| Congenital Heart Disease |
DOI: 10.32604/chd.2022.019603
CASE REPORT
Concordant Atrioventricular Connection to L-Looped Ventricles with the Left Ventricle on Top of the Right Ventricle in Situs Solitus: A Case Report with 3D Modelling and Printing
1Department of Pediatrics, Seoul National University Children’s Hospital, Seoul National University College of Medicine, Seoul, Korea
2Department of Thoracic and Cardiovascular Surgery, Seoul National University Children’s Hospital, Seoul, Korea
3Department of Radiology and the Institute of Radiation Medicine, Seoul National University Hospital, Seoul, Korea
*Corresponding Author: Eun-Jung Bae. Email: eunjbaek@snu.ac.kr
Received: 06 February 2022; Accepted: 08 June 2022
Abstract: We report the case of a rare complex cardiac anomaly involving situs solitus, concordant atrioventricular connection with left-hand ventricular topology, and L-looped ventricles. The ventricles had a superior-inferior relationship with an inferiorly located right ventricle, which had a double outlet with far posteriorly located great arteries. The left atrium was elongated, with juxta-positioned atrial appendages on the right side. The 3D-printed model using a computed tomography scan taken on the fourth day of birth demonstrated the anatomy clearly and helped us decide on the surgical management.
Keywords: Double outlet right ventricle; superior-inferior ventricle; L-looped ventricles; 3D printing
The relationship between the atrioventricular connection and the pattern of the ventricular loop in most hearts is either a concordant atrioventricular connection with right-hand ventricular topology (D-looped) or a discordant atrioventricular connection with left-hand topology (L-looped) in situs solitus [1,2]. We encountered the rare case of a newborn with situs solitus, concordant atrioventricular connection and L-looped ventricles. This would be a mismatch between the atrioventricular connection and segmental analysis. Herein, we describe this extremely unusual anatomy using a three-dimensional (3D) printed model, which clearly showed this highly complex heart. This study was approved by the Institutional Review Board of Seoul National University Hospital (No. H-2112-082-1282).
A male infant weighing 2.9 kg was born at full term. Since fetal echocardiography demonstrated a complex heart anomaly with superior-inferior ventricles and an abnormal origin of the great arteries, the mother was referred to a tertiary hospital. There were no perinatal problems, and he showed no cyanosis or signs of respiratory distress early after birth. Physical examination revealed a grade 2 cardiac murmur at the left sternal border. Percutaneous O2 saturation ranged from 88% to 92% on room air.
His postnatal echocardiography and computed tomograms showed visceral and atrial situs solitus, and levocardia (Figs. 1–3). The systemic and pulmonary veins had normal connections to the right and left atria, respectively. The cardiac chambers and arterial trunks showed grossly abnormal spatial relationships, including right side juxtaposition of the atrial appendages, superoinferior relationship of the ventricles with the left ventricle on top of the right ventricle, and origin of both arterial trunks from the inferiorly located right ventricle, i.e., double outlet right ventricle (DORV). The left atrium was elongated forward, upward, and rightward to connect to the left ventricle in the superior aspect of the right ventricle (Figs. 1D and 3B). The right atrium was positioned normally and was connected to the right ventricle. Therefore, concordant atrioventricular connections were observed through the superiorly located mitral valve and inferiorly located tricuspid valve (https://video1).
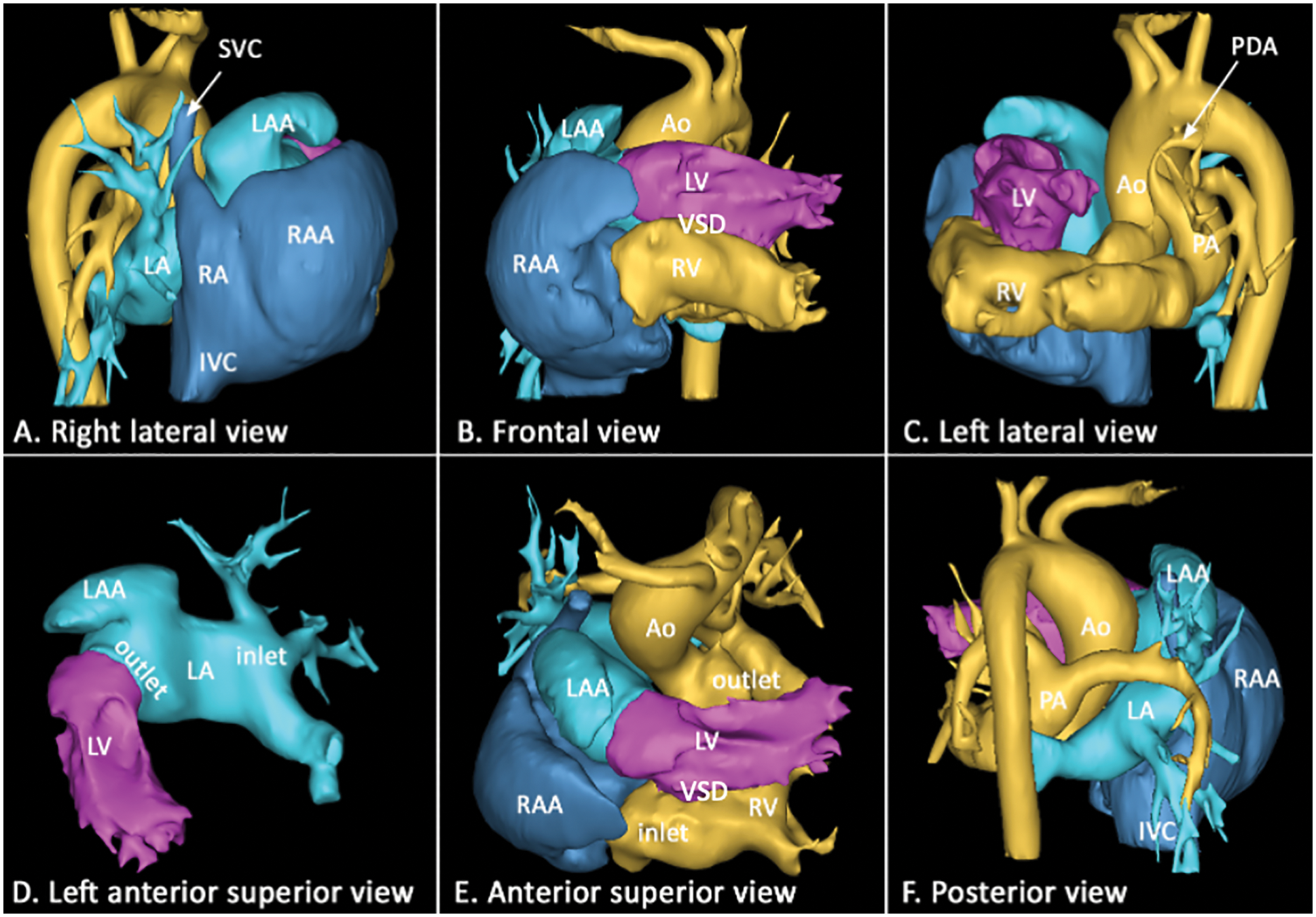
Figure 1: Volume-rendered computed tomographic angiograms obtained in 6 different views showing situs solitus with an unusual interatrial relationship. The left atrium is elongated anteriorly, superiorly, and rightward to connect to the anteriorly located left ventricle. The left atrial appendage is juxtaposed above the right atrial appendage on the right side of the arterial trunks. The left and right atria have concordant connections to the super-inferiorly related left and right ventricles, respectively. Both arterial trunks arise from the inferiorly located right ventricle
Both the mitral and tricuspid valves were balanced in size, without significant regurgitation. The ventricular relationship was similar to that of the L-looped ventricles (Fig. 2A). The right ventricular internal topology showed a left-hand pattern with the observer’s palm being able to be placed facing the right ventricular aspect of the septal surface superiorly, with the thumb directed toward the right ventricular inlet and the fingers directed toward the right ventricular outlet (Fig. 2C). A large perimembranous ventricular septal defect was observed in the horizontally oriented ventricular septum. Both the aorta and pulmonary arterial trunks arose from the posterior aspect of the right ventricle. Both arterial valves were supported by muscular infundibula. The aortic valve was located on the right side, slightly anterior to the pulmonary valve. After both arterial trunks arose backward from the inferiorly located right ventricle, they turned in a right angle superiorly to course upward in the posterior mediastinum (Fig. 2B). The aortic arch was left-sided, unobstructed, and showed normal head and neck branching. The main pulmonary artery was slightly smaller than the ascending aorta and branched into the right and left pulmonary arteries. There was a small left-sided patent ductus arteriosus. The patient’s airway was unobstructed.
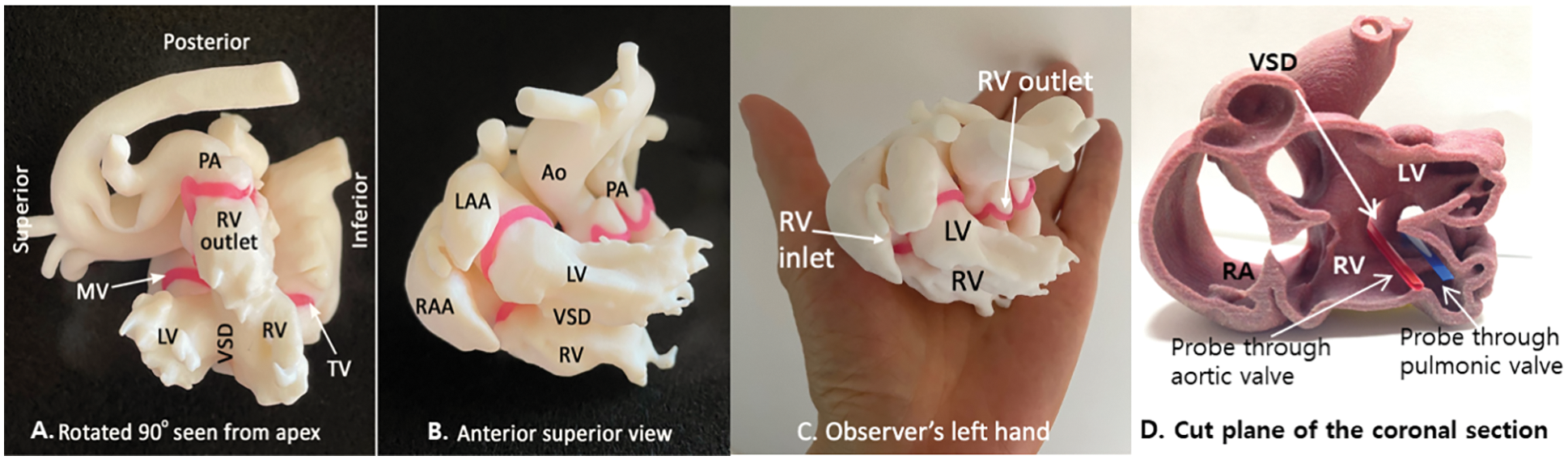
Figure 2: 3D-printed model of the heart. Panel A shows a view from the apex of the ventricles. The heart was rotated 90° counterclockwise to place the ventricular septum vertically oriented in this view. The ventricular relationship is equivalent to that of the L-looped ventricles. Panel B shows the left ventricle (LV) on top of the right ventricle (RV). The right ventricle wraps the left ventricle around from below. Panel C shows the anterior and superior view of the heart with the palm of the observer’s left hand placed below the heart. The palm of the left hand is placed toward the ventricular septum with the thumb directed toward the right ventricular inlet and the fingers directed toward the right ventricular outlet. Therefore, there is a left-hand pattern of the ventricular topology. Panel D is the cut plane of the coronal section visualizing the relationship between the ventricles, ventricular septal defect, and both great arteries. Both the aorta and pulmonary artery arise backward from the inferiorly located right ventricle
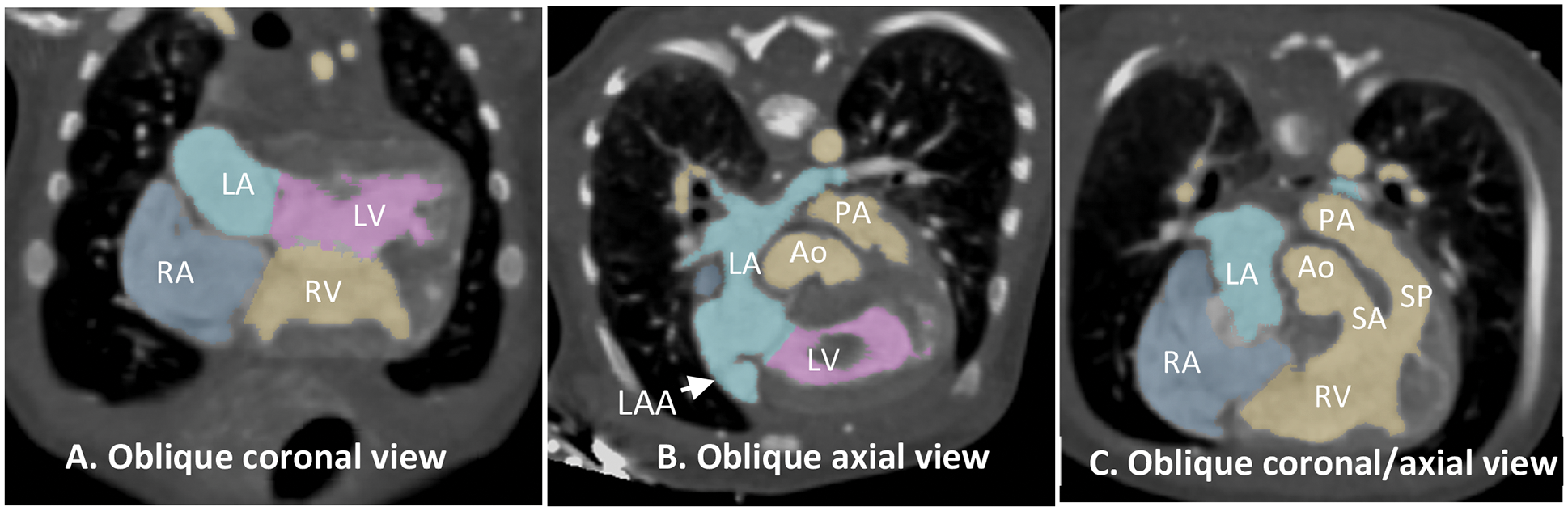
Figure 3: Computed tomographic angiograms reconstructed in oblique planes. (A): Oblique coronal view showing the four chambers of the heart with parallel concordant atrioventricular connections. (B): Oblique axial view showing the left atrium that is elongated anteriorly and superiorly toward the anteriorly located left ventricular (LV) inlet. The left atrial appendage (LAA) is on the right side. (C): Oblique axial/coronal view of the heart showing double-outlet right ventricle (RV). Both aorta (Ao) and pulmonary arterial trunk (PA) are supported by the muscular infundibula
Abbreviations: Ao, aorta; AV, aortic valve; IVC, inferior vena cava; MV, mitral valve; LA, left atrium; LAA, left atrial appendage; LV, left ventricle; PA, pulmonary artery; PDA, patent ductus arteriosus; PV, pulmonary valve; RA, right atrium; RAA, right atrial appendage; RV, right ventricle; SA, subaortic infundibulum; SP, subpulmonary infundibulum; TV, tricuspid valve; VSD, ventricular septal defect.
He initially had mild pulmonary stenosis. However, cardiomegaly and pulmonary congestion progressed into tachypnea and chest retractions. Thus, we performed pulmonary arterial banding one month after birth via thoracotomy. Cardiac catheterization at six months of age revealed good pulmonary arterial beds and adequate mean pulmonary arterial pressure of 13 mmHg; pulmonary vascular resistance was calculated as 2.3 Wood unit m2. Since the patient had a very large, perimembranous inlet extended VSD and deeply positioned great vessels from the inferiorly located RV, we considered that it would be geometrically difficult to perform intracardiac baffling despite both ventricles being sizable. This patient had a unique and highly complex cardiac anomaly, in which surgical decision was difficult. Therefore, 3D modeling, and printing service was outsourced to the Hospital for Sick Children in Toronto where a cardiac radiologist did postprocessing of the anonymized CT images using commercially available software programs (Mimics Medical and 3-Matic Medical, Materialise, Leuven, Belgium) and the models were printed using a commercially available 3D printer (Objet 260 Connex, Stratasys, Rehovot, Israel). We discussed surgical options: biventricular repair vs. Fontan palliation based on 3D-printed model, computed tomography scan, and echocardiography. By careful and extensive examination of the 3D-printed model, we decided to perform Fontan-type palliation due to the horizontal interventricular septal alignment and the spatial relationship of the inferiorly located RV and postero-inferiorly located aorta, which would make the baffling procedure extremely difficult (Fig. 2). At seven months, we performed a bidirectional cavopulmonary shunt and a Damus-Kaye-Stansel procedure to avoid potential subaortic stenosis due to the hypertrophied conal septum. The 3D-printed model indeed helped us understand the complex anatomical relationship between the atria, ventricles, VSD, and great arteries in the heart. The extracardiac conduit Fontan procedure, without fenestration, was performed at 33 months of age. The patient is currently a very active 9-year-old boy whom we follow up at our outpatient clinic.
The case described in this report showed an extremely unusual relationship between the chambers, including concordant atrioventricular connection to L-looped ventricles in the setting of situs solitus and levocardia, right-sided juxtaposition of the atrial appendages, superoinferiorly related ventricles with the left ventricle on top of the right ventricle, and double outlet right ventricle with the arterial trunks inferiorly located in the posterior mediastinum above the diaphragm. Concordant connection of the normally related atria to the L-looped ventricles is extremely rare [3–5]. Anderson et al described that there was disharmony between the atrioventricular connection and segmental combinations in these hearts [4].
The disharmonious connection was associated with the unusually elongated left atrium with its appendage juxtaposed on top of the right atrial appendage, and forward, superior and rightward displacement of the mitral valve annulus. The ventricles are superoinferiorly related and the four chambers of the heart were oriented in the coronal plane instead of the axial one, which is similar to that described in so-called topsy-turvy hearts [6–8]. In contrast to most hearts with superoinferior relationship of the ventricles including topsy-turvy hearts in which the right ventricle is the superior ventricle, the current case had the left ventricle on top of the right ventricle. The origin of the arterial trunks from the ventricle near the diaphragm in topsy–turvy hearts is associated with a low position of the aortic arch causing elongation of the head and neck branches of the aorta and stretching and narrowing of the airway. In the current case, the aortic arch was normally positioned despite the abnormally low position of the aortic root. In addition, there was no airway narrowing. Furthermore, this case cannot be explained by a simple counterclockwise tilting of the cardiac axis because the great vessels were located far posteriorly rather than anteriorly.
The 3D-printed model has been used for providing unequivocal perception of complex heart diseases and simulation before the surgical procedure [9]. This complex heart anatomy, in our case, was challenging to understand and determine whether biventricular repair was possible. The authors and colleagues at our center agreed upon the usefulness of 3D printing in the current case. Since the two ventricles were balanced in this complex DORV anatomy, we discussed the possibility of two ventricular repairs by baffling from the VSD to the aorta based on 3D-printed model. This model helped us to easily understand intraventricular anatomy and spatial relationship. Therefore, surgical planning could be made more readily. We decided to perform the Fontan palliation procedure due to the twisted ventriculoarterial plane and far posteriorly located great arteries and were able to avoid unnecessary ventriculotomy to close the VSD with the aid of 3D-model. Obviously, the 3D-printed model provided us with a more intuitive understanding of the spatial orientation of this complex anatomy.
We report a rare case of superior-inferior ventricles with concordant atrioventricular connection, L-looped ventricle, and a posteroinferiorly tilted aorta and pulmonary artery. The 3D-printed model clearly showed the anatomy and relationship of the atria, ventricles, and great arteries.
Acknowledgement: The authors thank Shi-Joon Yoo for providing the 3D-printed modelling service and valuable comments, and Susan Taejung Kim for English language editing.
Data Sharing: Deidentified participant data (including d. Birth Defects: Original Article Series,ata dictionaries) will be shared.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflict of interest to report regarding the present study.
1. Van praagh, R. (1972). The segmental approach to diagnosis of congenital heart disease. In: Birth defects: Original Article Series, vol. 8, pp. 4–23. Baltimore: Williams & Wilkins. [Google Scholar]
2. Yoo, S. J., Anderson, R. H. (2020). Abnormal positions and relationships of the heart. In: Wernovsky, G. (Eds.Anderson’s pediatric cardiology, 4th edition, pp. 913–926. USA: Elsevier. [Google Scholar]
3. Seo, J. W., Choe, G. Y., Chi, J. G. (1989). An unusual ventricular loop associated with right juxtaposition of the atrial appendages. International Journal of Cardiology, 25(2), 219–233. DOI 10.1016/0167-5273(89)90111-3. [Google Scholar] [CrossRef]
4. Anderson, R. H., Smith, A., Wilkinson, J. L. (1987). Disharmony between atrioventricular connections and segmental combinations: Unusual variants of “crisscross” hearts. Journal of the American College of Cardiology, 10(6), 1274–1277. DOI 10.1016/S0735-1097(87)80130-4. [Google Scholar] [CrossRef]
5. Weinberg, P. M., van Praagh, R., Wagner, H. R., Cuaso, C. C. (1980). New form of criss-cross atrioventricular relation: An expanded view of the meaning of D and L-loops. London: World Congress of Pediatric Cardiology. [Google Scholar]
6. Freedom, R. M., Culham, J. A. G., Moes, C. A. F. (1984). Angiography of congenital heart disease. New York: Macmillan Publishing Company. [Google Scholar]
7. Jaeggi, E., Chitayat, D., Golding, F., Kim, P., Yoo, S. J. (2008). Prenatal diagnosis of topsy-turvy heart. Cardiology in the Young, 18(3), 337–342. DOI 10.1017/S1047951108002308. [Google Scholar] [CrossRef]
8. Güzeltaş, A., Öztürk, E., Diker, M. (2013). Topsy-turvy heart: A very rare case of superoinferior ventricle. Pediatric Cardiology, 34(8), 2096–2098. DOI 10.1007/s00246-013-0656-x. [Google Scholar] [CrossRef]
9. Yoo, S. J., van Arsdell, G. S., (2018). 3D printing in surgical management of double outlet right ventricle. Frontiers in Pediatrics, 10(5). DOI 10.3389/fped.2017.00289. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |