
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE
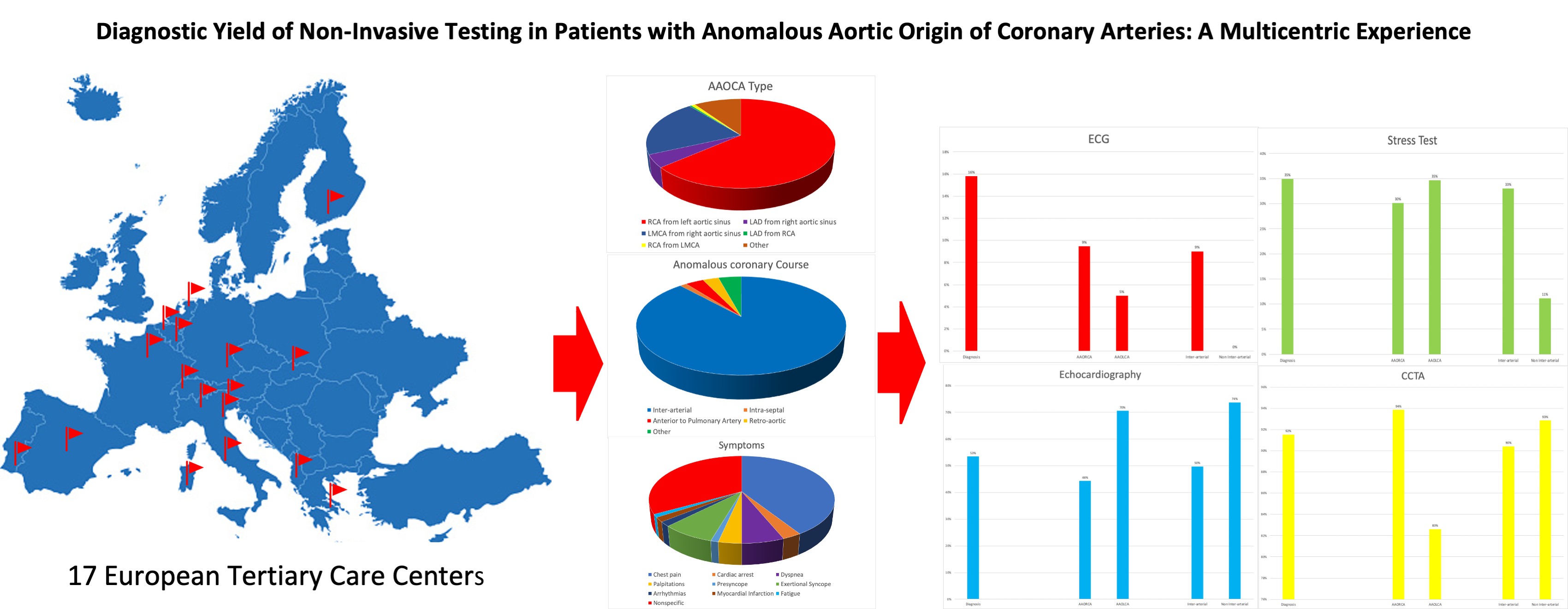
Diagnostic Yield of Non-Invasive Testing in Patients with Anomalous Aortic Origin of Coronary Arteries: A Multicentric Experience
1 Department of Cardio-Thoracic, Vascular Sciences and Public Health, University of Padova, Padova, Italy
2 Department of Woman and Child’s Health, Pediatric Cardiology, University of Padova, Padova, Italy
3 Athens Heart Surgery Institute and Iaso Children’s Hospital, Athens, Greece
4 Department for Cardiovascular Surgery, University Medical Center, Leiden, The Netherlands
5 Department for Cardiovascular Surgery, University Hospital Bern, Bern, Switzerland
6 Department of Congenital Cardiac Surgery, IRCCS Policlinico San Donato, San Donato Milanese, Italy
7 Department of Pediatric Cardiology and Congenital Heart Disease, Hôpital Marie Lannelongue, Université Paris-Sud, Le Plessis-Robinson, France
8 Deutsch Herz Zentrum, Munich, Germany
9 Katholieke Universiteit Leuven, Leuven, Belgium
10 Cardiothoracic Surgery Hospital de Santa Marta Rua, Lisbon, Portugal
11 Department of Pediatric Cardiothoracic Surgery, Children’s Hospital of Georgia, Georgia, USA
12 Department of Cardiac Surgery, University Hospital Ghent, Ghent, Belgium
13 Division of Cardiac Surgery, University Hospital Center of Tirana, Tirana, Albania
14 Department of Pediatric Cardiac Surgery, Hospital for Children and Adolescents, University of Helsinki, Helsinki, Finland
15 Congenital Cardiac Surgery Department, Hospital Universitario La Paz, Madrid, Spain
16 Department of Pediatric Cardiac Surgery, National Institute of Cardio-Vascular Diseases-Children’s Heart Center, Bratislava, Slovakia
17 Division of Pediatric Cardiology, Ospedale Brotzu, Cagliari, Italy
18 Division of Sport Medicine, Ospedale Ca’ Foncello, Treviso, Italy
19 Department of Medicine, Radiology Clinic, University of Padua Medical School, Padova, Italy
* Corresponding Author: Massimo A. Padalino. Email:
Congenital Heart Disease 2022, 17(4), 375-385. https://doi.org/10.32604/chd.2022.019385
Received 23 January 2022; Accepted 15 May 2022; Issue published 04 July 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Anomalous aortic origin of a coronary artery (AAOCA) is a congenital heart disease with a 0.3%−0.5% prevalence. Diagnosis is challenging due to nonspecific clinical presentation. Risk stratification and treatment are currently based on expert consensus and single-center case series. Methods: Demographical and clinical data of AAOCA patients from 17 tertiary-care centers were analyzed. Diagnostic imaging studies (Bidimensional echocardiography, coronary computed tomography angiography [CCTA] were collected. Clinical correlations with anomalous coronary course and origin were evaluated. Results: Data from 239 patients (42% males, mean age 15 y) affected by AAOCA were collected; 154 had AAOCA involving the right coronary artery (AAORCA), 62 the left (AAOLCA), 23 other anomalies. 211 (88%) presented with an inter-arterial course. Basal electrocardiogram (ECG) was abnormal in 37 (16%). AAOCA was detected by transthoracic echocardiography and CCTA in 53% and 92% of patients, respectively. Half of the patients reported cardiac symptoms (119/239; 50%), mostly during exercise in 121/178 (68%). An ischemic response was demonstrated in 37/106 (35%) and 16/31 (52%) of patients undergoing ECG stress test and stress-rest single positron emission cardiac tomography. Compared with AAORCA, patients with AAOLCA presented more frequently with syncope (18% vs. 5%, P = 0.002), in particular when associated with inter-arterial course (22% vs. 5%, P < 0.001). Conclusion: Diagnosis of AAOCA is a clinical challenge due to nonspecific clinical presentations and low sensitivity of first-line cardiac screening exams. Syncope seems to be strictly correlated to AAOLCA with inter-arterial course.Graphic Abstract
Keywords
Cite This Article
 Copyright © 2022 The Author(s). Published by Tech Science Press.
Copyright © 2022 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools