DOI:10.32604/cmc.2020.011943
| Computers, Materials & Continua DOI:10.32604/cmc.2020.011943 | |
| Article |
Confocal 3D Optical Intraoral Scanners and Comparison of Image Capturing Accuracy
Department of Prosthetic Dentistry, Faculty of Dentistry, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand
*Corresponding Author: Sasiwimol Sanohkan. Email: ssasiwimol@yahoo.com
Received: 06 June 2020; Accepted: 24 July 2020
Abstract: Several capture techniques are used in intraoral optical scanners in the dental market, such as Triangulation (Cerec Omnicam, Dentsply Sirona), Activewave front sampling (3M ESPE) and confocal technology (iTero, Align). The accuracy of intraoral scanners is the most significant focal point for developers to research. This in-vitro study studied the accuracy of confocal scanners launched from 2015-2020 (Trios 3, Trios 4, iTero Element; 3Shape Trios A/S, Copenhagen, Denmark, and iTero Element2, and iTero Element5D; Align Technologies, San Jose, CA, USA). A 3D printing model modified from the American National Standard No. 132 was scanned five times each scanner. Both Trios3 and Trios4 were scanned using regular scan mode (N) and high-resolution mode (HR). All scanning methods followed the recommendations from the manufacturers. Then the digital models were exported and saved as STL files. Various measurements were determined in the digital model from each scan using Rhinoceros 3D Software (Rhino, Robert McNeel & Associates for Windows, Washington DC, USA). Measurements from the 3D printed model were used as control. All data were recorded in Microsoft Excel and then transferred to SPSS. Descriptive statistics were recorded. Multiple comparisons of various measurements were made among the different scanners and with the control using One-way ANOVA and post hoc using Sheffe (p < 0.01). The surface area in the X and Y axis ranged from 2–60 mm, while the depth (Z-axis) ranged from 2–8 mm. The Trios and iTero families showed similar accuracy. However, for the diagonal, the Trios series showed better results compared with the iTero series. Within the same brand, different versions showed no significant change regarding accuracy.
Keywords: Confocal; intraoral scanners; accuracy; 3-dimensional analysis; teeth analysis; digital
Vast advancement has been made in digital technology and image capturing and processing [1–3]. Such advancements have created new modalities in modern medicine and dentistry [4,5]. Currently, intraoral scan, computer-aided design (CAD) and computer-aided manufacturing (CAM) are widely used in prosthodontics, restorative dentistry, orthodontics, and implant dentistry [6]. Digital technologies aid in the diagnosis, treatment planning, and fabrication of prostheses. An excellent dental impression is preferred to fabricate an accurate dental prosthesis or restoration [7]. Dentists send a digital impression from the clinic to the laboratory, and dental technicians create a digital model, design, and manufacture the prosthesis. Once the dental laboratory receives a digital file (impression), dental laboratory technicians design the work on the computer and fabricate the prosthesis or restoration.
Although various intraoral scans are available in the market, a noncontact scanning technique is widespread [8]. Intraoral scanners (IOS) have a small area of measurements, such as 1 to 2 teeth or quadrants [9,10]. A series of developments have advanced scanning technology. For example, (a) triangulation scanning technique was used but was slower, such as Cerec (Dentsply Sirona, USA). In addition, (b) active wavefront sampling, True Definition (3M ESPE), provides a smaller tip for dentists to approach the last molar with more accuracy. Further, (c) confocal scanning technique is a faster technique, improving accuracy and is powderless such as iTero (Align Technology) and Trios (3Shape) [11–13].
Confocal laser scanning microscopy captures images by focusing on an optical light beam with high-resolution visual images and depth selectivity [12]. The optical light from a light source passes to the specific lens, and the mean light will be smaller than the standard microscope technique and enhanced to scan more details of the sample [14]. Also, a shift in the focus plane results in a curve, creating 3D images of the flat surfaces minimizing the distortions, as shown in Fig. 1 [15].
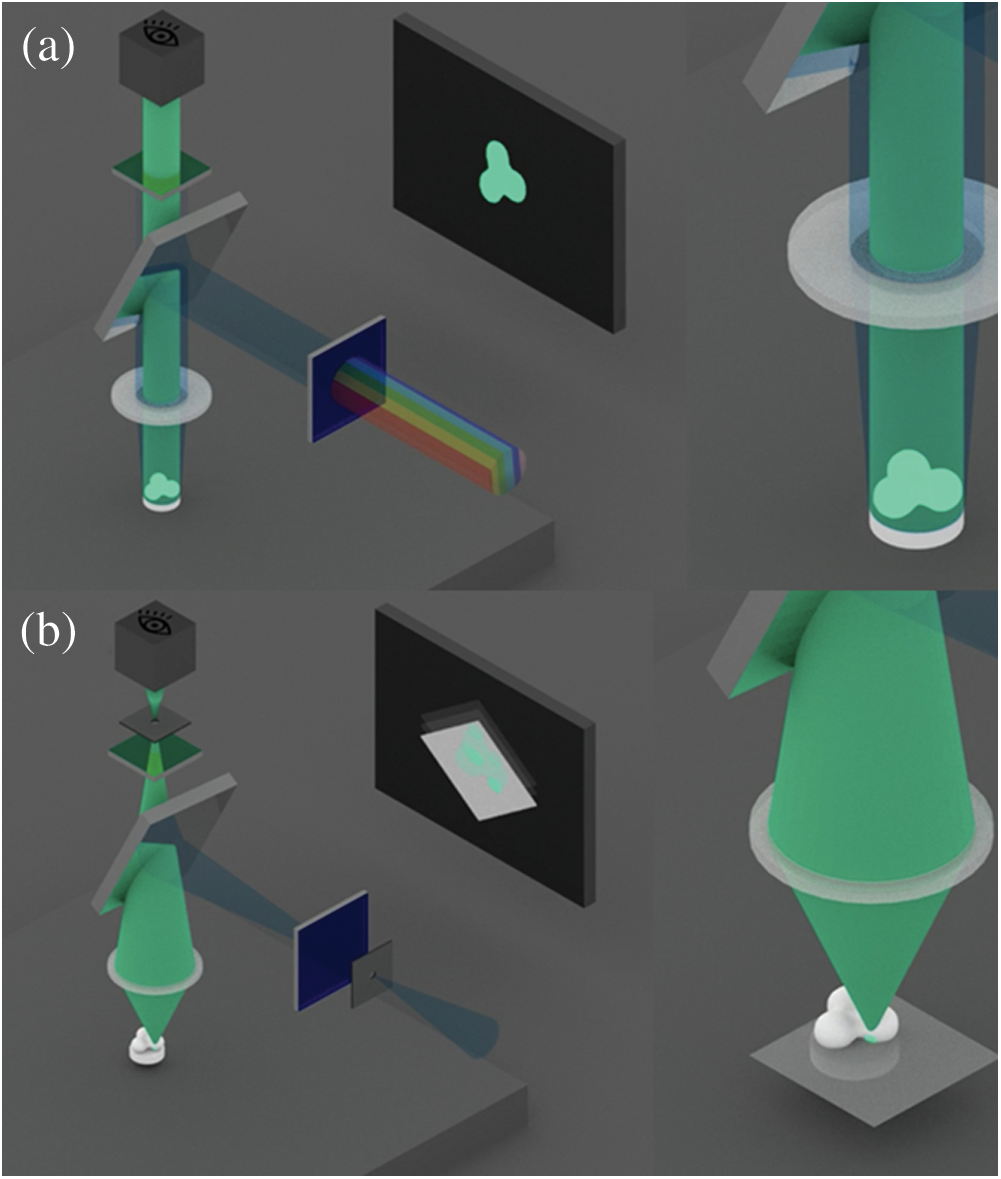
Figure 1: Microscopy imaging of standard/normal microscopy (a) and confocal microscopy (b) showing the 3D images of the flat surfaces [15]
The first intraoral confocal scanner was incorporated in early 2007 by iTero Element (Cadent recently acquired by Align in 2011). A year later, a Danish startup company named 3Shape launched Trios in the dental market. The iTero Element and Trios IOS share the majority in the dental market, which has more advantages by having powderless systems while scanning, providing faster scans and color capture [16]. Moreover, these two IOS use CAD Software, which is used in restorative dentistry, implant dentistry, and orthodontics [17]. At present, other companies are endeavoring to integrate this confocal technology into their scanner systems. This in-vitro study aimed to compare the confocal IOS launched from 2015 to 2020 (Trios 3, Trios 4, Trios Element, iTero Element2, and iTero Element5D).
The study consists of scanning, measurements, and comparison of the confocal IOS launched from 2015 to 2020 (Trios Element, iTero Element2, and iTero Element5D). This study followed the study of Amornvit et al. [18], modified from the American National Standard (ANS) Standard No. 132 [19] to compare the scans. A dental model was printed with grey resin (50 microns) from Form2 (Formlab) following manufacturers’ recommendations. Various points were marked to measure the various axes (X, Y, XY, and Z).
The resin dental model was scanned five times each with Trios 3 and Trios 4 in the regular mode (Trios 3 and Trios 4), and high-resolution mode (Trios 3HR and Trios 4HR) (3Shape Trios A/S 2018, Copenhagen, Denmark) and (iTero Element, iTero Element2 and iTero Element5D) (Align Technologies, San Jose, CA, USA) following the recommendations from the manufacturers. Then the digital models were exported and saved as stereolithography (STL) files.
Then measurements were determined using a digital model (as shown in Fig. 2) from each scan using the Rhinoceros Software (Rhino, Robert McNeel & Associates for Windows, Washington DC, USA). The 3D printed model was measured using digital calipers. Additionally, the details of the scans from various IOS were also evaluated.
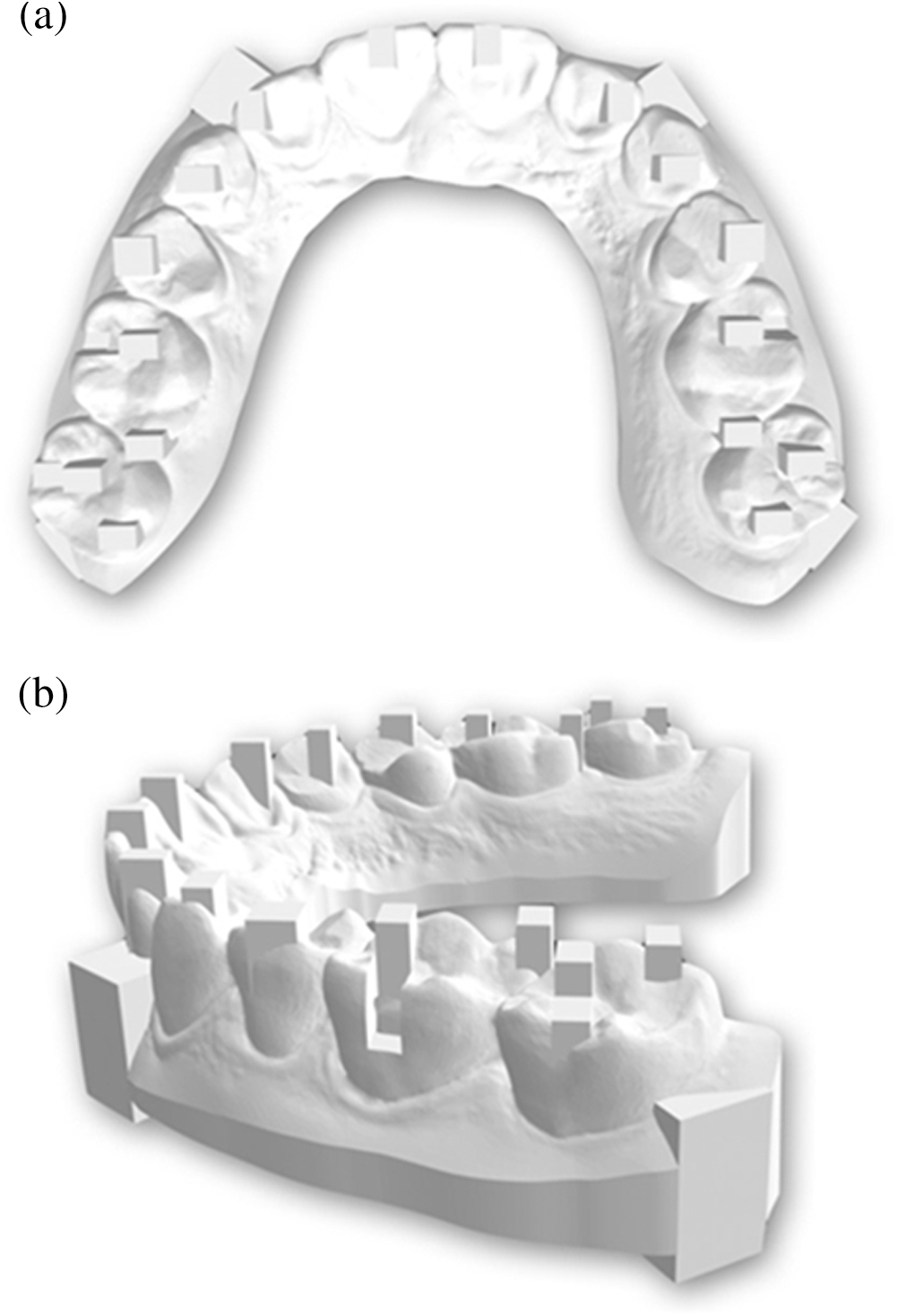
Figure 2: Digital dental model, occlusal view (a) and side view (b)
At first, the data were entered in Microsoft Excel 2019 and then transported to SPSS. Version 22 (IBM Company, Chicago, IL, USA), and descriptive statistics were calculated. Multiple comparisons of measurements among various IOS and the control were made using One-way ANOVA and post hoc using Sheffe (p < 0.01).
Tabs. 1–4 show the descriptive statistics of the scans of measurements in the X-axis, Y-axis (Y1, Y2, Y3, and Y4), XY-axis (AR and AL) and Z-axis (Z1, Z2, Z3, and Z4). The scan results show that Trios 3 and Trios 3HR presented better capture quality than iTero Element2 and iTero Element5D.
Table 1: Descriptive statistics in the X-axis
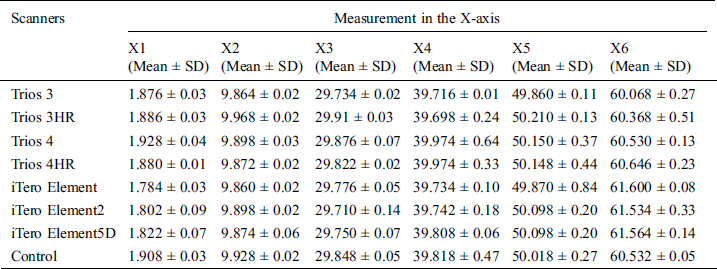
Table 2: The descriptive statistics in the Y-axis
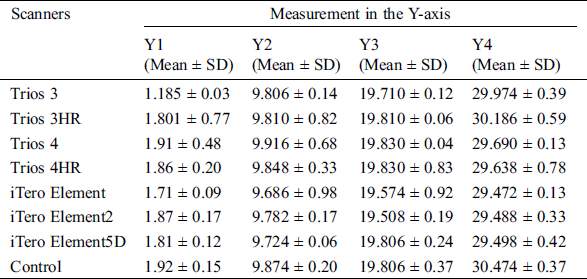
Table 3: Descriptive statistics in the Z-axis
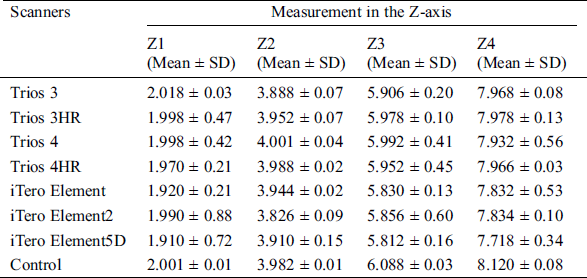
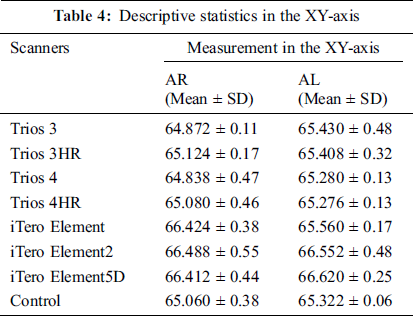
Table 4: Descriptive statistics in the XY-axis
Tab. 1 shows the descriptive statistics of the scans of measurements in the X-axis (X1, X2, X3, X4, X5, and X6). The measurements X1, X2, X3, X4, and X5, is revealing no significant difference compared with the control (p > 0.01). For the X6, iTero Element, iTero Element2, and iTero Element5D showed a significant difference compared with the control (p < 0.001). Multiple comparisons among the scanners in the X-axis showed a significant difference for the measurements X1 to X5. Additionally, each scanner (Trios 3, Trios 3HR, Trios 4, and Trios 4HR) showed significant differences (p < 0.001) with iTero Element, iTero Element2, and iTero Element5D for the measurement X6 (60 mm).
Tab. 2 shows the descriptive statistics of the scans of measurements on the Y-axis (Y1, Y2, Y3, and Y4). All measurements in the Y-axis (Y1, Y2, Y3, and Y4) showed no significant difference compared with the control (p > 0.01). Multiple comparisons among the scanners in the Y-axis showed no significant difference for the measurements Y1 to Y4.
Tab. 3 shows the descriptive statistics of the scans of measurements in the Z-axis (Z1, Z2, Z3, and Z4). All measurements in the Z-axis (Z1, Z2, Z3, and Z4) showed no significant difference compared with the control (p > 0.01). Multiple comparisons among the scanners in the Z-axis showed a significant difference for the measurements Z1 to Z4.
Tab. 4 shows the descriptive statistics of the scans of measurements in the XY-axis (AR and AL). Both analyses (AR and AL) showed a significant difference compared with the control (p < 0.001). Also, each scanner, Trios 3, Trios 3HR, Trios 4, and Trios 4HR showed significant differences (p < 0.001) with iTero Element, iTero Element2, and iTero Element5D for the measurements AR and AL (65 mm)
Digital technologies can be integrated into medicine and dentistry for ease in the diagnosis and treatment of a disease. Image capturing and processing has continued to advance in recent years [20–22]. In dentistry, its applications include data acquisition to prosthesis fabrication. Intraoral scanners reduce the clinical time of dentists and dental technicians. The IOS simplifies the procedures in the clinic, eliminates plaster models and allows improved communication between the dentist and dental technician, reducing errors [6,7,18]. IOS also helps in explaining to and motivating the patients. In intraoral scanning technology, the confocal trend has become more advantageous, making scanning more accurate and faster. The intraoral scanner companies are prepared to launch their new products, incorporating the confocal technique, including Cerec, Prime scan, and Virtual Vivo from Dental Wings (Straumann). This study compared the confocal scanners launched from 2015 to 2020 (Trios and iTero IOS), and the results form guidelines in selecting the proper dental work for each scanner.
The 3Shape has a smaller tip than the iTero (shown in Fig. 3). The capture box is one factor that can affect accuracy. The capture box is an area where the scanner captures objects in each image and is related to the scanner tip. The smaller tip makes it accessible to various locations intraorally, especially the third molar area. The sleeve of the 3Shape is smaller than the iTero, but the capture box is 65% larger (shown in Fig. 3). A small capture box requires more stitching or connecting image files and will create more errors (shown in Fig. 4). Hence, a larger capture box results in more accuracy but makes it challenging to capture the corner areas intraorally, such as in Lab scans.
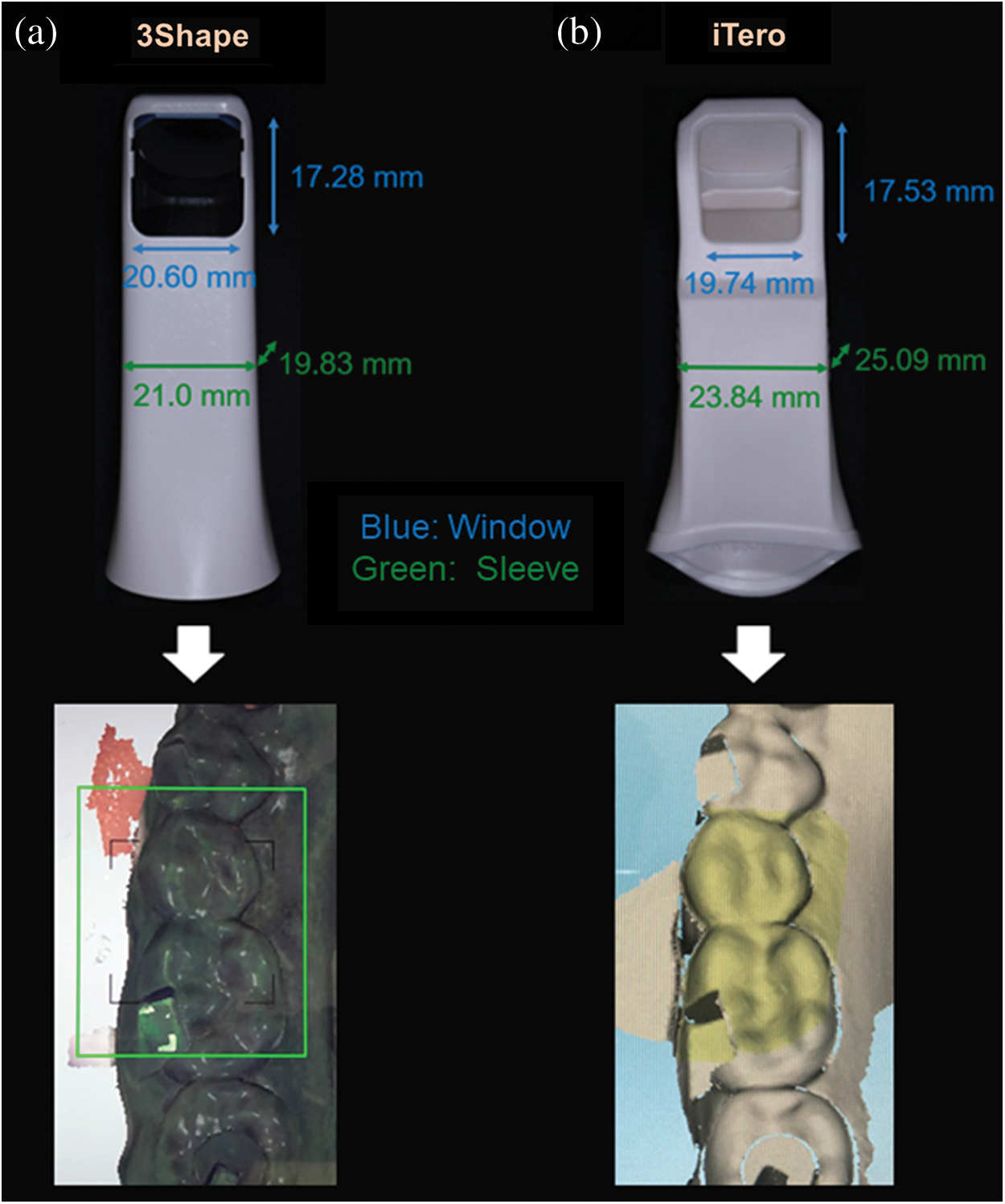
Figure 3: Scan tip, sleeve size and capture box shown in the computer monitor of 3Shape (A) and iTero (B)
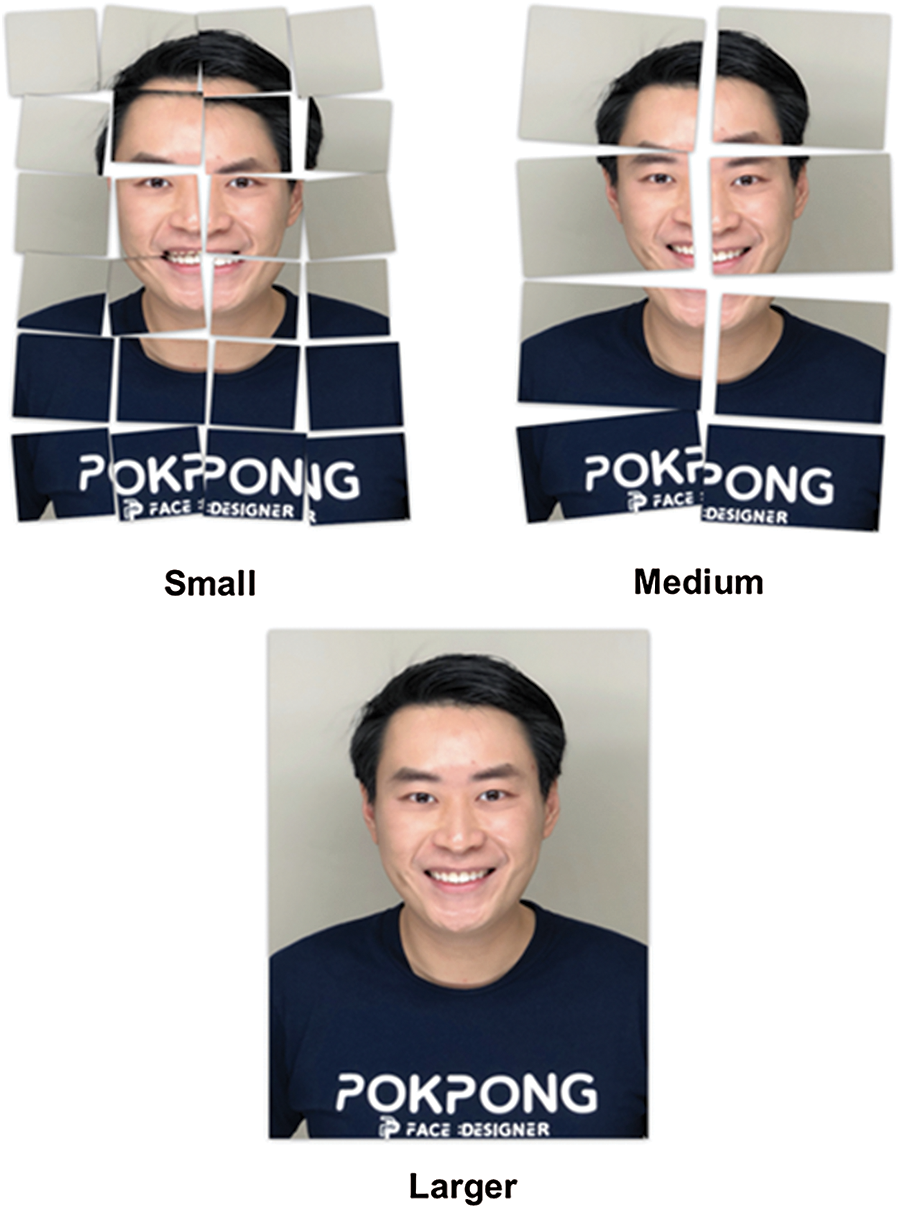
Figure 4: A small capture box requires more stitching images to scan, creating more errors, whereas large capture boxes need fewer stitching images showing fewer errors
From observation, 3Shape has 30 × 22 mm, whereas iTero Element has 18 × 14 mm for the light source area. Trios 3 shows shaking optical lights moving slightly around an object resulting from changing the distance of the moving lens to enhance the ability to capture the depth accurately. The iTero Element shows two lights; first, a white light slightly the same as Trios but projected together with two angles in the same capture and second, a red light laser for enhancing the capturing accuracy (shown in Fig. 5).
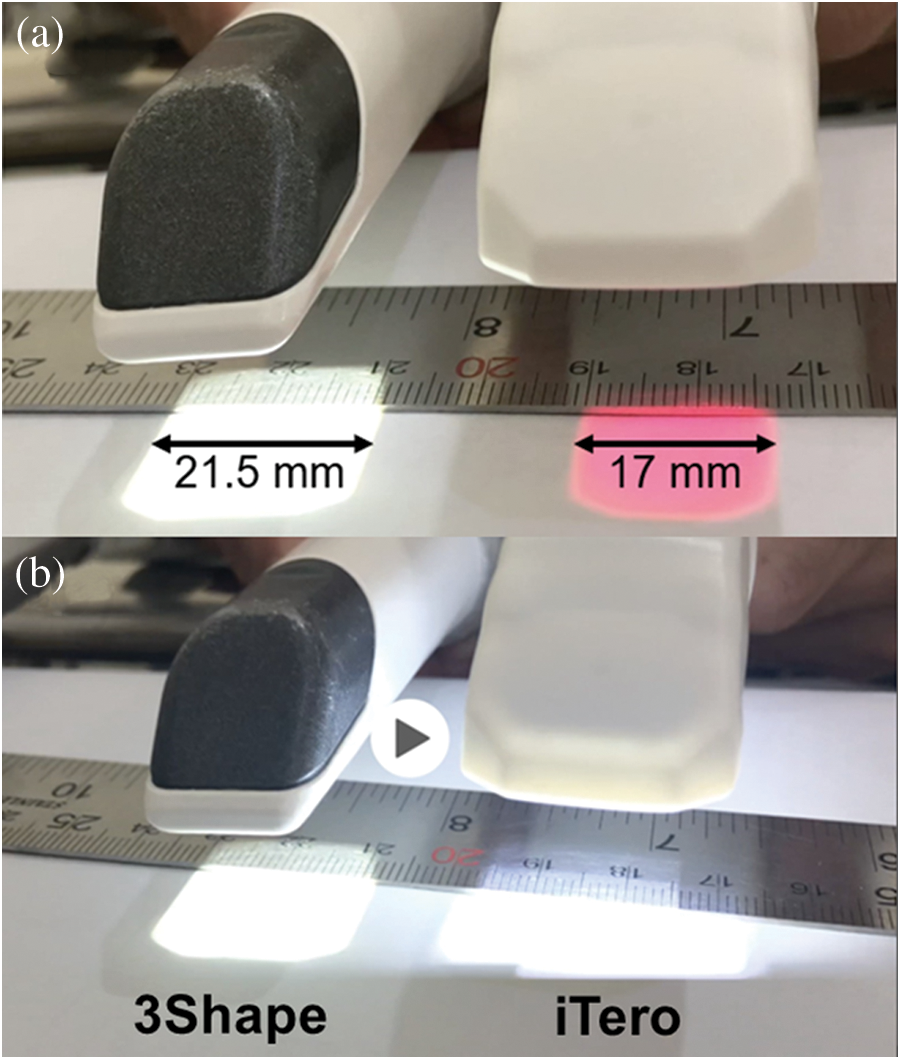
Figure 5: Capture box of Trios 3 and iTero measured by slow motion mode of a digital camera showing the white light by Trios 3 and the red light by iTero (a) and showing the white light by both scanners (b)
In this study, for measurements <60 mm, no significant difference was found among the various IOS (Trios 3, Trios 3HR, Trios 4, Trios 4HR, iTero Element, iTero Element2, and iTero Element5D). The dimension measured X6 (60 mm) could be represented as 14 units or full arch restoration. On the other hand, for diagonal measurements (AR and AL) of 65 mm, a significant difference (p-value < 0.01) was observed between the iTero series. The Trios series in both normal and HR modes can record full arch more accurately than the iTero series. Obtaining accuracy for the diagonal measurement is most challenging. The bending or distortion mostly occurs in the anterior areas because of the shape of the anterior teeth, less structured tooth surface and steep inclines, tapering, and thinner, more similar to triangular than posterior teeth (shown in Fig. 6).
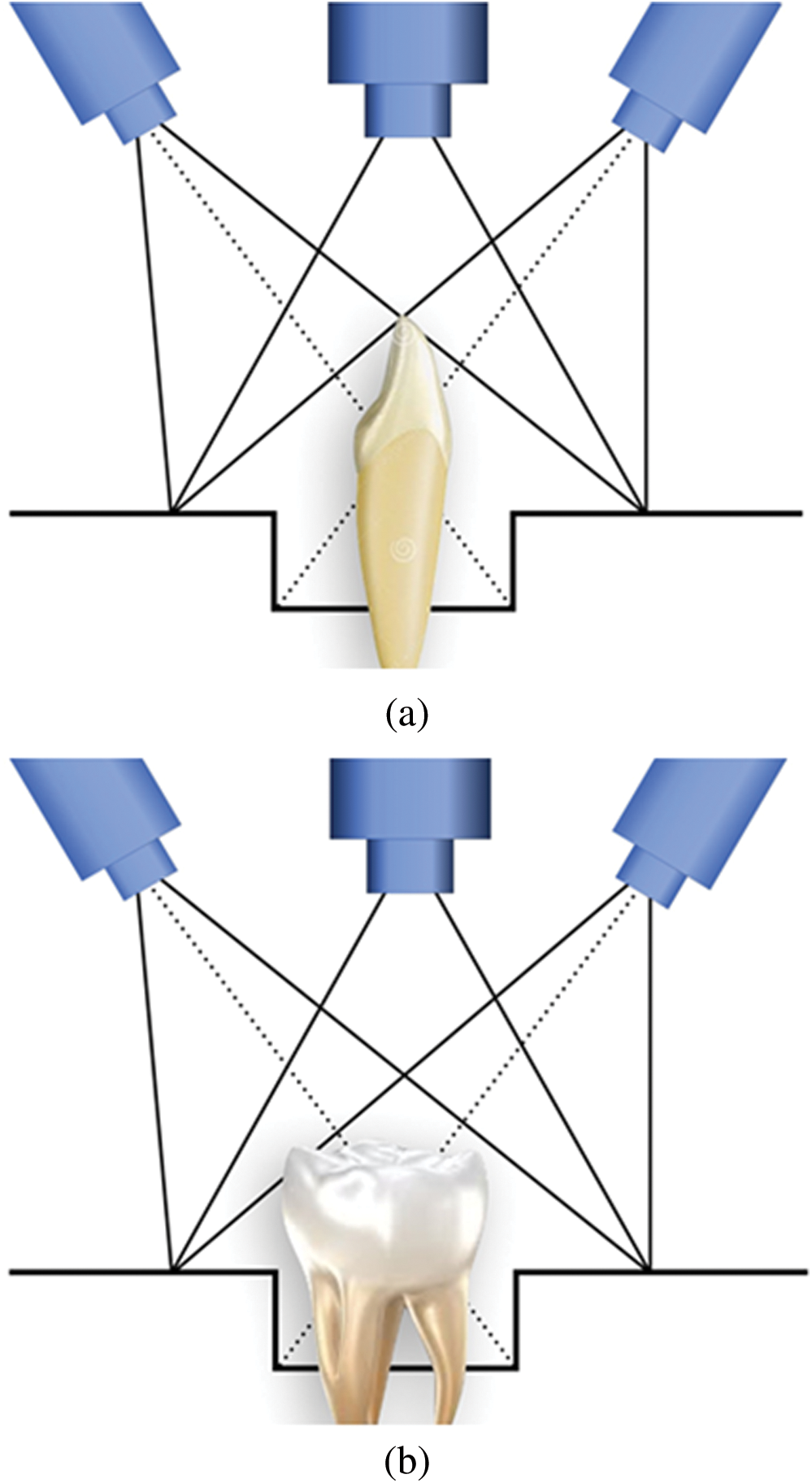
Figure 6: Schematic diagram showing anterior scan (a) and posterior scan (b)
Some scans in Trios show bending, but the software will not correct itself, and the operator needs to rescan that area. However, distortion in the scan of iTero will attempt to correct or render itself, which may result in lowered accuracy, especially in a full mouth scan. To reduce distortion, some landmarks may place flowable composite or gingival barrier liquid, e.g., Opaldam, on the palate and scan the palate before and across the arch (shown in Fig. 7).
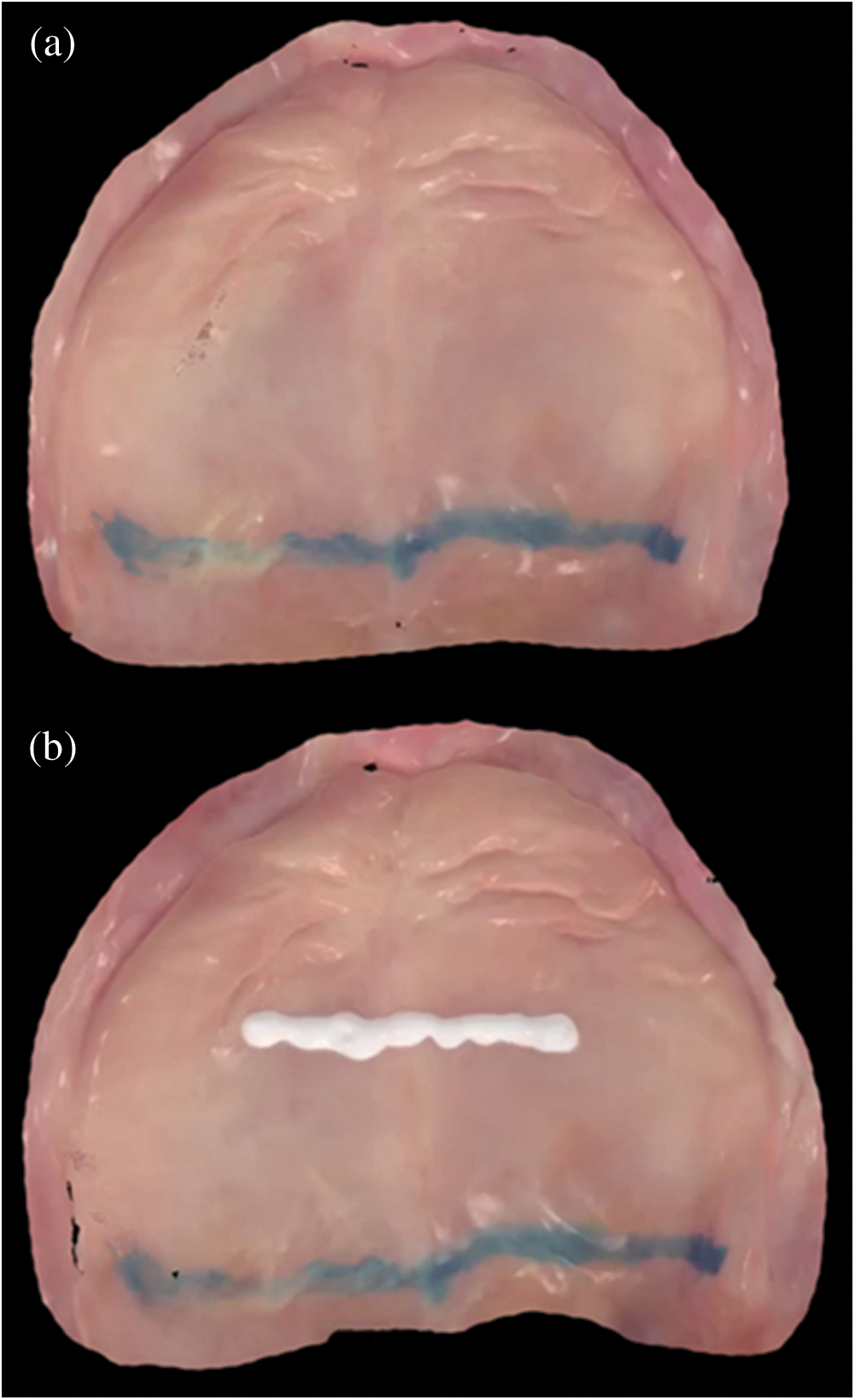
Figure 7: Palatal scan showing without (a) and with (b) flowable composite on the palate to increase scanning accuracy
Regarding high resolution or Zoom mode in the current version, the scanning mode of 3Shape allows the capturing of smaller details such as the margin or interproximal area. The capture box will be narrow, meaning the beam of light sources of the confocal scanner will be more parallel to increase the detail-capturing ability of the IOS. The results in the present study are similar to the research findings by Chiu et al. in 2020, reporting no significant difference between the normal and high-resolution modes for Trios 3 [23]. This study studied only a small area of the dental model, similar to the results of the study conducted by Amornvit et al. [18]. However, when used in a larger area especially diagonal axis, a significant difference was found between normal and HR modes of 3Shape, especially in the Z-axis (height), which supports the hypothesis that focus beam adjustment of the scanner enhances the accuracy in depth [18]. Renne et al. found that Trios shows better speed, precision, and trueness of complete-arch scans compared with iTero [24]. However, few studies have found that although some deviations appeared visually, no significance was found between the 2 IOS scanners (Trios and iTero) [13,24].
Errors can occur while scanning and measuring the intraoral features. The IOS captures approximately 1200 images when scanning an arch. Scanning errors can result due to the overlap of the images while scanning and processing of the images resulting in deviations, especially in the anterior teeth [6,24]. Errors can occur when computer processing from filter algorithms and calibration [25]. Errors have also been observed among the various axes. In our study, more errors were observed in the Z-axis or when depth scanning. These errors might be reduced with improvements in the software.
Other factors influenced accuracy such as scanner unit (size of wand and capture box, receiver, light source), operator (scanning pattern and skill), software and computer speed scanning area (scanning area, length and surface irregularities), and intraoral factors (temperature, relative humidity, and illumination) [26–28]. These factors were not considered in this study.
This study showed that confocal optical scanning technology is reliable. Within the limitations of this study, the following results were observed.
•The surface area in the X and Y axis ranged from 2 to 60 mm, while the depth (Z-axis) ranged from 2 to 8 mm. All scanners were acceptable.
•For the diagonal, the Trios series showed better results compared with the iTero series.
•Within the same brand, different versions showed no significant change regarding accuracy.
Funding Statement: This research was supported by the Maxillofacial Prosthodontics and Dental Materials Research Unit, Faculty of Dentistry, Prince of Songkla University and Scholarship Award of Thai Ph.D. Student under Thailand’s Education Hub for Southern Region of ASEAN countries, Prince of Songkla University.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1Y. Gui and G. Zeng. (2020), “Joint learning of visual and spatial features for edit propagation from a single image. ,” Visual Computer, vol. 36, no. (3), pp, 469–482, .
2W. Wang, Y. T. Li, T. Zou, X. Wang, J. Y. You et al.. (2020). , “A novel image classification approach via Dense-MobileNet models. ,” Mobile Information Systems, vol. 2020, 7602384, .
3D. Zhang, Z. Liang, G. Yang, Q. Li, L. Li et al.. (2018). , “A robust forgery detection algorithm for object removal by exemplar-based image inpainting. ,” Multimedia Tools and Applications, vol. 77, no. (10), pp, 11823–11842, . [Google Scholar]
4T. A. Sulaiman. (2020), “Materials in digital dentistry—A review. ,” Journal of Esthetic and Restorative Dentistry, vol. 32, no. (2), pp, 171–181, . [Google Scholar]
5P. Amornvit and S. Sanohkan. (2019), “The accuracy of digital face scans obtained from 3D scanners: An in vitro study. ,” International Journal of Environmental Research & Public Health, vol. 16, no. (24), pp, 5061, . [Google Scholar]
6P. K. Kudva. (2016), “Digital dentistry: The way ahead. ,” Journal of Indian Society of Periodontology, vol. 20, no. (5), pp, 482–483, . [Google Scholar]
7K. Suese. (2020), “Progress in digital dentistry: The practical use of intraoral scanners. ,” Dental Materials Journal, vol. 39, no. (1), pp, 52–56, . [Google Scholar]
8T. Sawase and S. Kuroshima. (2020), “The current clinical relevancy of intraoral scanners in implant dentistry. ,” Dental Materials Journal, vol. 39, no. (1), pp, 57–61, . [Google Scholar]
9Y. Takeuchi, H. Koizumi, M. Furuchi, Y. Sato, C. Ohkubo et al.. (2018). , “Use of digital impression systems with intraoral scanners for fabricating restorations and fixed dental prostheses. ,” Journal of Oral Sciences, vol. 60, no. (1), pp, 1–7, . [Google Scholar]
10H. Rudolph, H. Salmen, M. Moldan, K. Kuhn, V. Sichwardt et al.. (2016). , “Accuracy of intraoral and extraoral digital data acquisition for dental restorations. ,” Journal of Applied Oral Science, vol. 24, no. (1), pp, 85–94, . [Google Scholar]
11R. Richert, A. Goujat, L. Venet, G. Viguie and S. Viennot et al.. (2017). , “Intraoral scanner technologies: A review to make a successful impression. ,” Journal of Healthcare Engineering, vol. 2017, pp, 8427595, . [Google Scholar]
12S. Logozzo, E. M. Zanetti, G. Franceschini, A. Kilpelä and A. Mäkynen. (2014), “Recent advances in dental optics–Part I: 3D intraoral scanners for restorative dentistry. ,” Optics and Lasers in Engineering, vol. 54, pp, 203–221, . [Google Scholar]
13F. Mangano, A. Gandolfi, G. Luongo and S. Logozzo. (2017), “Intraoral scanners in dentistry: A review of the current literature. ,” BMC Oral Health, vol. 17, no. (1), pp, 149, . [Google Scholar]
14S. Logozzo, G. Franceschini, A. Kilpela, M. Caponi, L. Governi et al.. (2011). , “A comparative analysis of intraoral 3D digital scanners for restorative dentistry. ,” Internet Journal of Medical Technology, vol. 5, no. (1), pp, 1–18, . [Google Scholar]
15Fluorescent and Confocal Microscopies. Orsay, France: Physics Reimagined, . [Online]. Available. : https://toutestquantique.fr/en/fluorescent-and-confocal/. [Google Scholar]
16K. M. Lee. (2018), “Comparison of two intraoral scanners based on three-dimensional surface analysis. ,” Progress in Orthodontics, vol. 19, no. (1), pp, 6, . [Google Scholar]
17Digital Impression Systems. South San Francisco, CA 94080, USA: Dentalcompare, . [Online]. Available. : https://www.dentalcompare.com/Dental-Digital-Imaging-Dental-Imaging/4875-3D-Camera-Systems-Digital-Impression-Systems/. [Google Scholar]
18P. Amornvit, S. Sanohkan and C. Peampring. (2020), “Studying the optical 3D accuracy of intraoral scans: An in vitro Study. ,” Journal of Healthcare Engineering, vol. 2020, 5739312, . [Google Scholar]
19ANSI/ADA Standard No. 132. (2015), Scanning Accuracy of Dental Chairside and Laboratory CAD/CAM Systems. Illinois, USA: American Dental Association, . [Online]. Available. : http://ebusiness.ada.org/productcatalog/10945/ADA-ANSI-Dental-StandardsCADCAM/ANSIADA-Standard-No-132-Scanning-Accuracy-of-Dental-Chair-Si/ADA132-2015D. [Google Scholar]
20Y. Song, Y. Zeng, X. Y. Li, B. Y. Cai and G. B. Yang. (2017), “Fast CU size decision and mode decision algorithm for intra prediction in HEVC. ,” Multimedia Tools and Applications, vol. 76, no. (2), pp, 2001–2017, . [Google Scholar]
21W. Wang, Y. B. Jiang, Y. H. Luo, J. Li, X. Wang et al.. (2019). , “An advanced deep residual dense network (DRDN) approach for image super-resolution. ,” International Journal of Computational Intelligence Systems, vol. 12, no. (2), pp, 1592–1601, .
22D. Cao, B. Zheng, B. F. Ji, Z. B. Lei and C. H. Feng. (2018), “A robust distance-based relay selection for message dissemination in vehicular network. ,” Wireless Networks, vol. 26, no. (3), pp, 1755–1771, . [Google Scholar]
23A. Chiu, Y. W. Chen, J. Hayashi and A. Sadr. (2020), “Accuracy of CAD/CAM digital impressions with different intraoral scanner parameters. ,” Sensors (Basel), vol. 20, no. (4), pp, 1157, . [Google Scholar]
24W. Renne, M. Ludlow, J. Fryml, Z. Schurch, A. Mennito et al.. (2017). , “Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. ,” Journal of Prosthetic Dentistry, vol. 118, no. (1), pp, 36–42, . [Google Scholar]
25A. Ender and A. Mehl. (2013), “Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. ,” Journal of Prosthetic Dentistry, vol. 109, no. (2), pp, 121–128, . [Google Scholar]
26H. N. Park, Y. J. Lim, W. J. Yi, J. S. Han and S. P. Lee. (2018), “A comparison of the accuracy of intraoral scanners using an intraoral environment simulator. ,” Journal of Advanced Prosthodontics, vol. 10, no. (1), pp, 58–64, . [Google Scholar]
27R. E. Matta, W. Adler, M. Wichmann and S. M. Heckmann. (2017), “Accuracy of impression scanning compared with stone casts of implant impressions. ,” Journal of Prosthetic Dentistry, vol. 117, no. (4), pp, 507–512, .
28R. G. Nedelcu and A. S. Persson. (2014), “Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. ,” Journal of Prosthetic Dentistry, vol. 112, no. (6), pp, 1461–1471, . [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |