
 Submit a Paper
Submit a Paper Open Access
Open Access
ARTICLE
Research on the Association between Fear of Cancer Recurrence in Young Breast Cancer Patients and Adult Attachment and Self-Disclosure
Department of Breast Cancer Surgery, Jiangsu Cancer Hospital, The Affliated Cancer Hospital of Nanjing Medical University, Jiangsu Institute of Cancer Research, Nanjing, 210009, China
* Corresponding Author: Minghui Wang. Email:
Psycho-Oncologie 2024, 18(3), 169-179. https://doi.org/10.32604/po.2024.052703
Received 11 April 2024; Accepted 01 July 2024; Issue published 12 September 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Although fear of cancer recurrence (FCR) is the most important factor affecting the life quality of young breast cancer patients, and it may be affected by the patient’s personality, marital relationship and communication, there is a lack of research on the relationship between adult attachment, self-disclosure and FCR in patients. This study investigated the current situation of FCR in young breast cancer patients, its correlation with adult attachment and self-disclosure and its influencing factors, in order to predict the impact of adult attachment and self-disclosure of patients to spouse on FCR. Methods: A survey was conducted on 126 breast cancer patients at our hospital using the General Information Questionnaire (GIQ), Fear of Progression Questionnaire-Short Form (FoP-Q-SF), Experiences in Close Relationships inventory (ECR), and Distress Disclosure Index (DDI). The study analyzed the status of FCR among young breast cancer patients and its correlation with adult attachment and self-disclosure, along with its influencing factors. Results: Among the 126 young breast cancer patients, 50 had a FoP-Q-SF score <34 (normal group), while 76 had a FoP-Q-SF score ≥34 (FCR positive group), with an FCR incidence rate of 60.32%. Univariate analysis showed statistically significant differences between the two groups in terms of FoP-Q-SF score, ECR score, attachment anxiety score, attachment avoidance score, DDI score, age, educational level, employment status, per capita monthly income, and treatment method (p < 0.05). Correlation analysis revealed that FoP-Q-SF scores were positively correlated with attachment anxiety score, attachment avoidance score, ECR scores and negatively correlated with DDI scores (p < 0.05). Linear regression analysis indicated that age, per capita monthly income, treatment method, attachment anxiety, attachment avoidance and self-disclosure level were negative predictors of FoP-Q-SF scores in young breast cancer patients (p < 0.05). Conclusion: The incidence rate of FCR among young breast cancer patients is high. There is a positive correlation between adult attachment and the level of FCR, and a negative correlation between the level of self-disclosure and FCR. Patients with lower per capita monthly income, more complex treatment methods, higher level of attachment anxiety, higher level of attachment avoidance and lower DDI scores had higher FoP-Q-SF scores.Keywords
Breast cancer, a malignant tumor originating from ductal or mammary epithelium [1], is one of the most common malignancies in women [2]. According to the World Health Organization’s International Agency for Research on Cancer statistics from 2020, there were 2.26 million new cases of breast cancer globally [3], with a trend towards younger age at diagnosis. It is reported that up to 18.8% of patients are under the age of 40 [4]. With the continuous development of medical technology, including surgery, radiotherapy, and chemotherapy, the number of breast cancer survivors in China is gradually increasing [5]. However, studies have shown that the recurrence rate within three years post-surgery can still reach about 30% [6]. Fear of Cancer Recurrence (FCR) has become the most severe factor affecting the mental health of breast cancer patients. FCR refers to the anxiety caused by the fear of cancer progression or recurrence [7,8]. A survey indicate that the incidence of FCR in young breast cancer patients can be as high as 80% [9], which can severely affect their mental health and quality of life. This may cause patients to lose confidence in their treatment, leading to poor prognosis.
Another factor associated with the physical and mental health and quality of life of breast cancer patients is adult attachment [10–12]. Study has shown that breast cancer patients with different types of attachment exhibit differences in seeking help, expressing emotions, and perceiving their illness. These differences significantly impact psychological adjustment, intimate relationships, and patient prognosis for both the patients and their spouse or primary caregivers [13]. A study from Hungary [14] proved that high attachment anxiety and high attachment avoidance in breast cancer patients reflect low relationship satisfaction and sexual satisfaction, and monitoring and adjusting patients’ physical, psychological and personality characteristics may help improve patients’ quality of life, thereby reducing patients’ FCR. Patients with avoidant attachment tend to avoid discussing their illness and emotional issues, leading to an accumulation of FCR. On the other hand, patients with anxious attachment excessively rely on the support of others, and when they perceive a lack of support, their FCR significantly increases [15].
Self-disclosure can also have an impact on patients’ psychology and quality of life. Zhao et al. [16] believed that self-disclosure is the process through which individuals share their thoughts, feelings, and experiences with others, serving as an effective psychological therapy to obtain social support and alleviate negative emotions [16]. In marital relationships, self-disclosure helps both partners better understand and support each other, enhancing the quality of the marriage. A good marital relationship and partner support have a positive impact on alleviating the fear of cancer recurrence in breast cancer patients. However, due to various reasons such as Chinese young women being ashamed to talk about breasts and bearing the burden of family, they suppress their self-disclosure, thus suppressing the negative emotions of FCR in their hearts and cannot be properly relieved [17]. Soriano et al. [18] found that communication style induced suppression of self-disclosure in patients and spouses was associated with high levels of fear of cancer recurrence. Therefore, actively encouraging and supporting breast cancer patients to engage in self-disclosure is of great significance for alleviating FCR, improving mental health, and enhancing the quality of life [19].
This is a single-center retrospective study, aims to analyze the current state of FCR among young breast cancer patients, its influencing factors, and its correlation with adult attachment and self-disclosure. This could help clinical medical staff to use psychological interventions which is compatible with Chinese marriage mode to improve the intimate relationships between patients and their spouses, reduce patients’ FCR, enhance treatment confidence, increase social support, and improve treatment compliance.
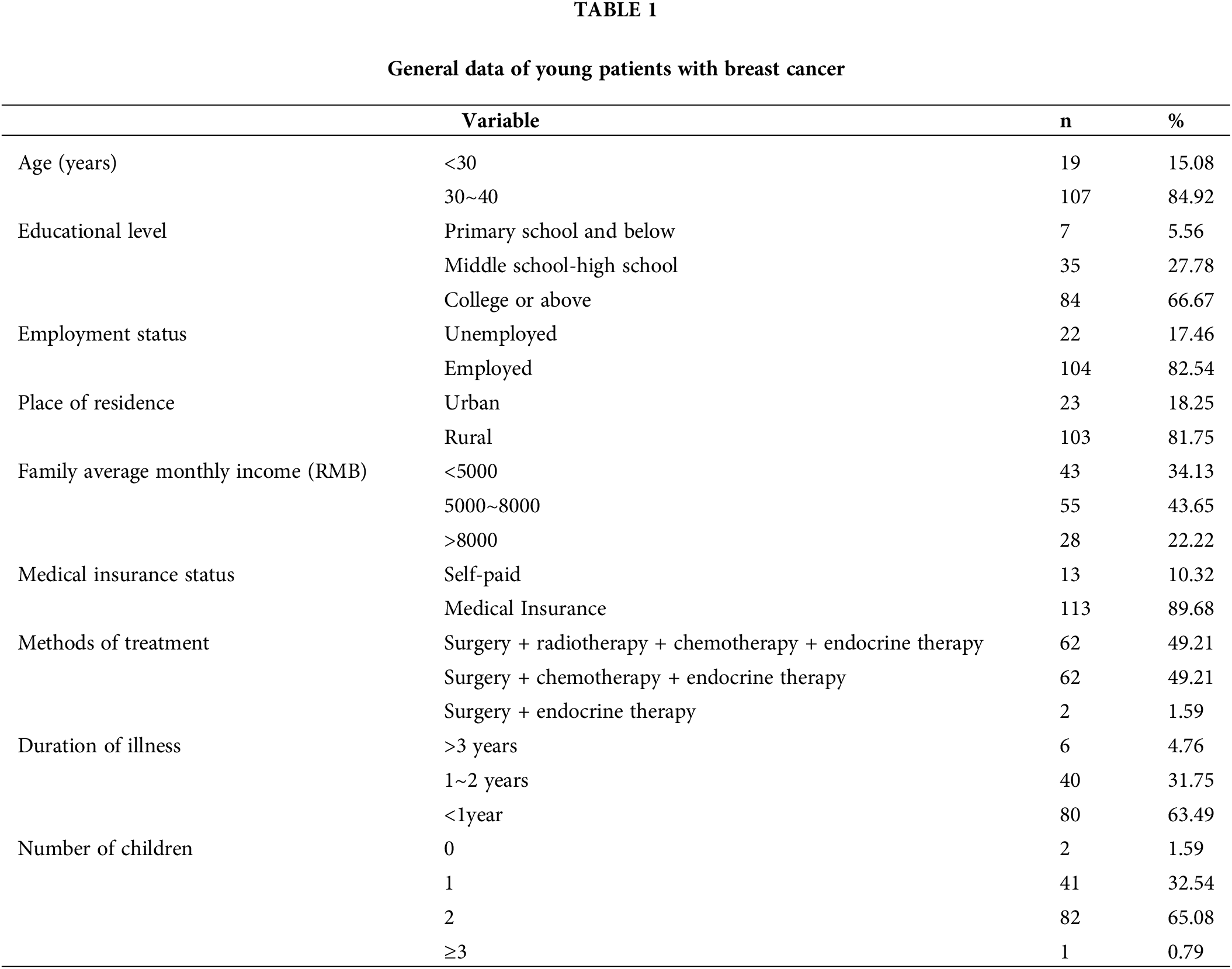
A total of 126 young breast cancer patients (They are all female and married) who received inpatient treatment in the breast tumor department of Jiangsu Cancer Hospital from January 2022 to January 2023 were selected as the study subjects. The average age of the patients was (33.16 ± 3.40) years. Other general information is presented in Table 1. The patients were surveyed using general information questionnaires (GIQ), the Fear of Progression Questionnaire-Short Form (FoP-Q-SF), the Experiences in Close Relationships Scale (ECR), and the Distress Disclosure Index (DDI). Based on the assessment results of the FoP-Q-SF, patients were divided into a normal group and an FCR-positive group.
Inclusion criteria: (1) Pathologically diagnosed with breast cancer. (2) Patients were informed about the study and signed a consent form. (3) Age ≥20 years and ≤40 years. (4) Conscious and able to complete the questionnaire either in writing or orally. Exclusion criteria: (1) Patients with other severe diseases. (2) Patients who have had or are combined with other tumors. (3) Patients with cancer recurrence or metastasis. (4) Patients with incomplete data or those who withdrew from the study midway.
General information questionnaire
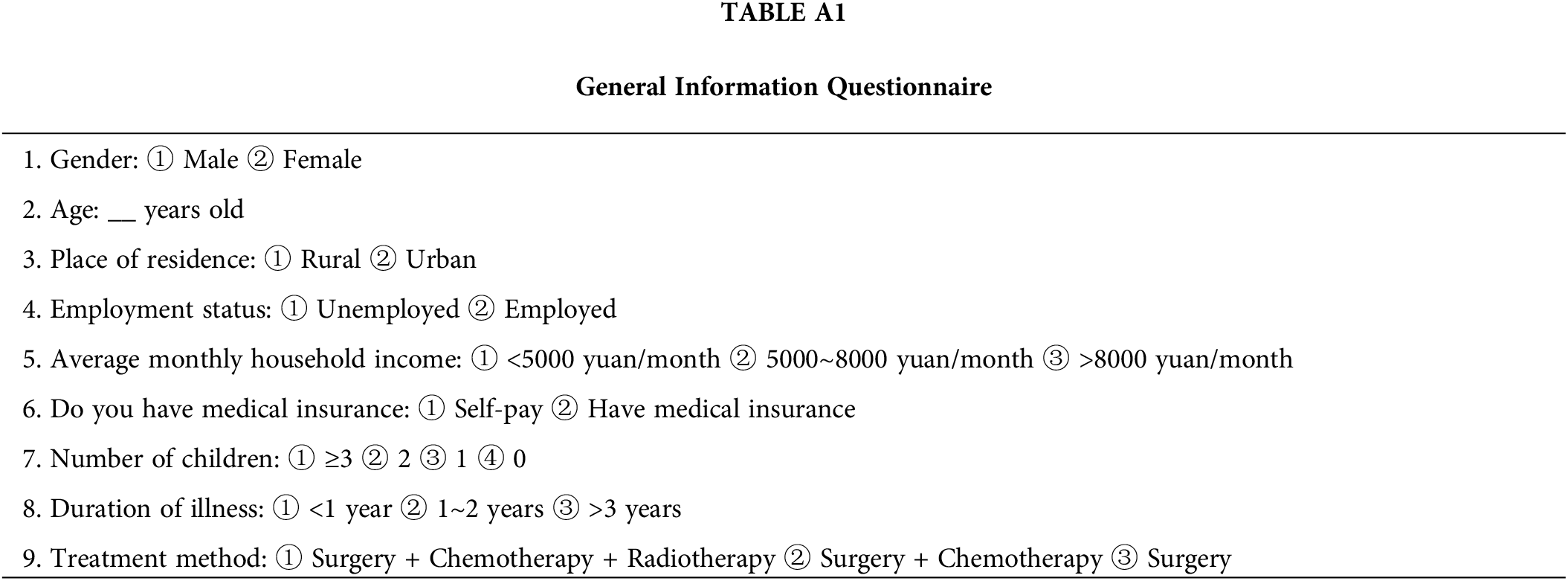
A self-designed questionnaire was used to collect the basic information of the patients, including age (<30 years old, 30–40 years old), employment status (unemployed, employed), place of residence (rural, urban), family average monthly income (<5000 RMB/month, 5000~8000 RMB/month, >8000 RMB/month), medical insurance status (self-paid, insured), treatment method (surgery + chemotherapy + radiotherapy+ endocrine therapy, surgery + chemotherapy+ endocrine therapy, surgery + endocrine therapy), duration of illness (<1 year, 1~2 years, >3 years), and number of children (≥3, 2, 1, 0) (Table A1).
Fear of progression questionnaire-short form (FoP-Q-SF)
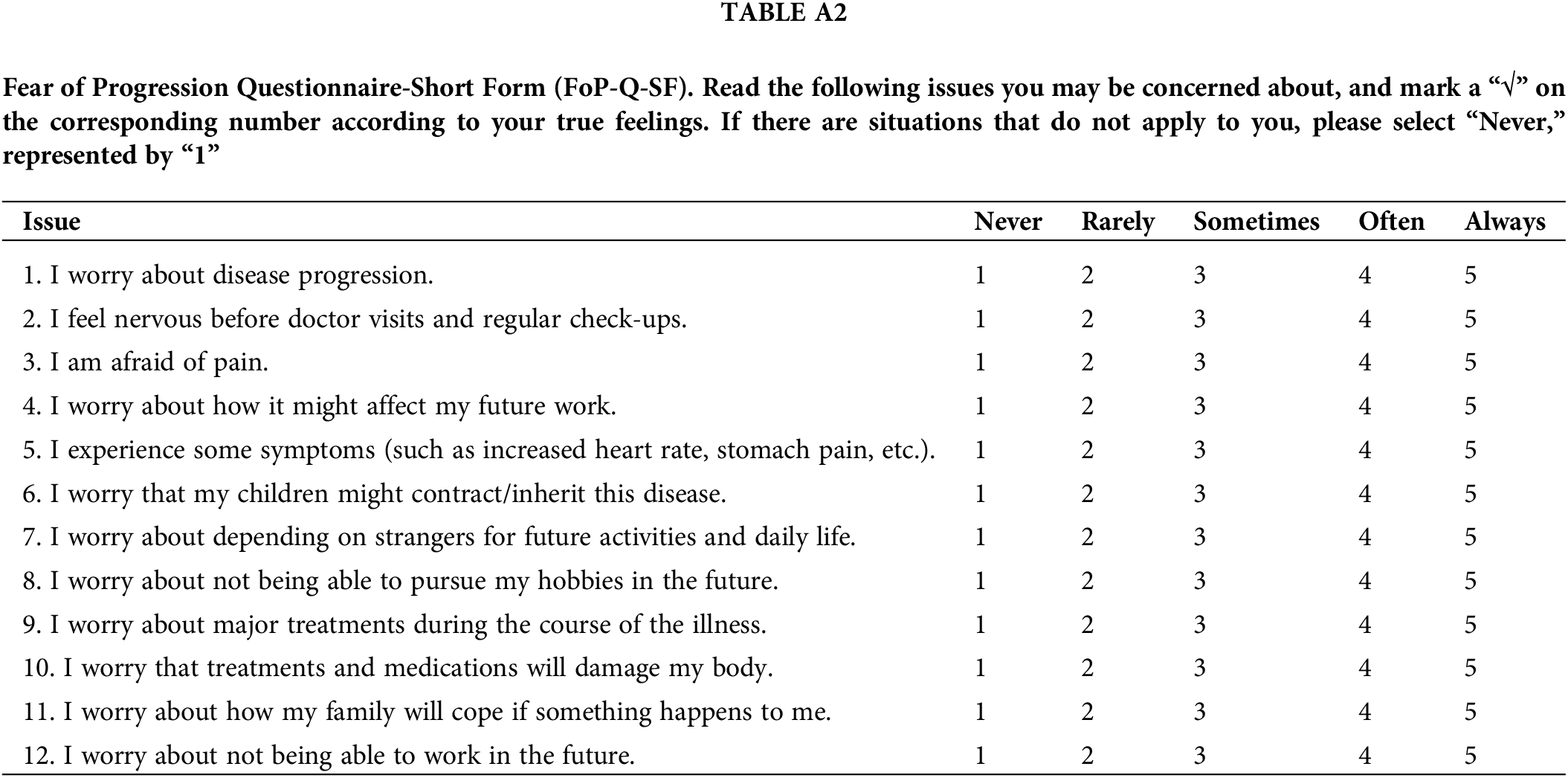
This questionnaire is designed to measure the multidimensional fear of recurrence in breast cancer patients (Table A2) [20]. It consists of 12 items divided into two dimensions: physical health and social-family. It uses a Likert 5-point scoring system, ranging from “never” to “always”, with total scores ranging from 12 to 60. Higher scores indicate higher levels of fear of recurrence. A score of ≥34 points is considered positive for fear of cancer recurrence. The scale has a Cronbach’s alpha coefficient of 0.856, with dimension-specific Cronbach’s alpha coefficients of 0.838 and 0.842, indicating good reliability and validity.
Experiences in close relationships inventory (ECR)
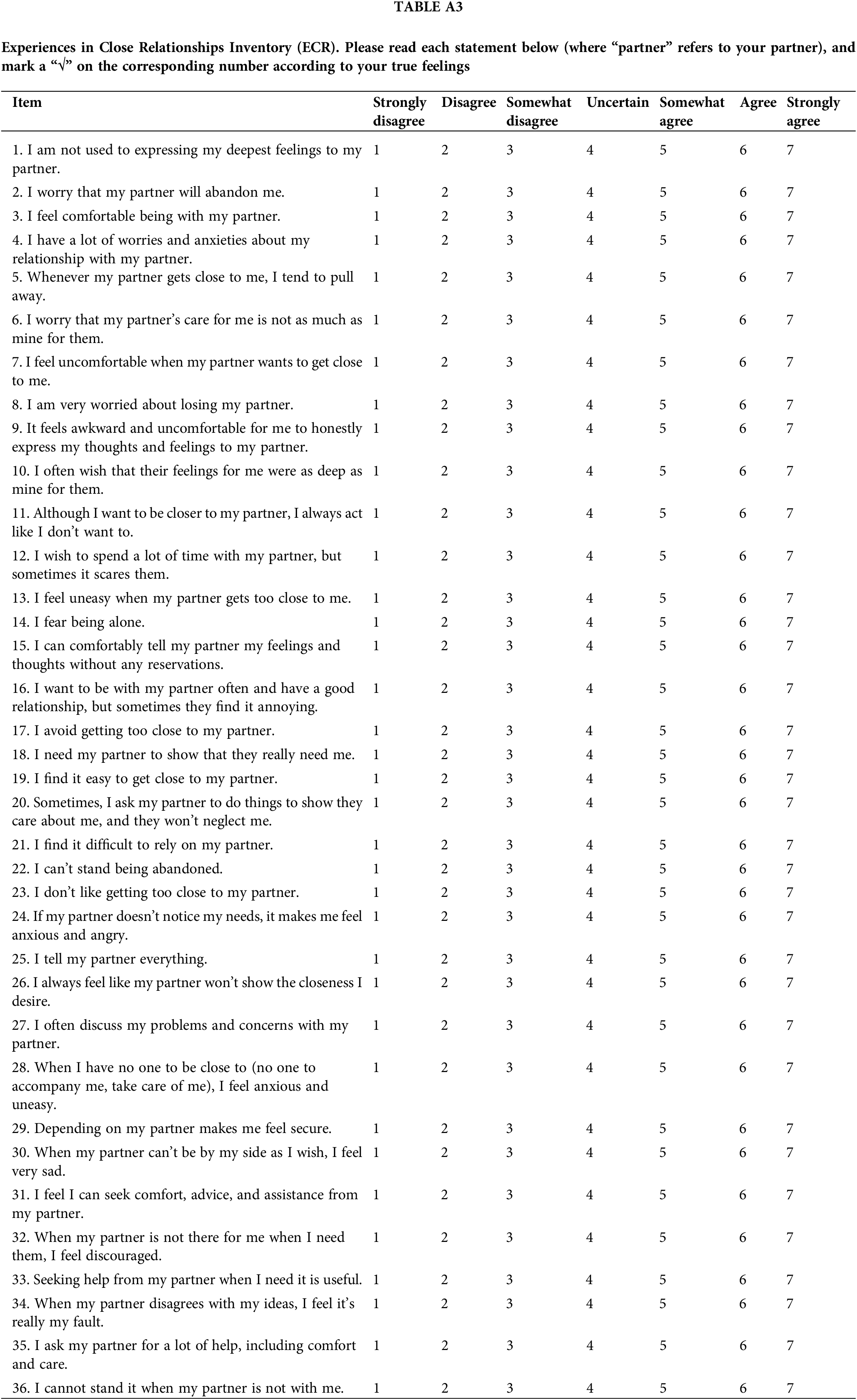
This inventory is used to measure the adult attachment style in intimate relationships of breast cancer patients, focusing on the relationship between the patient and her husband. It is the most widely used universal scale in the field of marital attachment (Table A3) [21,22]. The inventory consists of 36 items, divided into two dimensions: attachment avoidance and attachment anxiety, with 18 items each. It employs a Likert 7-point scoring system, ranging from “strongly disagree” to “strongly agree” Higher scores indicate higher levels of attachment avoidance and attachment anxiety. The inventory has a Cronbach’s alpha coefficient of 0.756, with dimension-specific Cronbach’s alpha coefficients of 0.868 for attachment avoidance and 0.794 for attachment anxiety, indicating good reliability and validity.
Distress disclosure index (DDI)
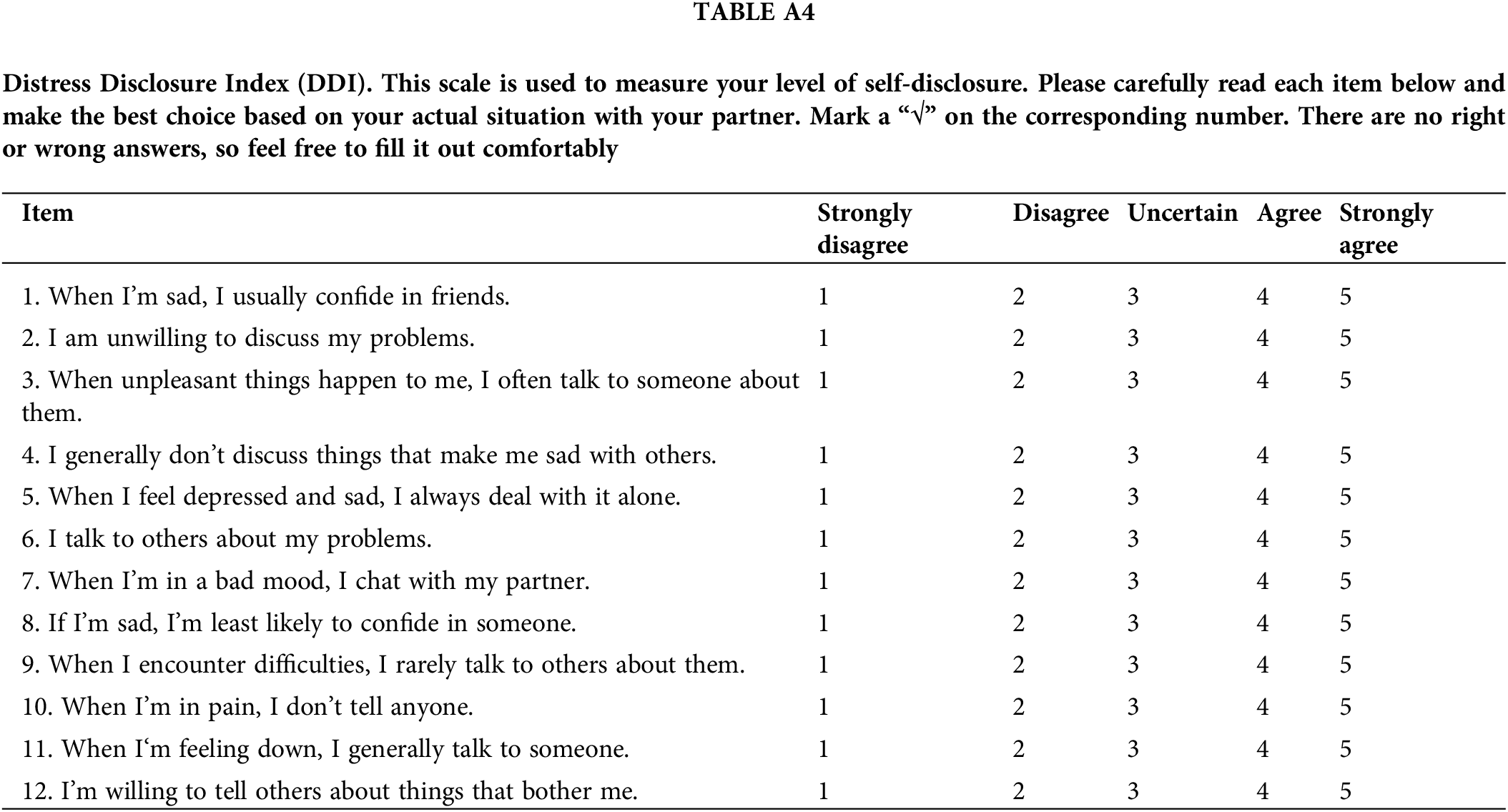
This scale is used to measure the extent to which breast cancer patients disclose their inner distress or psychological troubles to their spouse (Table A4) [16]. It was introduced into China by Li et al. in 2009 and has been widely used [23]. There are 12 items in the scale, including two dimensions of self-disclosure and self-concealment, and each item adopts Likert 5-level scoring method, from low to high, from “strongly disagree” to “strongly agree”, self-disclosure dimension is positive score, and self-concealment dimension is reverse score. The total score ranges from 12 to 60. The higher the score, the higher the willingness and degree of disclosure with others, among which 12 to 29 were low self-disclosure, 30 to 44 were medium self-disclosure, and 45 to 60 were high self-disclosure [24]. The scale has a Cronbach’s alpha coefficient of 0.866, indicating good reliability and validity.
The survey was conducted by three researchers who had undergone uniform training to guide patients in filling out the questionnaires themselves. Before filling out the questionnaires, patients were informed of the purpose, significance, filling method, and precautions of the study, and were advised to answer based on their actual situations. The survey process was conducted in a private setting to avoid interference from others and to protect the privacy of the patients. If patients encountered questions they did not understand, the researchers explained patiently to avoid subjective and leading answers. If a patient’s response was unclear or uncertain, the researchers would ask repeatedly to confirm the answer before it was recorded in the questionnaire. After completion, the researchers checked the questionnaires on the spot. The survey was conducted from January 2022 to January 2023. A questionnaire survey was conducted for each patient during the period when they were diagnosed with breast cancer and received surgery or chemoradiotherapy. A total of 137 questionnaires were distributed, and after excluding 11 invalid questionnaires (missing significant content), 126 valid questionnaires were collected.
Data entry was performed using Excel software, and the data were imported into SPSS 26.0 software for processing and analysis. Breast cancer patients were divided into a fear of recurrence positive group and a normal group based on the FoP-Q-SF scores of ≥34 points. Categorical variables were presented as [n(%)], and comparisons between groups were made using the χ2 test. Continuous variables were tested for normality; those conforming to a normal distribution were presented as
Univariate analysis of variables in the fear of recurrence positive group and normal group among young breast cancer patients
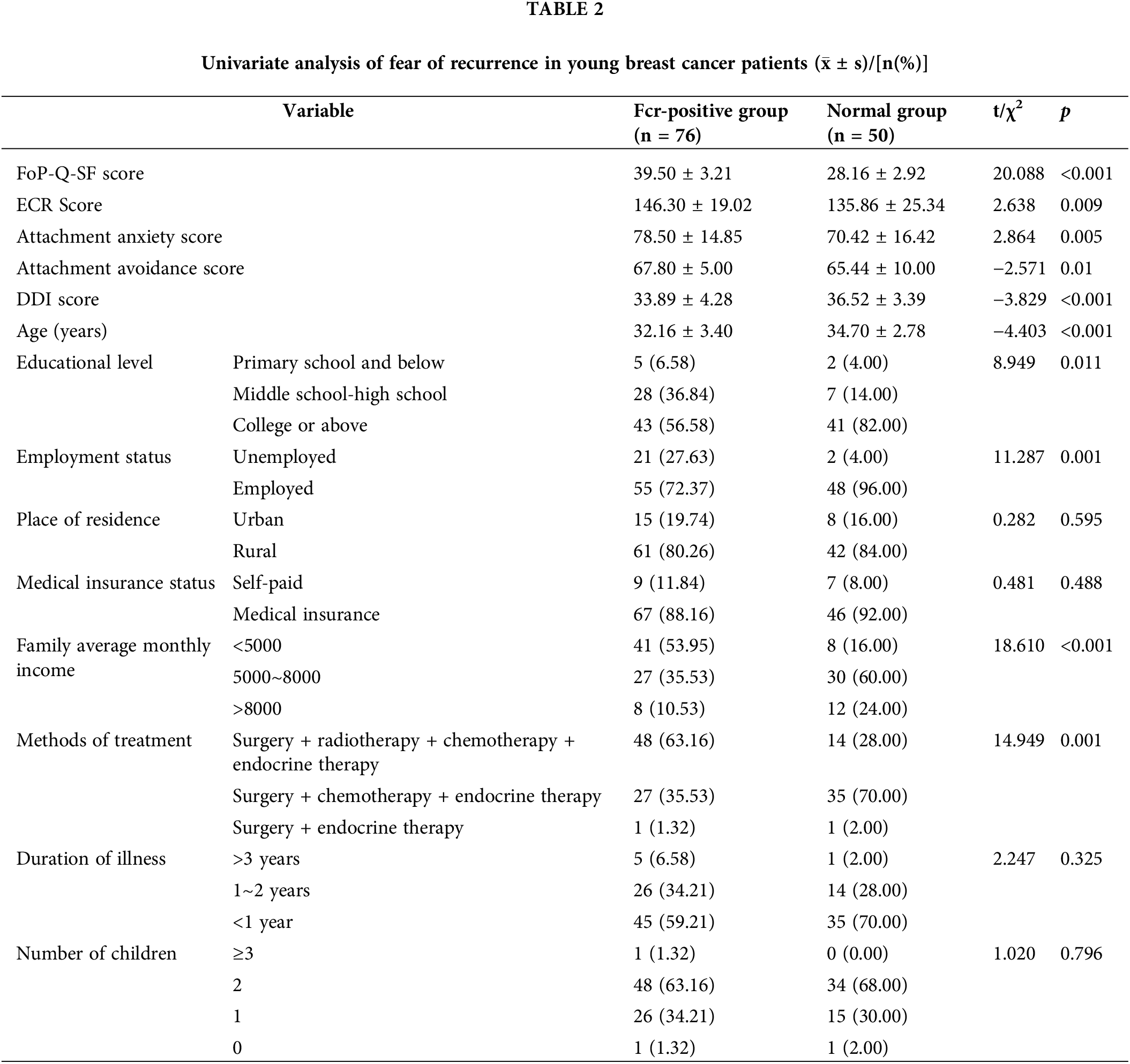
Based on a FoP-Q-SF score of ≥34, young breast cancer patients were divided into an FCR positive group (76 patients) and a normal group (50 patients), with an FCR incidence rate of 60.32%. There were no significant differences between the FCR positive group and the normal group in terms of place of residence, medical insurance status, duration of illness, and number of children (p > 0.05). Significant differences were observed in FoP-Q-SF scores, ECR scores, Attachment anxiety score, Attachment avoidance score, DDI scores, age, educational level, employment status, average monthly income per person, and treatment methods (p < 0.05), as shown in Table 2.
Correlation analysis between FoP-Q-SF Scores and ECR scores, DDI scores among young breast cancer patients
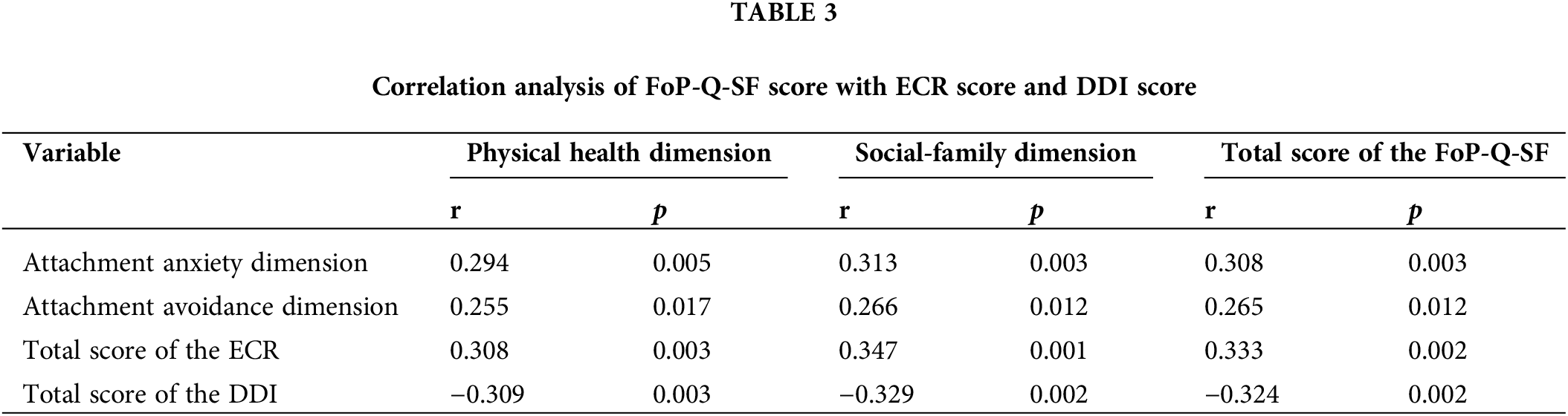
According to the Pearson correlation analysis, the scores of the physical health dimension, the social-family dimension, and the total score of the FoP-Q-SF were significantly positively correlated with the scores of the attachment anxiety dimension, attachment avoidance dimension, and the total score of the ECR (p < 0.05 for all). At the same time, the scores of the physical health dimension, the social-family dimension, and the total score of the FoP-Q-SF were significantly negatively correlated with the DDI scores (p < 0.05). See Table 3.
Analysis of independent risk factors for fear of recurrence in young breast cancer patients
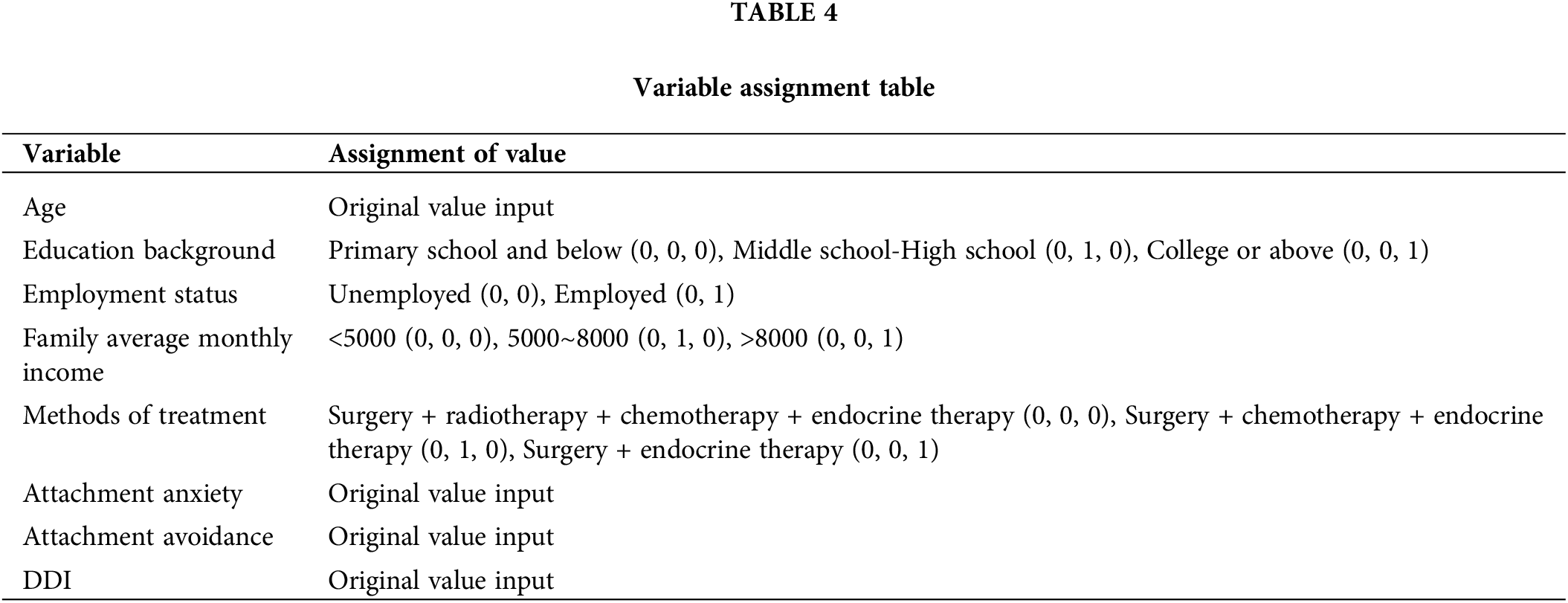
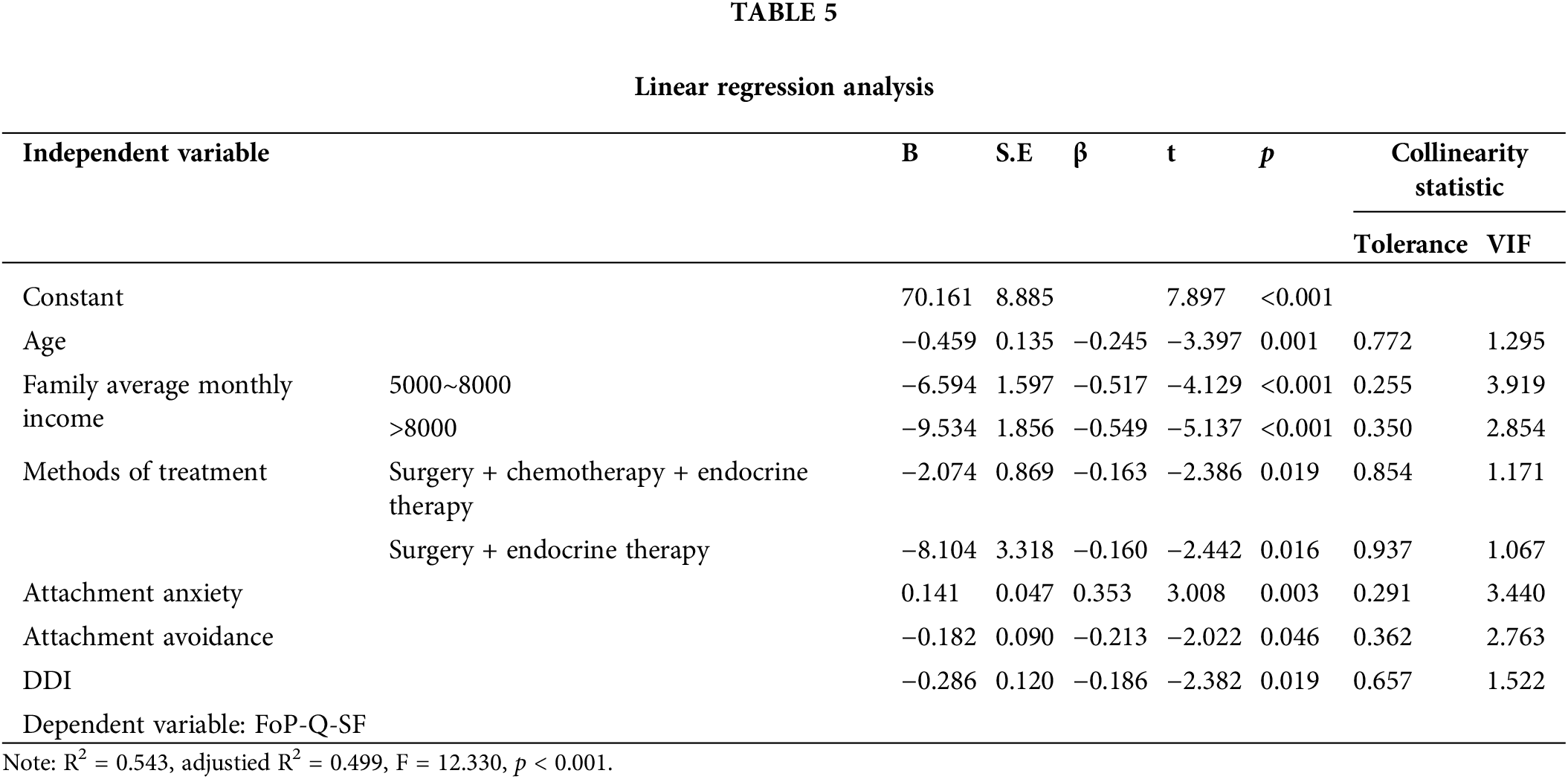
For the categorical variables that showed significant differences in the univariate analysis between the FCR positive group and the normal group, dummy variables were set up, and continuous variables were entered in their original form, as shown in Table 4. Linear regression analysis was utilized; the results indicated that age, average monthly income per person, treatment method, attachment anxiety, attachment avoidance, and self-disclosure were incorporated into the regression equation, suggesting that these six variables have an impact on the FoP-Q-SF scores of young breast cancer patients. The regression analysis model had a fit of R2 = 0.543 indicating that the age, average monthly income per person, treatment method, attachment anxiety, attachment avoidance and DDI scores could explain 54.3% of the variance in FoP-Q-SF scores. ANOVA analysis of the regression equation was significant (F = 12.330, p < 0.001), as shown in Table 5.
Patients experiencing fear of cancer recurrence during treatment may feel burdened, develop negative and apathetic attitudes towards self-management, and encounter challenges in their marital relationships. In severe cases, this can even lead to suicidal tendencies [25,26]. It is crucial for clinical medical staff to monitor patients’ FCR and provide timely and effective interventions.
In this study, the incidence of FCR (60.32%) in young breast cancer patients was slightly higher than that reported by Guo et al. [27], which was 53.8%. This discrepancy may be attributed to the fact that the participants in this study were all under 40 years old. Younger individuals often bear the responsibility of supporting their families, making a cancer diagnosis more unexpected and difficult to accept compared to the elderly. Some studies have indicated that FCR in breast cancer patients decreases with age [28]. Further linear regression analysis in this study included age as a variable, showing that it impacts the FCR score. The findings suggest that the younger the breast cancer patient, the more severe the FCR.
In addition to age, per capita monthly income and treatment methods are also factors affecting FCR in young breast cancer patients. Per capita monthly income is a negative predictor of FoP-Q-SF, indicating that lower per capita monthly income is associated with more severe FCR. This may be related to the extended treatment duration and higher costs of breast cancer treatment compared to common diseases, which imposes a greater economic burden on families. Li et al. [29] also highlighted that reducing the economic burden through medical insurance and social support can significantly lower the level of FCR among breast cancer patients. The treatment method also had a significant negative predictive effect on the FoP-Q-SF scores of young breast cancer patients. Different conditions and stages of breast cancer require various treatment methods. In this study, the main treatments consisted of surgery and radiotherapy/chemotherapy. More complex treatment methods lead to side effects such as damage, pain, nausea, vomiting, hair loss, skin damage, and bone marrow suppression, increasing patients’ awareness of the severity of the disease and making them more prone to experiencing negative emotions such as FCR and anxiety [30].
Regarding the effects of adult attachment and self-disclosure on FCR in young breast cancer patients, this study found that attachment anxiety score, attachment avoidance score, adult attachment total score, and self-disclosure were significantly correlated with FCR through Pearson or Spearman correlation analysis. Further linear regression analysis revealed that higher degrees of attachment anxiety and attachment avoidance, coupled with lower levels of self-disclosure, were associated with higher levels of FCR. Increasing evidence [18,22,31] has demonstrated that intimacy is related to FCR, with adult attachment and self-disclosure impacting marital intimacy.
Young breast cancer patients often experience fear in the face of their diagnosis. Providing appropriate resources can help patients better confront these challenges, with spouses representing a crucial social support resource [31]. Adult attachment influences marital relationship satisfaction, which in turn affects the occurrence and degree of FCR [31,32]. Karbowa-Plowens highlights that individuals with attachment anxiety tend to rely excessively on others and lack self-confidence, hindering their self-management ability. On the other hand, patients with attachment avoidance are more inclined to suppress themselves, enforce independence, and avoid communication with others. This limited psychological endurance can lead to collapse from long-term depression, making it challenging for such patients to establish good nurse-patient relationships and receive effective treatment guidance. Both attachment styles increase patients’ negative emotions, and prolonged unresolved issues can exacerbate anxiety and depression, further affecting FCR [33]. Therefore, clinical healthcare workers should understand the relationship between adult attachment and FCR and adopt effective intervention measures to help patients and their spouses form a secure attachment pattern according to different attachment types. This approach can reduce patients’ FCR and improve the satisfaction of the marital relationship.
Spouses of Chinese breast cancer patients often underestimate the psychological pressure experienced by the patients, leading to a tendency to overlook their feelings. When patients attempt to confide in their spouse or family members but receive no response, they tend to withdraw emotionally, which is detrimental to their recovery [16]. Zhou et al.’s study [19] demonstrated that marital self-disclosure intervention for cancer patients can enhance patients’ psychological resilience, improve marital quality, alleviate patient anxiety, and consequently reduce the degree of FCR in cancer patients. Therefore, nursing staff should recognize the link between self-disclosure and FCR. For patients who tend to suppress their emotions, measures should be taken to encourage them to communicate with their spouses, family, and friends. This approach can help patients receive more care and support, bolster their confidence in disease treatment, and alleviate FCR.
Our study has several limitations that warrant acknowledgment. Firstly, the sample size of this study is insufficient, which may affect the generalizability of the findings. Additionally, our investigation solely examines the level of adult attachment and self-disclosure from the perspective of patients, neglecting the potential impact of the spouse’s attachment style on patients’ mental health. Moreover, our study lacks exploration into the relationship between the four types of adult attachment (secure, fearful, preoccupied, and dismissive) and FCR in patients. Future research endeavors will focus on addressing these limitations by expanding the sample size, considering the spouse’s attachment style, and investigating the relationship between different types of adult attachment and FCR in breast cancer patients.
This study has illuminated the relationship between marital attachment, self-disclosure among breast cancer patients, and the fear of cancer recurrence, enabling nurses to gain deeper insights into the crucial role of emotional support between breast cancer patients and their spouses. In clinical practice, nurses can enhance patient care by providing comprehensive health education, fostering a more accurate understanding of the disease, and implementing effective strategies to enhance patients’ levels of self-disclosure. Encouraging patients to seek psychological support from their spouses can strengthen marital relationships, alleviate fear and anxiety, and potentially enhance patients’ quality of life and confidence in treatment, thereby improving prognosis.
Acknowledgement: None.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: Conception and design: Huimin Zheng; Provision of study materials or patients: Miao Ye; Collection and assembly of data: Minghui Wang; Data analysis and interpretation: Miao Ye; Manuscript writing: All authors. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: All experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval: The study was approved by the Ethics committee of the Jiangsu Cancer Hospital (IRB number: 2023-009). All participants signed the informed consent in this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Asaoka M, Narui K, Suganuma N, Chishima T, Yamada A, Sugae S, et al. Clinical and pathological predictors of recurrence in breast cancer patients achieving pathological complete response to neoadjuvant chemotherapy. Eur J Surg Oncol. 2019;45(12):2289–94. [Google Scholar] [PubMed]
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. [Google Scholar] [PubMed]
3. International Agency for Research on Cancer. Latest global cancer data: cancer burden rises to 19.3 million new cases and 10.0 million cancer deaths in 2020. Available from: https://www.iarc.who.int/news-events/latest-global-cancer-data-cancer-burden-rises-to-19-3-million-new-cases-and-10-0-million-cancer-deaths-in-2020/. [Accessed 2020]. [Google Scholar]
4. Rossi L, Mazzara C, Pagani O. Diagnosis and treatment of breast cancer in young women. Curr Treat Options Oncol. 2019;20(12):86. [Google Scholar] [PubMed]
5. El Masri J, Phadke S. Breast Cancer epidemiology and contemporary breast cancer care: a review of the literature and clinical applications. Clin Obstet Gynecol. 2022;65(3):461–81. [Google Scholar] [PubMed]
6. Cho D, Chu Q, Lu Q. Associations among physical symptoms, fear of cancer recurrence, and emotional well-being among Chinese American breast cancer survivors: a path model. Support Care Cancer. 2018;26(6):1755–61. [Google Scholar] [PubMed]
7. Park S, Sato Y, Takita Y, Tamura N, Ninomiya A, Kosugi T, et al. Mindfulness-based cognitive therapy for psychological distress, fear of cancer recurrence, fatigue, spiritual well-being, and quality of life in patients with breast cancer-A randomized controlled trial. J Pain Symptom Manage. 2020;60(2):381–9. [Google Scholar] [PubMed]
8. Bilodeau K, Gouin MM, Fadhlaoui A, Porro B. Supporting the return to work of breast cancer survivors: perspectives from Canadian employer representatives. J Cancer Surviv. 2023; 1–9. doi:10.1007/s11764-023-01382-5. [Google Scholar] [CrossRef]
9. Dalton K, Waterman M, Wassersug R, Garland SN. Fear of cancer recurrence in males diagnosed with breast cancer. Support Care Cancer. 2021;29(11):6183–6. [Google Scholar] [PubMed]
10. Favez N, Antonini T, Delaloye JF, Notari SC. From breast cancer surgery to survivorship: insecure attachment tendencies predict negative psychological outcomes. Health Psychol Open. 2021;8(1). doi:10.1177/2055102920987463. [Google Scholar] [CrossRef]
11. Nicolaisen A, Hagedoorn M, Hansen DG, Flyger HL, Christensen R, Rottmann N, et al. The effect of an attachment-oriented couple intervention for breast cancer patients and partners in the early treatment phase: a randomised controlled trial. Psychooncology. 2018;27(3):922–8. [Google Scholar] [PubMed]
12. Ramos K, Langer SL, Todd M, Romano JM, Ghosh N, Keefe FJ, et al. Attachment style, partner communication, and physical well-being among couples coping with cancer. Pers Relatsh. 2020;27(3):526–49. [Google Scholar] [PubMed]
13. Brandão T, Schulz MS, Matos PM. Attachment and adaptation to breast cancer: the mediating role of avoidant emotion processes. Eur J Cancer Care. 2018;27(2):e12830. [Google Scholar]
14. Désfalvi J, Lakatos C, Csuka SI, Sallay V, Filep O, Dank M, et al. Attachment style, relationship and sexual satisfaction: comparing breast cancer patients and healthy women. Orv Hetil. 2020;161(13):510–8. [Google Scholar]
15. Ramos K, Leo K, Porter LS, Romano JM, Baucom BRW, Langer SL. Attachment in couples coping with cancer: associations with observed communication and long-term health. Int J Environ Res Public Health. 2023;20(7):5249. [Google Scholar] [PubMed]
16. Zhao H, Li X, Zhou C, Wu Y, Li W, Chen L. Psychological distress among Chinese patients with breast cancer undergoing chemotherapy: concordance between patient and family caregiver reports. J Adv Nurs. 2022;78(3):750–64. [Google Scholar] [PubMed]
17. Xu J, Wang X, Chen M, Shi Y, Hu Y. Dilemma: disclosure experience among young female breast cancer survivors in China. J Adolesc Young Adult Oncol. 2022;11(5):486–92. [Google Scholar]
18. Soriano EC, Otto AK, LoSavio ST, Perndorfer C, Siegel SD, Laurenceau JP. Fear of cancer recurrence and inhibited disclosure: testing the social-cognitive processing model in couples coping with breast cancer. Ann Behav Med. 2021;55(3):192–202. [Google Scholar] [PubMed]
19. Zhou Y, Che CC, Chong MC, Zhao H, Lu Y. Effects of marital self-disclosure on marital relationship and psychological outcome for cancer patients: a systematic review. Support Care Cancer. 2023;31(6):361. [Google Scholar] [PubMed]
20. Youssef Y, Mehnert-Theuerkauf A, Götze H, Friedrich M, Esser P. Rapid screener for the assessment of fear of progression in cancer survivors: the fear of progression-questionnaire rapid screener. Eur J Cancer Care. 2021;30(3):e13400. [Google Scholar]
21. do Rosário Ramos Nunes Bacalhau M, Pedras S, da Graça Pereira Alves M. Attachment style and body image as mediators between marital adjustment and sexual satisfaction in women with cervical cancer. Support Care Cancer. 2020;28(12):5813–9. [Google Scholar]
22. Chen XY, Lou FL. The relationships among insecure attachment, social support and psychological experiences in family caregivers of cancer inpatients. Eur J Oncol Nurs. 2020;44:101691. [Google Scholar]
23. Li L, Zhong HY, Xiao T, Xiao RH, Yang J, Li YL, et al. Association between self-disclosure and benefit finding of Chinese cancer patients caregivers: the mediation effect of coping styles. Support Care Cancer. 2023;31(12):684. [Google Scholar] [PubMed]
24. Tao L, Lv JY, Tan XL, Hu XX, Fu L, Li JY. Relationships between attachment style, emotional self-disclosure, and quality of life among young breast cancer survivors: a cross-sectional study. Semin Oncol Nurs. 2024;40(1):151526. [Google Scholar] [PubMed]
25. Schapira L, Zheng Y, Gelber SI, Poorvu P, Ruddy KJ, Tamimi RM, et al. Trajectories of fear of cancer recurrence in young breast cancer survivors. Cancer. 2022;128(2):335–43. [Google Scholar] [PubMed]
26. Oztas B, Ugurlu M, Kurt G. Fear of cancer recurrence and coping attitudes of breast cancer survivors. Eur J Cancer Care. 2022;31(6):e13742. [Google Scholar]
27. Guo HT, Wang SS, Zhang CF, Zhang HJ, Wei MX, Wu Y, et al. Investigation of factors influencing the fear of cancer recurrence in breast cancer patients using structural equation modeling: a cross-sectional study. Int J Clin Pract. 2022;2022:2794408. [Google Scholar] [PubMed]
28. Gormley M, Ghazal L, Fu MR, Van Cleave JH, Knobf T, Hammer M. An integrative review on factors contributing to fear of cancer recurrence among young adult breast cancer survivors. Cancer Nurs. 2022;45(1):E10–26. [Google Scholar] [PubMed]
29. Li Y, Fang C, Xiong MD, Hou H, Zhang YT, Zhang CH. Exploring fear of cancer recurrence and related factors among breast cancer patients: a cross-sectional study. J Adv Nurs. 2024;80(6):2403–14. [Google Scholar] [PubMed]
30. Pudkasam S, Polman R, Pitcher M, Fisher M, Chinlumprasert N, Stojanovska L, et al. Physical activity and breast cancer survivors: importance of adherence, motivational interviewing and psychological health. Maturitas. 2018;116:66–72. [Google Scholar] [PubMed]
31. Gall TL, Bilodeau C. God attachment: resource or complication in women’s and their partners’ adjustment to the threat of breast cancer. J Relig Health. 2021;60(6):4227–48. [Google Scholar] [PubMed]
32. Muldbücker P, Steinmann D, Christiansen H, de Zwaan M, Zimmermann T. Are women more afraid than men? Fear of recurrence in couples with cancer-predictors and sex-role-specific differences. J Psychosoc Oncol. 2021;39(1):89–104. doi:10.1080/07347332.2020.1762823. [Google Scholar] [PubMed] [CrossRef]
33. Karbowa-Płowens M. Attachment styles, coping with stress, and social support among cancer patients. Contemp Oncol. 2023;27(2):95–100. doi:10.5114/wo.2023.130015. [Google Scholar] [PubMed] [CrossRef]
Appendix A
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools