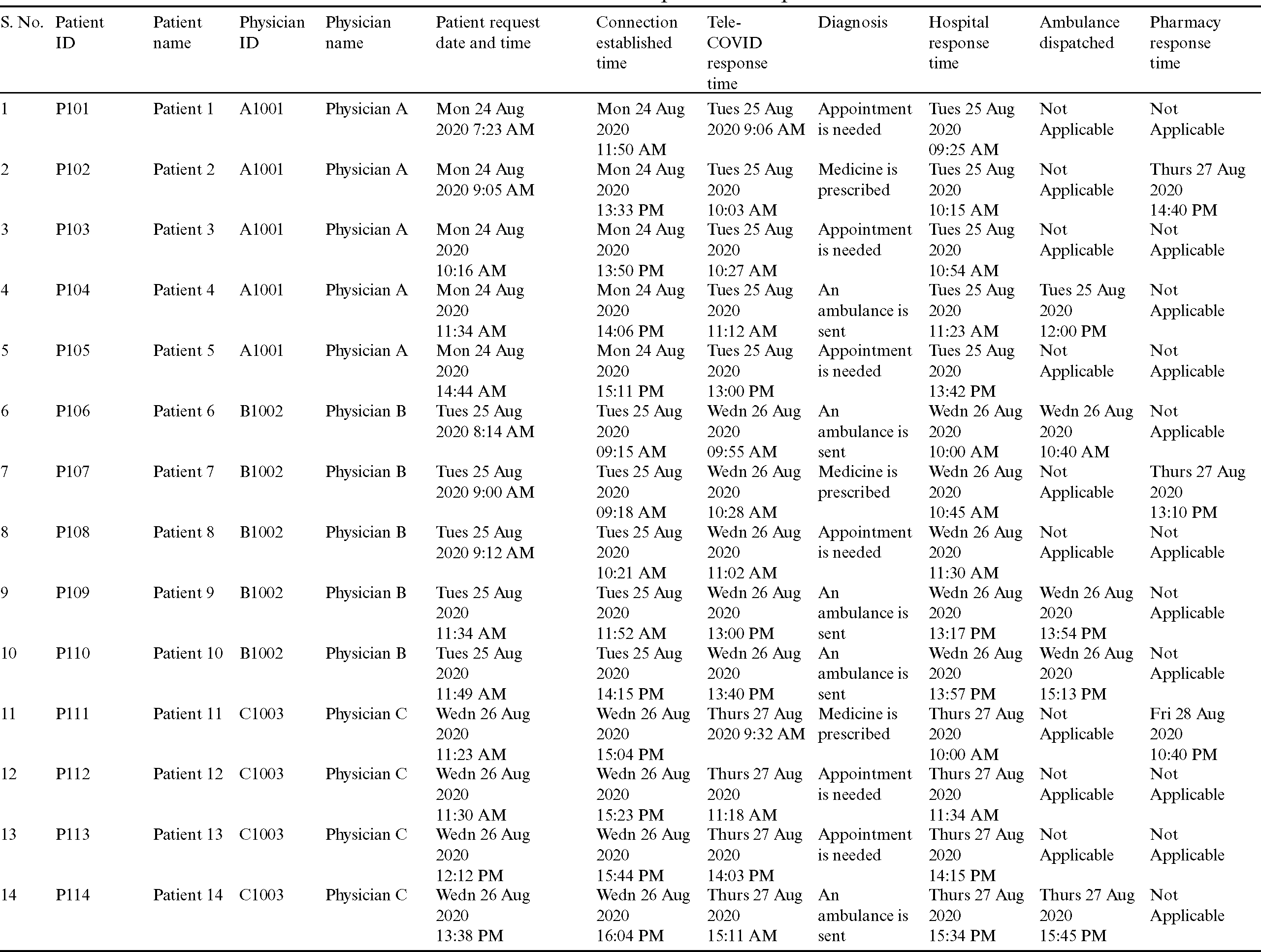
The other example is for patient P102 who required medication only; the initial processing and response time was the same as for P101 while the pharmacy response time was on the same day, Tues 25 Aug 2020, at 14:40 PM, that the patient communicated with the doctor and the doctor prescribed the medication. Patient P102 started the conversation with the doctor on Tues 25 Aug 2020 at 9:00 AM and the pharmacy responded within a few hours and delivered the medication to the patient’s residence.
The final example relates to the dispatch of an ambulance in a case where the patient was seriously ill and required hospitalization. The doctor requested an ambulance for P104, and the hospital responded and dispatched ambulance on Tues 25 Aug 2020 at 12:00 PM within 1 h of the patient’s conversation with the doctor. The city hospital was too busy and full of COVID patients; therefore, at the initial stage of the Tele-COVID deployment, the ‘Tele-COVID Response Time’ and ‘Hospital Response time,’ which were in the morning.
This could be improved later when the shortage of COVID staff is over. However, the functions for ‘Patient Requests Date and Time’ and ‘Appointment Approval Time’ depend on the request from the patient and the Tele-COVID application is ready to respond 24/7. Once COVID-19 is over, Tele-COVID can be used under normal circumstances and deployed anywhere due to the SOA and data can be exchanged between several heterogenous telemedicine application.
7 Security Implementation in Tele-COVID
The term security can be defined as a combination of privacy, integrity, and confidentiality and it can be achieved by protecting the patient’s data from unauthorized access. The Tele-COVID system architecture is fully protected with the help of a digital signature. Encryption, authentication, and authorization techniques with PKI and digital signatures were used for the application. There are two main security ends for the application, i.e., the patient’s end and the doctor’s end. At the patient’s end, the patient may send a request for an appointment, and it can only be sent through the Tele-COVID application which is linked to the national ID of the patient; therefore, it is not possible to send a request for an appointment for unregistered users. The patient is registered in a national database with an authorized phone number. In this phase of registration, an SMS will be sent to the mobile number of the patient which is registered in the national database. Upon confirmation, the registration will be completed. All the data are retrieved from the national register of the patient’s country of residence. In order to use this application in any other country, it is necessary to connect Tele-COVID with the relevant national database, so the patient’s record can be retrieved from authorized sources.
The second end for security is the doctor’s end and the security usage of the Tele-COVID framework design was built utilizing Apache Axis [36]. Apache Axis is an open-source web service system using XML. Tele-COVID utilized Java based (WSS4J) Apache Axis security for its web services based on the execution of the OASIS web services security (WS-Security). WSS4J is utilized to sign and confirm SOAP messages with WS-Security data. Additionally, WSS4J is implemented to ensure that our application benefits from the help of the Apache Axis web administration structure. WSS4J creates and measures the SOAP ties for XML Security with XML Signature and XML Encryption. Additionally, it attributes tokens for the username, timestamps, and Security Assertion Markup Language (SAML). The security of Tele-COVID activities is assured through the use of username tokens. WSS4J controllers are installed for the service sending descriptor in the Web Service Deployment Descriptor (WSDD) document for inclusion with the WS-Security layer for our telemedicine services. Moreover, by including controllers, the server-side arrangement descriptor likewise characterizes the solicitation and reaction streams. In the RequestFlow, with each service for a Tele-COVID activity, there are two security controllers that validate and approve the request. The Tele-COVID application decrypts the SOAP message with a public key for the doctor utilizing PKI security. When the message is decrypted, the WSDoAllReceiver confirms the username and secret key for approval. In the ResponseFlow, each response is encrypted with the specialist’s public key and the message is carefully marked for validation using the telemedicine’s private key.
Tele-COVID is fully capable of preventing reply attacks, which are also referred to as ‘man-in-the-middle-attack,’ where hackers can establish a connection to obtain physicians’ and patients’ data. Bottom level security is implemented to save on the cost of implementation, and it is also easy to implement. One of the essential factors in our proposed design is the avoidance of replay attacks where hackers can gain access to encrypted SOAP messages to hack the patient’s personal information. Fig. 12 illustrates a situation in which an attacker attempts to break encrypted security messages. To make any attempt at hacking unsuccessful, PKI and digital signatures for encryption, confirmation, and approval were utilized. Nevertheless, signed digital messages can be captured and resent using several techniques and this could be a major threat to Tele-COVID’s architectural design; this kind of situation represents a reply attack.

Figure 12: Proposed security architectural design without timestamp
The innovative method used to stop and prevent a reply attack is the creation of a unique SOAP message. There are various kinds of methods utilized to ensure the uniqueness of SOAP messages, such as a bit string used one time only and time stamping. WSS4J generates time stamping for each unique SOAP message to stop reply attack assaults. To avoid any kind of attack, timestamping was utilized in our Tele-COVID architectural design to make it completely secure and attack-free.
Timestamping represents a series of characters, indicating the information or time at which the service is requested. In timestamping, every service is recorded by a program. Fig. 13 shows the sample code implemented in Tele-COVID to prevent a reply attack through timestamping. A length of 45 seconds was set as the upper limit for each timestamp. Fig. 14 gives an overall view after counteraction from a replay attack.

Figure 13: Sample code of timestamping implementation

Figure 14: Proposed security architectural design with timestamp
Telemedicine is widely used for treating patients from a distance and it has become more essential and valuable during the COVID-19 pandemic where isolation is mandatory. SOA is increasing in popularity due to its wide range of privileged services and the fact that it can operate free from products, vendors, and technologies. In this paper, we have proposed an architectural design using SOA implemented in the Tele-COVID application that helps in the treatment of COVID-19 patients. Tele-COVID is based on the four main SOA-based services. Each service has its unique features for treating COVID-19 patients from a distance and its capability has been proven by testing the initial 25 patients. The Tele-COVID architecture has considered most of the security aspects that protect the data of the patient and physician from any intentional or unintentional cyber-attacks. In the future, the intention is to extend the SOA-based services to cloud computing since cloud computing and SOA resembles one another in terms of numerous services that can be further categorized as Infrastructure-as-a-Service (IaaS), Platform-as-a-Service (PaaS), and Software-as-a-Service (SaaS).
Funding Statement: The authors would like to express their Gratitudes to the ministry of education and the deanship of scientific research Najran University Kingdom of Saudi Arabia for their financial and technical support under code number NU/ESCI/18/010.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. V. Surveillances. (2020). “The epidemiological characteristics of an outbreak of 2019 novel Coronavirus diseases (Covid-19)-China, 2020,” China CDC Weekly, vol. 2, no. 8, pp. 113–122.
2. J. C. COVID-19. (2020). (Accessed 8 October 2020. Available: https://www.arcgis.com/apps/opsdashboard/index.html#/85320e2ea5424dfaaa75ae62e5c06e61.
3. S. Xu and Y. Li. (2020). “Beware of the second wave of Covid-19,” Lancet, vol. 395, no. 10233, pp. 1321– 1322.
4. A. Shaikh. (2015). “The impact of SOA on a system design for a telemedicine healthcare system,” Network Modeling Analysis in Health Informatics and Bioinformatics, vol. 4, no. 1, pp. 15.
5. D. Anton, G. Kurillo, A. Y. Yang and R. Bajcsy. (2017). “Augmented telemedicine platform for real-time re-mote medical consultation,” in Int. Conf. on Multimedia Modeling, Reykjavik, Iceland, Springer, pp. 77–89.
6. W. R. Smith, A. J. Atala, R. P. Terlecki, E. E. Kelly and C. A. Matthews. (2020). “Implementation guide for rapid integration of an outpatient telemedicine program during the Covid-19 pandemic,” Journal of the American College of Surgeons, vol. 231, no. 2, pp. 216–222.
7. World Health Organization (WHOSaudi Arabia: WHO coronavirus disease (COVID-19) dashboard. (Accessed 28 October 2020. [Online]. Available: https://covid19.who.int/region/emro/country/sa.
8. A. Shaikh, M. Memon, N. Memon and M. Misbahuddin. (2009). “The role of service-oriented architecture in telemedicine healthcare system,” in Int. Conf. on Complex, Intelligent and Software Intensive Systems, Fukuoka, Japan, IEEE, pp. 208–214.
9. A. Shaikh, S. Ali, N. Memon and P. Karampelas. (2010). “SOA security aspects in web-based architectural design,” in From Sociology to Computing in Social Networks. Vienna, Springer, pp. 415–430.
10. K. Avila, P. Sanmartin, D. Jabba and M. Jimeno. (2017). “Applications based on service-oriented architecture (soa) in the field of home healthcare,” Sensors, vol. 17, no. 8, pp. 1703. [Google Scholar]
11. A. Shaikh, M. Misbahuddin and M. S. Memon. (2008). “A system design for a telemedicine health care system,” in Int. Multi Topic Conf., Jamshoro, Pakistan, Springer, pp. 295–305. [Google Scholar]
12. B. Moazzami, N. R. Khorasani, A. D. Moghadam, E. Farokhi and N. Rezaei. (2020). “Covid-19 and telemedicine: Immediate action required for maintaining healthcare providers well-being,” Journal of Clinical Virology, vol. 126, pp. 104345. [Google Scholar]
13. K. L. Rockwell and A. S. Gilroy. (2020). “Incorporating telemedicine as part of Covid-19 outbreak response systems,” American Journal of Managed Care, vol. 26, no. 4, pp. 147–148. [Google Scholar]
14. R. Bashshur, C. R. Doarn, J. M. Frenk, J. C. Kvedar and J. O. Woolliscroft. (2020). “Telemedicine and the Covid-19 pandemic, lessons for the future,” Telemedicine and e-Health, vol. 26, no. 5, pp. 571–573. [Google Scholar]
15. D. M. Mann, J. Chen, R. Chunara, P. A. Testa and O. Nov. (2020). “Covid-19 transforms health care through telemedicine: Evidence from the field,” Journal of the American Medical Informatics Association, vol. 126, no. 5, pp. 104345. [Google Scholar]
16. V. Chauhan, S. Galwankar, B. Arquilla, M. Garg, S. Di Somma. (2020). et al., “Novel coronavirus (Covid-19Leveraging telemedicine to optimize care while minimizing exposures and viral transmission,” Journal of Emergencies, Trauma, and Shock, vol. 13, no. 1, pp. 20. [Google Scholar]
17. M. Serper, A. W. Cubell, M. E. Deleener, T. K. Casher, D. J. Rosenberg. (2020). et al., “Telemedicine in liver disease and beyond: Can the Covid-19 crisis lead to action?,” Hepatology, vol. 72, no. 2, pp. 723– 728. [Google Scholar]
18. K. Boehm, S. Ziewers, M. P. Brandt, P. Sparwasser, M. Haack. (2020). et al., “Telemedicine online visits in urology during the Covid-19 pandemic-potential, risk factors, and patients’ perspective,” European Urology, vol. 78, no. 1, pp. 16–20. [Google Scholar]
19. S. M. Saleem, L. R. Pasquale, P. A. Sidoti and J. C. Tsai. (2020). “Virtual ophthalmology: Telemedicine in a Covid-19 era,” American Journal of Ophthalmology, vol. 216, no. 5, pp. 237–242. [Google Scholar]
20. R. A. Machado, N. L. de Souza, R. M. Oliveira, H. M. Júnior and P. R. F. Bonan. (2020). “Social media and telemedicine for oral diagnosis and counselling in the Covid-19 era,” Oral Oncology, vol. 105, no. 6, pp. 1–2. [Google Scholar]
21. A. E. Loeb, S. S. Rao, J. R. Ficke, C. D. Morris, L. H. Riley III. (2020). et al., “Departmental experience and lessons learned with accelerated introduction of telemedicine during the Covid-19 crisis,” Journal of the American Academy of Orthopaedic Surgeons, vol. 28, no. 11, pp. 469–476. [Google Scholar]
22. M. J. Tanaka, L. S. Oh, S. D. Martin and E. M. Berkson. (2020). “Telemedicine in the era of Covid-19: The virtual orthopaedic examination,” Journal of Bone and Joint Surgery, vol. 102, no. 12, pp. 1–7. [Google Scholar]
23. B. Calton, N. Abedini and M. Fratkin. (2020). “Telemedicine in the time of coronavirus,” Journal of Pain and Symptom Management, vol. 60, no. 1, pp. e12–e14. [Google Scholar]
24. S. Omboni. (2020). “Telemedicine during the Covid-19 in Italy: A missed opportunity?,” Telemedicine and e-Health, vol. 26, no. 8, pp. 973–975. [Google Scholar]
25. H. Leite, I. R. Hodgkinson and T. Gruber. (2020). “New development: ‘Healing at a distance’-telemedicine and COVID-19,” Public Money & Management, vol. 40, no. 6, pp. 483–485. [Google Scholar]
26. H. C. Jen. (2008). “Telemedicine information monitoring system,” in HealthCom 2008-10th Int. Conf. on e-Health Networking, Applications and Services, Singapore, IEEE, pp. 48–50. [Google Scholar]
27. S. H. Hsieh, S. L. Hsieh, P. H. Cheng and F. Lai. (2012). “E-health and healthcare enterprise information system leveraging service-oriented architecture,” Telemedicine and e-Health, vol. 18, no. 3, pp. 205– 212. [Google Scholar]
28. B. B. Traore, B. Kamsu-Foguem and F. Tangara. (2016). “Integrating MDA and SOA for improving telemedicine services,” Telematics and Informatics, vol. 33, no. 3, pp. 733–741. [Google Scholar]
29. C. D. Capua, A. Meduri and R. Morello. (2010). “A smart ECG measurement system based on web-service-oriented architecture for telemedicine applications,” IEEE Transactions on Instrumentation and Measurement, vol. 59, no. 10, pp. 2530–2538. [Google Scholar]
30. T. Raafat and F. Cecelja. (2011). “Application of semantic web services for mobile telemedicine service discovery,” in IEEE 35th Annual Computer Software and Applications Conf., Munich, Germany, IEEE, pp. 562–563. [Google Scholar]
31. I. Ruiz, J. Contreras and J. Garcia. (2020). “Towards a physical rehabilitation system using a telemedicine approach,” Computer Methods in Biomechanics and Biomedical Engineering: Imaging & Visualization, vol. 8, no. 5, pp. 1–10. [Google Scholar]
32. J. Peral, A. Ferrandez, D. Gil, R. Munoz-Terol and H. Mora. (2018). “An ontology-oriented architecture for dealing with heterogeneous data applied to telemedicine systems,” IEEE Access, vol. 6, pp. 41118–41138. [Google Scholar]
33. D. Y. Weider and R. Bhagwat. (2011). “Modeling emergency and telemedicine heath support system: A service oriented architecture approach using cloud computing,” International Journal of E-Health and Medical Communications, vol. 2, no. 3, pp. 63–88. [Google Scholar]
34. E. Guillén, J. Ubaque, L. Ramirez and Y. Cardenas. (2012). “Telemedicine network implementation with SOA architecture: A case study,” in Proc. of the World Congress on Engineering and Computer Science, pp. 24–27. [Google Scholar]
35. M. A. Musen and J. H. Van Bemmel. (1997). Handbook of medical informatics. In: Handbook of medical informatics. Heidelberg: Springer. [Google Scholar]
36. Apache axis. (2015). “Web Service Security,” (Accessed 6 October 2020. Available: http://axis.apache.org/axis/java/security.html. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |