
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

A Study on the Effect of Fear of Negative Evaluation on Restrained Eating and Its Intervention among Female College Students
1 Department of Psychology, Guangxi Normal University, Guilin, 541006, China
2 Department of Psychology, Guangxi University of Science and Technology, Liuzhou, 545006, China
3 School of Teacher Education, Hechi University, Hechi, 546300, China
* Corresponding Authors: Weijian Fu. Email: ; Wenyi Liu. Email:
(This article belongs to the Special Issue: Mental Health Promotion and Psychosocial Support in Vulnerable Populations: Challenges, Strategies and Interventions)
International Journal of Mental Health Promotion 2025, 27(2), 137-159. https://doi.org/10.32604/ijmhp.2025.059866
Received 18 October 2024; Accepted 13 January 2025; Issue published 03 March 2025
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Restrained eating, often motivated by the desire to control weight, is prevalent among young female college students and is considered a risk factor for eating disorders. Negative evaluation fear, exacerbated by social pressure, peer comparison, and academic stress, has been identified as a potential contributor to restrained eating behavior. However, research exploring the relationship between negative evaluation fear and restrained eating, particularly in the context of self-esteem and physical appearance perfectionism, remains limited. This study aims to investigate these relationships and design an intervention program to reduce restrained eating behaviors in female college students. Methods: Study 1 involved 617 female college students, using the Physical Appearance Perfectionism Scale, Rosenberg Self-Esteem Scale, Fear of Negative Evaluation Scale, and Dutch Eating Behavior Questionnaire to measure key variables. We examined the relationships between physical appearance perfectionism, self-esteem, fear of negative evaluation, and restrained eating. In Study 2, a 4-week group psychological intervention based on Acceptance and Commitment Therapy (ACT) was implemented with 45 students, divided into experimental, control, and placebo groups. The intervention’s effectiveness was assessed in reducing restrained eating and negative evaluation fear. Results: The study found that fear of negative evaluation significantly predicted restrained eating and physical appearance perfectionism. Physical appearance perfectionism, in turn, positively predicted restrained eating and partially mediated the relationship between negative evaluation fear and restrained eating. Self-esteem moderated this mediation effect. Additionally, the ACT-based intervention significantly reduced fear of negative evaluation and restrained eating behavior in the experimental group. Conclusion: This study identifies fear of negative evaluation and physical appearance perfectionism as key predictors of restrained eating in female college students. Fear of negative evaluation significantly predicted restrained eating, with physical appearance perfectionism partially mediating this relationship. The ACT-based intervention effectively reduced both fear of negative evaluation and restrained eating. These findings highlight the importance of addressing negative evaluation fear and appearance perfectionism in interventions for restrained eating.Keywords
The 2020 Report on Nutrition and Chronic Diseases in China highlights the rising rates of overweight and obesity, particularly among young women. In 2020, the obesity rate for adult women reached 7.3%, with young women in urban areas exhibiting higher rates than men [1]. Among female college students, increasing concerns about body image have led to a rise in weight-control behaviors, including dieting. A cross-national study revealed that Chinese women, particularly college students, exhibit higher levels of restrained eating compared to men, driven by a greater focus on weight and body image [2]. These behaviors may contribute to eating disorders and associated mental health issues such as anxiety and depression. The prevalence of eating disorders and related psychological problems among female college students is a growing concern, highlighting the need for effective interventions to improve their mental well-being.
Many existing studies on college students have shown that mental health issues, such as anxiety, depression, and self-esteem, are dynamic and fluctuate over time [3]. Longitudinal data indicate that these issues are not static, and their development varies across different groups of students. These studies also reveal significant heterogeneity among different groups within the college student population, meaning that the psychological challenges faced by students may vary depending on factors such as year in school, academic pressure, and social context [4]. For instance, students in their first year of college may experience heightened anxiety and lower self-esteem, which may change as they adjust to academic and social environments [5]. This dynamic nature of mental health issues must be considered when examining their impact on behaviors such as restrained eating.
One key psychological factor contributing to restrained eating is Fear of Negative Evaluation (FNE), which refers to anxiety about being negatively judged by others, particularly regarding physical appearance [6]. Research has demonstrated a positive correlation between FNE and restrained eating, with socially anxious individuals often engaging in restrictive dieting to achieve what they consider an ideal body shape, believing this will enhance their social acceptance and status [7]. Additionally, individuals with low self-esteem and those exhibiting high levels of physical appearance perfectionism are more likely to experience heightened FNE, which can exacerbate restrained eating tendencies [8].
Perfectionism, particularly related to physical appearance, is another critical factor influencing eating disorders. Perfectionism involves the pursuit of unrealistic standards, coupled with a fear of negative evaluation [9]. Research indicates that physical appearance perfectionism is more closely associated with eating disorders than general perfectionism [10], with individuals high in physical appearance perfectionism being more likely to engage in restrictive eating behaviors. Moreover, self-esteem plays a crucial role in eating disorders, as individuals with low self-esteem often place excessive emphasis on their appearance and weight [9]. Studies have found that those who engage in restrained eating behaviors tend to have lower episodic self-esteem, in contrast to non-restrictive dieters, whose self-esteem tends to remain more stable [11].
Building on this theoretical framework, the present study explores the factors influencing restrained eating behaviors among female college students, specifically focusing on FNE, self-esteem, and physical appearance perfectionism. The aim is to examine the internal mechanisms linking these psychological factors to restrained eating and propose a group intervention based on Acceptance and Commitment Therapy (ACT) to address these issues.
ACT is an evidence-based psychological intervention that enhances psychological flexibility by helping individuals accept negative emotions, commit to value-driven actions, and reduce maladaptive behaviors [12]. Unlike other therapeutic approaches, ACT does not solely focus on symptom reduction, but instead promotes behavior change through values alignment. This makes ACT particularly effective in addressing complex, multifaceted issues like restrained eating, FNE, and low self-esteem. ACT has been shown to be effective in treating eating disorders by reducing emotional avoidance and fostering a healthier relationship with one’s body and self-image [13]. Given its focus on improving psychological flexibility and addressing the underlying cognitive and emotional factors contributing to restrained eating, ACT is a well-suited intervention for female college students.
This study aims to implement an ACT-based intervention to improve psychological flexibility, reduce Fear of Negative Evaluation, and enhance self-esteem among female college students. By doing so, we hope to alleviate restrained eating behaviors and provide a foundation for future research on effective interventions for eating disorders in this population.
2 Theoretical Background and Research Hypothesis
2.1 Fear of Negative Evaluation and Restrained Eating
FNE is defined as the fear of being evaluated by others, distress over negative evaluations, and the anticipation that others may give negative judgments about oneself [14]. In clinical samples of women diagnosed with eating disorders, it has been found that their levels of FNE are significantly higher than those of non-eating disordered control populations [15]. Cross-sectional studies have also shown that FNE, along with a tendency to be thin, is a strong predictor of bulimic symptoms [16]. In a longitudinal study, researchers found that FNE was a determinant of subsequent symptoms of body dissatisfaction and eating disorders [17]. Restrained eating refers to limiting one’s food intake in order to control or reduce weight [18]. However, individuals who engage in restrained eating often progress to overeating, becoming what is termed “failed restrictive eaters” [19]. Overeating and bulimic symptoms are part of the symptom profile in individuals with bulimia nervosa while dieting behaviors are also observed in those with anorexia nervosa. In these cases, failed restrictive eaters may turn to binge eating as a way to cope with negative emotions. Some studies have found a correlation between restrained eating and binge frequency, with the likelihood of bingeing behavior significantly increasing after a day of restrictive dieting [20,21]. FNE has been identified in multiple studies as one of the key predictors of eating disorders [22]. Recent studies specifically targeting the college student population have used longitudinal data to track the development of eating behaviors and associated psychological factors over time. These studies have highlighted the dynamic nature of mental health issues, such as anxiety, depression, and self-esteem, within the college student population. Longitudinal research shows that these psychological factors fluctuate as students navigate their academic careers and social environments. For example, students entering college may experience heightened anxiety and lower self-esteem, while these factors may evolve as students’ progress in their academic journey and adjust to their environment [23]. Longitudinal studies also emphasize the heterogeneity of these experiences among different groups within the student population, indicating that some students may be more susceptible to eating disorders based on varying levels of social pressure, academic stress, and personal characteristics [24]. In this context, FNE is particularly relevant, as it often manifests more strongly in individuals who are socially anxious or who place excessive value on external validation, such as body image. Understanding the dynamic and heterogeneous nature of FNE and its relationship to restrained eating behaviors is crucial for developing effective interventions for college students.
2.2 The Mediating Effect of Physical Appearance Perfectionism
Research has shown that perfectionism has two dimensions. One is adaptive perfectionism, which is associated with health, and the other is maladaptive perfectionism, which is associated with anxiety, negativity, and depression. One study found a strong correlation between maladaptive perfectionism and FNE [25]. Maladaptive perfectionists have a rigid concept of success and failure, often viewing failure as unacceptable, which negates their self-worth [26]. If their goals are unattainable, they see this as a negative reflection on their self-worth [10], and as a result, they fear negative evaluation and worry that others will judge them negatively [27]. Perfectionists with higher sensitivity to negative evaluation are less adaptable and often fail to accurately interpret these evaluations, instead perceiving them as a lack of acceptance by others [28]. Studies have shown that FNE is an effective predictor of maladaptive perfectionism, with maladaptive perfectionism and FNE being positively correlated [29]. Physical appearance perfectionism refers to setting and strictly adhering to unrealistic standards of physical appearance and judging one’s self-worth based on whether these standards are met. Physical appearance perfectionism is considered a specific domain of maladaptive perfectionism [12]. Among female college students, negative body self-concept can affect social appearance anxiety through the mediation of FNE and physical appearance perfectionism [30]. Additionally, research has found that the fear of appearance imperfection within physical appearance perfectionism is significantly positively correlated with FNE, and can affect social appearance anxiety through the mediation of other variables related to FNE [31]. In the context of college students, particularly among female students, the relationship between physical appearance perfectionism and psychological health issues such as anxiety and depression is of growing concern. FNE and physical appearance perfectionism play key roles in social appearance anxiety, making college students, especially women, particularly vulnerable to appearance-related pressures [23].
A significant body of research has explored the relationship between maladaptive perfectionism and eating behavior problems. Maladaptive perfectionists are at a higher risk for developing eating disorders [32]. When performance fails to meet excessively high standards, perfectionism is often accompanied by overly critical self-appraisal, and this maladaptive cycle can become pathological. Perfectionism is considered maladaptive when individuals evaluate themselves based solely on the pursuit of unrealistically high standards in a specific domain [33]. In the context of eating disorders, perfectionism is often linked to physical appearance, with individuals with bulimia nervosa displaying higher levels of physical appearance perfectionism [34]. Women who perceive themselves as having an imperfect body shape are more likely to experience symptoms such as binge eating [35], which is commonly seen in individuals who fail in their efforts to restrict their eating.
2.3 The Moderating Effect of Self-Esteem
FNE can influence restrained eating behaviors through physical appearance perfectionism, with self-esteem playing a moderating role in this process. Some researchers suggest that self-esteem refers to an individual’s perception of their own worth and that it significantly affects various psychological factors [36]. Individuals evaluate their self-worth based on internal and external cues, and self-esteem can influence a range of psychological outcomes. For college students, low self-esteem is often linked to heightened pressure regarding their social interactions and appearance, as they tend to be more sensitive to the evaluations of others, especially in terms of physical appearance and social acceptance. As a result, students with lower self-esteem may experience anxiety and fear when confronted with negative evaluations of themselves [37]. Self-esteem has a negative correlation with FNE, meaning that individuals with high self-esteem tend to experience less fear of negative judgment. High self-esteem is associated with a positive mindset, which can buffer the impact of negative evaluations [38]. In contrast, individuals with low self-esteem are more vulnerable to FNE, experiencing greater distress and concern when faced with negative evaluations from others. These individuals are particularly sensitive to how others perceive them, especially in social and appearance-related contexts, and may be more likely to engage in behaviors such as restrained eating to cope with these fears [39]. For college students, these dynamics are especially relevant. College years are marked by significant social pressures, and students with low self-esteem may be more susceptible to these pressures, resulting in maladaptive coping mechanisms, including unhealthy eating behaviors [40].
The history of psychology has seen significant research on perfectionism and self-esteem, with perfectionism recognized as an important personality trait in the development and maintenance of various psychological disorders. Maladaptive perfectionists tend to have lower levels of self-esteem. For instance, one study found that self-esteem mediates the relationship between perfectionism and obsessive-compulsive symptoms, revealing that individuals with obsessive-compulsive disorder (OCD) exhibit higher levels of perfectionism and lower self-esteem compared to control participants [41]. Individuals with OCD often associate imperfect performance with failure, which further contributes to their lowered self-esteem. Furthermore, research has shown that individuals with lower self-esteem are more likely to experience depressive symptoms and display higher levels of perfectionism [42]. In contrast, well-adjusted perfectionists generally have higher levels of self-esteem, and elevated self-esteem can mitigate the embarrassment associated with maladaptive perfectionism [43]. Appearance perfectionists, a subtype of maladaptive perfectionists, tend to have lower self-esteem [44].
Numerous studies have demonstrated a strong link between self-esteem and eating behavior problems. In adolescent populations, low self-esteem has been identified as a key risk factor for the development of eating disorders. Adolescents with lower self-esteem are at greater risk for problematic eating behaviors, particularly in female adolescents [45,46]. Individuals with bulimia nervosa are particularly sensitive to negative evaluations linked to low self-esteem, and they tend to have lower self-perceptions and poorer self-ratings [47]. Low self-esteem and body dissatisfaction strongly influence restrained eating behaviors. This relationship is exacerbated in cultures influenced by Eastern Confucian values, which intensify body dissatisfaction and contribute to low self-esteem related to body size and appearance, particularly among females [48].
In summary, this study suggests that self-esteem, as a variable influencing many psychological factors, likely moderates the relationship between FNE and physical appearance perfectionism, as well as the impact of physical appearance perfectionism on restrained eating behaviors among female college students.
Deboer et al., in a study involving 82 female college students participating in an eating disorder prevention program [16], found that directly addressing the internalization of the desire to be thin led to a reduction in FNE related to body size and weight among female college students. Furthermore, reductions in restrained eating behaviors contributed to further decreases in FNE, suggesting that this process may play an important role in mitigating and preventing eating disorder behaviors. Other researchers have used cognitive-behavioral interventions, combining cognitive restructuring with exposure therapy, to develop programs aimed at reducing FNE in the context of social anxiety, with some promising results [49,50]. In another study, cognitive-behavioral therapy (CBT) was applied to 175 patients with social anxiety disorder, leading to a reduction in both FNE and social anxiety symptoms [51]. However, some studies using positive movie extinction training to intervene in FNE have found reductions in negative stimuli but no significant decrease in FNE regression [52].
There are a variety of potential methods for intervening with the negative emotions triggered by FNE, such as anxiety and fear. For instance, research on autistic children has shown that music therapy can significantly reduce negative emotions, foster positive emotional experiences, and decrease overall emotional distress [53]. Additionally, positive thinking meditation has been shown to be effective in reducing negative emotions, leading to a more emotionally peaceful state. Follow-up studies revealed that the effects of positive thinking meditation lasted over time, with one study showing that eight weeks of positive thinking group counseling reduced depression levels among college students [54].
In summary, while numerous studies have explored the relationship between various psychological variables and FNE, providing valuable theoretical insights, intervention studies specifically targeting FNE remain relatively scarce. Therefore, it is essential to expand research in this area, building upon existing studies to identify effective intervention methods and broaden the scope of this field. In this context, acceptance and commitment therapy (ACT), a representative method of third-generation cognitive-behavioral therapy, is considered in this study as an intervention for female college students to reduce FNE and the occurrence of restrained eating behaviors.
In summary, we propose the following four hypotheses:
H1: Fear of negative evaluation among female college students positively predicts restrained eating.
H2: Physical appearance perfectionism mediates the relationship between fear of negative evaluation and restrained eating.
H3: Self-esteem moderates the mediation model between fear of negative evaluation, physical appearance perfectionism, and restrained eating behavior among female college students, with self-esteem moderating both the early and later segments of the mediation pathway. The specific hypothetical model is depicted in Fig. 1.
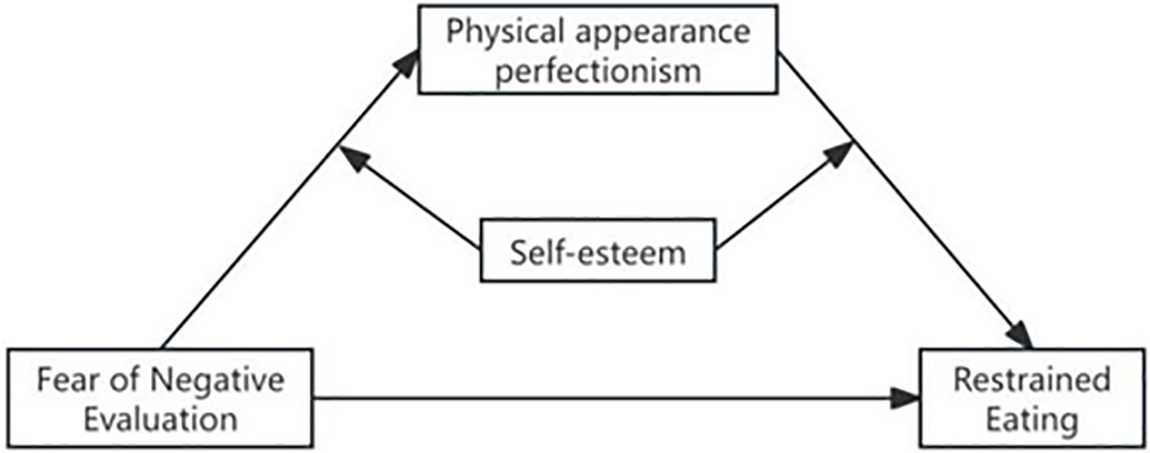
Figure 1: Theoretical model diagram
H4: Group psychological intervention based on Acceptance and Commitment Therapy (ACT) can reduce the level of fear of negative evaluation among female college students, thereby decreasing the occurrence of restrained eating.
To test these hypotheses, we conducted two studies:
In Study 1, We distributed questionnaires and collected data to examine the current state of fear of negative evaluation, physical appearance perfectionism, self-esteem, and restrained eating among female college students. The data were analyzed to explore the interrelationships between these variables. Based on the findings, we aim to establish a theoretical model in which physical appearance perfectionism acts as a mediating variable.
In Study 2, We implemented ACT through the development of a group intervention program for female college students experiencing negative emotional issues due to high levels of fear of negative evaluation. The goal was to improve their psychological flexibility, help them accept themselves, live in the present, and regulate their emotions rationally. This, in turn, was expected to reduce both the level of fear of negative evaluation and the occurrence of restrained eating.
Study 1
Study 1 aims to elucidate the interrelationships among fear of negative evaluation, physical appearance perfectionism, self-esteem, and restrained eating. We employed a questionnaire-based measurement to assess these variables among female college students and constructed a theoretical model, providing a foundation for the intervention method in Study 2.
Participant
In this study, questionnaires were distributed to female college students at various colleges and universities using both online and offline methods. The online method involved inviting participants to complete the questionnaire via social media platforms, while the offline method involved distributing paper versions of the questionnaire directly to female college students on campus. All procedures involving human participants were conducted in accordance with the ethical standards outlined in the 1964 Declaration of Helsinki, and the study received approval from the Ethics Committee of Hechi University, with the approval number H24016. A total of 700 questionnaires were distributed. All participants signed the informed consent in this study. The process for excluding invalid responses involved several steps: first, questionnaires that were incomplete or had missing data for key questions were excluded. Second, responses that exhibited patterns of random or inconsistent answers, such as multiple identical answers to contradictory questions, were also deemed invalid and removed. Additionally, questionnaires where the participants failed to meet the inclusion criteria, such as age or student status, were excluded. After applying these criteria, 617 valid questionnaires were retained, yielding a response rate of 88.14%. The sample consisted of 202 freshmen, 206 sophomores, 70 juniors, 65 seniors, and 74 postgraduates. Among the participants, 161 were only-children, while 456 were non-only-children. Additionally, 346 participants had families located in rural areas, and 271 participants had families located in urban or suburban areas. Body Mass Index (BMI) categories play a crucial role in understanding restrained eating behaviors. Underweight individuals may engage in restrictive eating to prevent further weight loss, often due to heightened body image concerns; Normal weight individuals may restrict their diet due to fear of negative evaluation; Overweight individuals are often motivated by body dissatisfaction and societal expectations, leading to increased restrictive eating; Obese individuals may struggle with more intense fear of negative evaluation, exacerbating eating control behaviors [55]. Controlling for BMI in studies on fear of negative evaluation and restrained eating is essential, as BMI influences body image perceptions and eating behaviors, potentially confounding the relationship between fear of negative evaluation and restrained eating [56]. According to the standard of Chinese BMI index of “Guidelines for the Prevention and Control of Overweight and Obesity in Adults in China” [57], the BMI index showed that there were underweight participants 164, normal 409, overweight 33, and obese 11; the average age of the sample was 19.1 years (SD = 1.75).
4.1 Fear of Negative Evaluation Scale
The Brief FNE Scale was used with 12 questions [58]. The Chinese revised edition has also been extensively validated within China [59]. Higher scores indicate higher levels of negative evaluation of the outside world. The scale contains 8 positively scored questions and 4 directionally scored questions using a 5-point Likert scale, with higher total scores indicating higher levels of negative appraisal fear in individuals. Because some researchers have found that the four reverse-scored questions of the Brief FNE Scale confound the tested sample, it is suggested that administering the scale using the eight positive-scored questions would have higher reliability [59]. Therefore, the eight positive-scored questions of the scale were used to measure the level of FNE among female college students in the present study. The internal consistency coefficient of this scale in this study was 0.903 and the synthetic reliability was 0.922.
4.2 Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (SES) was developed by Rosenberg in 1965 [35]. The Chinese revised version of the scale was revised by Shen and Cai in 2008 [60]. The scale has been widely used as a measure of self-esteem and contains 10 items, five reverse scored and five positive scored, all rated on a 4-point Likert scale, with higher total scores indicating higher levels of self-esteem. The internal consistency coefficient of the scale in this study was 0.891.
4.3 Physical Appearance Perfectionism Scale
The Chinese version of the Physical Appearance Perfectionism Scale was developed by Chinese scholars Yang and Stoeber in 2012, based on the previously established Specific Perfectionism Scale [61]. The scale contains 12 items, which are divided into two subscales: worrying about an imperfect appearance (7 items) and wishing for a perfect appearance (5 items), and is scored on a 5-point Likert scale, with a higher total score indicating higher levels of perfectionism in the appearance of an individual. The internal consistency coefficient of the scale was 0.83, and the reliability of the two subscales was 0.85 and 0.80, respectively. In the present study, the internal consistency coefficient of the scale was 0.879, the synthetic reliability was 0.900, and the reliability coefficients of the subscales were 0.815 and 0.871.
The Restrained Eating Scale of the Dutch Eating Behavior Questionnaire developed by van Strien et al. was used [62]. The Chinese revised version of the scale was conducted by Li et al. in 2018, and it has demonstrated good reliability among Chinese participants [63]. The scale consists of 10 question items and is scored on a 5-point Likert scale, with higher total scores indicating a higher level of restrained eating in an individual, and those with a mean score of ≥3 on the restrained eating are considered to be restrictive, while those with a mean score of <3 on the restrained eating are considered to be nonrestrictive. The internal consistency coefficient of this scale in this study was 0.910 and the synthetic reliability was 0.927.
4.5 Procedure and Statistical Analysis
The online data collection for this study was done through an online platform that distributed questionnaires to female undergraduates in universities across the country, while offline, graduate students went into classes to distribute questionnaires to female undergraduates, which lasted for about 8–10 min, all of which were accompanied by a guide. In this study, Epidata version 3.1 software was used for data entry of the paper version of the questionnaire, and SPSS 26.0 software as well as related plug-ins were used for data organization, descriptive statistical analysis, ANOVA, correlation analysis, regression analysis, and common method bias test.
5.1 Data Normality Tests and Common Method Bias Tests
Due to the effect of bias such as data collection, which may cause the data to show a non-normal distribution, the data need to be tested for normality. The results are shown in Table 1.
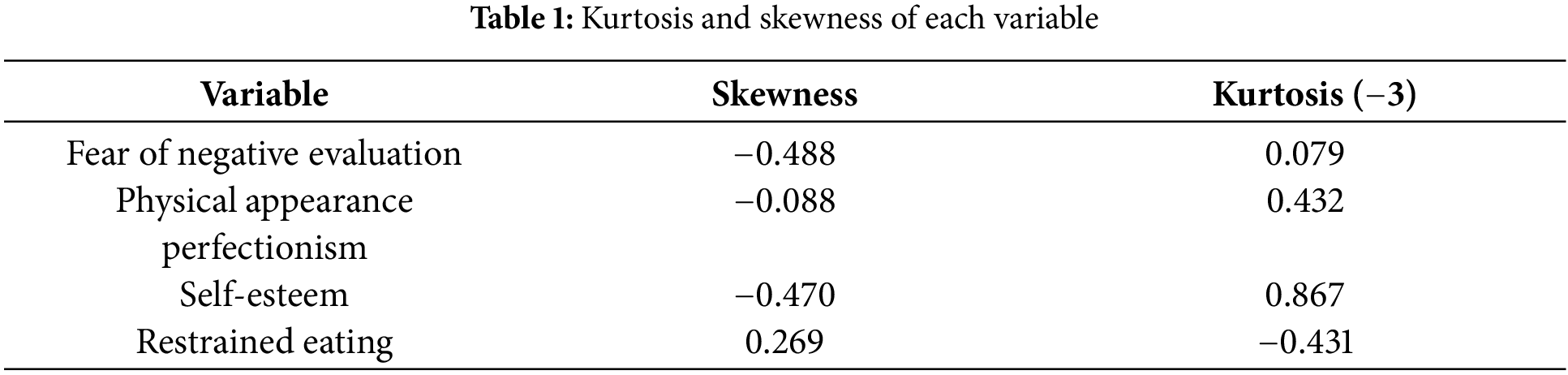
According to Kim’s perspective [64], we adopt the criterion that the absolute value of skewness is less than 2 and the absolute value of kurtosis minus 3 is less than 7 to represent the normality of the data. The reason for subtracting 3 from the kurtosis before taking the absolute value is that the theoretical kurtosis value of a normal distribution is 3, which indicates the distribution shape of the normal distribution. The purpose of subtracting 3 is to eliminate the baseline kurtosis of 3 for the normal distribution, allowing us to focus on the differences between the data distribution and the normal distribution. From the above table, it can be seen that all the variables satisfy the above conditions, so it can be considered that the data are approximately normally distributed in this study.
The test for common method bias in this study was conducted using the one-way test proposed by Harman, and the results showed that there were six factor eigenroots greater than 1, and the first of these explained 28.41% of the total variance, which is less than the critical value of 40%, so we can assume that there is no significant common method bias in this study.
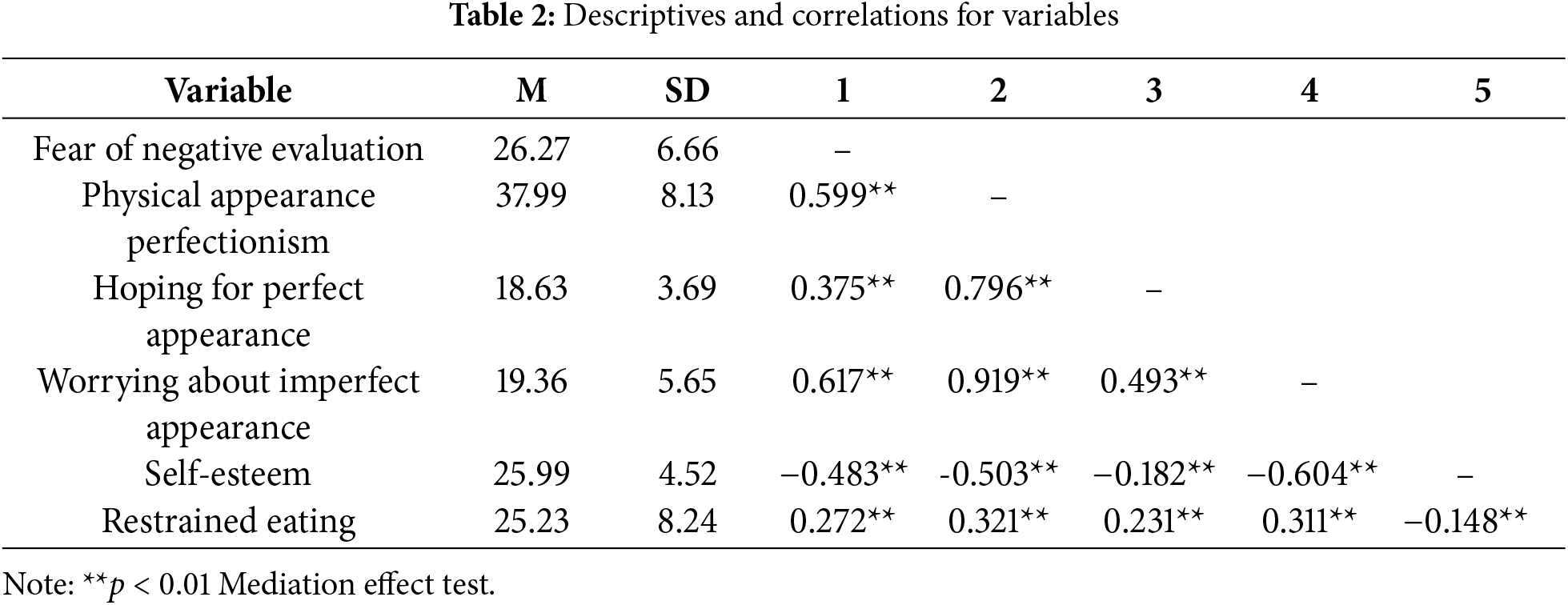
Descriptive statistics and correlation tests for each variable in this study are shown in Table 2.
Multiple regression analyses were performed using the model4 model in the SPSS macro program developed by Hayes et al. [65]. Tests of confidence interval estimates were performed using the Bootstrap method with 5000 replicate samples to calculate their 95% confidence intervals (95% CI). The mediating effect of appearance perfectionism was tested after controlling for age and BMI. The results are shown in Table 3.
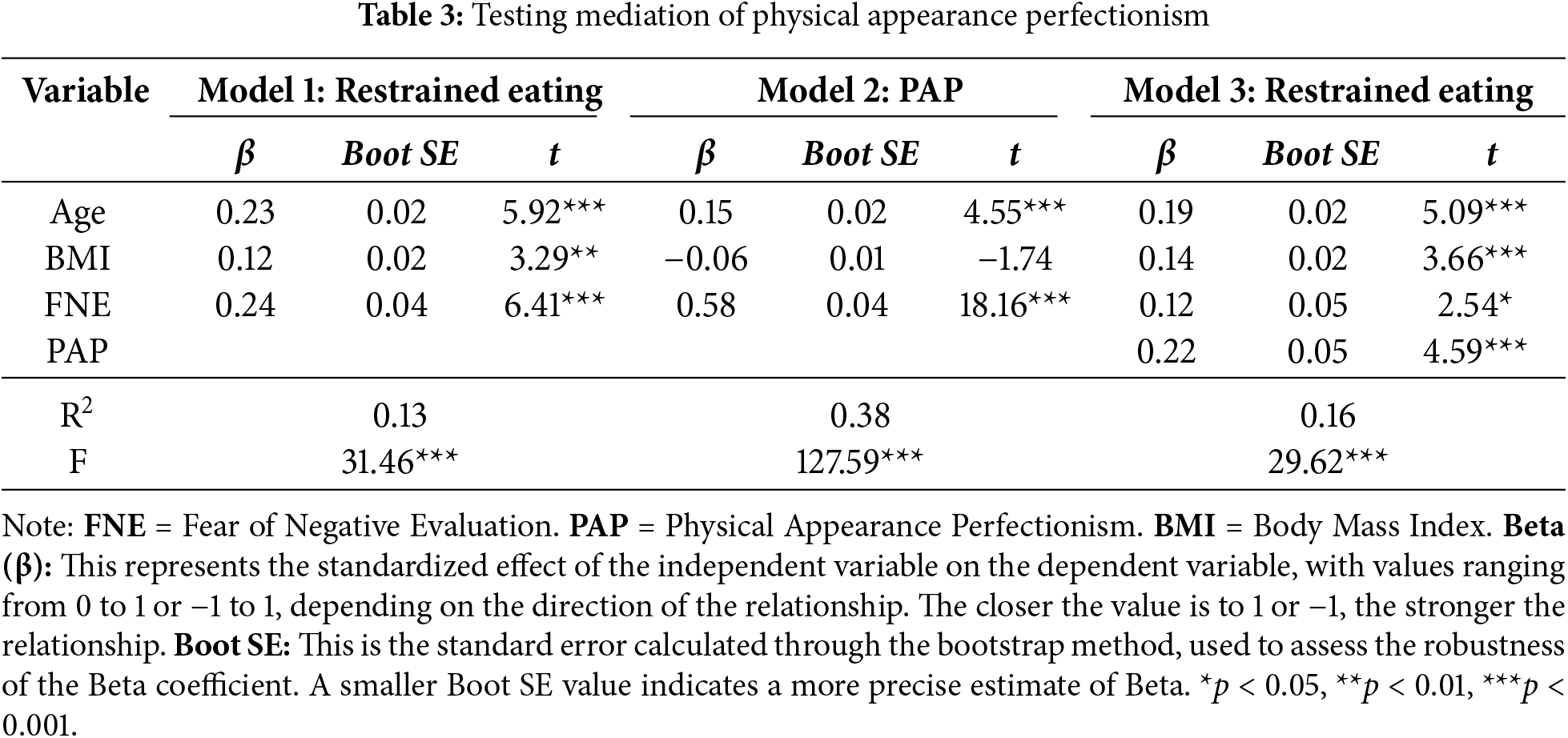
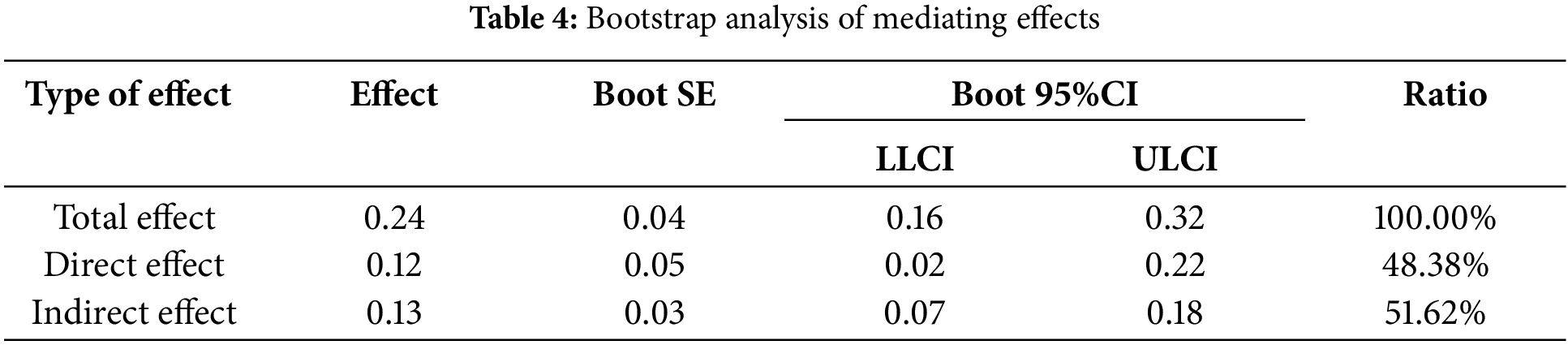
In Model 1, FNE positively predicted restrained eating (β = 0.24, t = 6.41, p < 0.001); in Model 2, FNE positively predicted physical appearance perfectionism (β = 0.58, t = 18.16, p < 0.001); and in Model 3, both physical appearance perfectionism (β = 0.22, t = 4.59, p < 0.001) and FNE (β = 0.12, t = 2.54, p < 0.05) both positively predicted restrained eating; the results were examined using the Bootstrap test and are shown in Table 4, indicating that the 95% CIs for the direct and indirect effects of FNE on restrained eating were not inclusive of 0, while the direct and indirect effects of this outcome accounted for the total effects of 48.38% and 51.62%. In summary, we found that physical appearance perfectionism exerted a partial mediating effect between FNE and restrained eating.
5.2 Analysis of the Moderating Effects of Self-Esteem
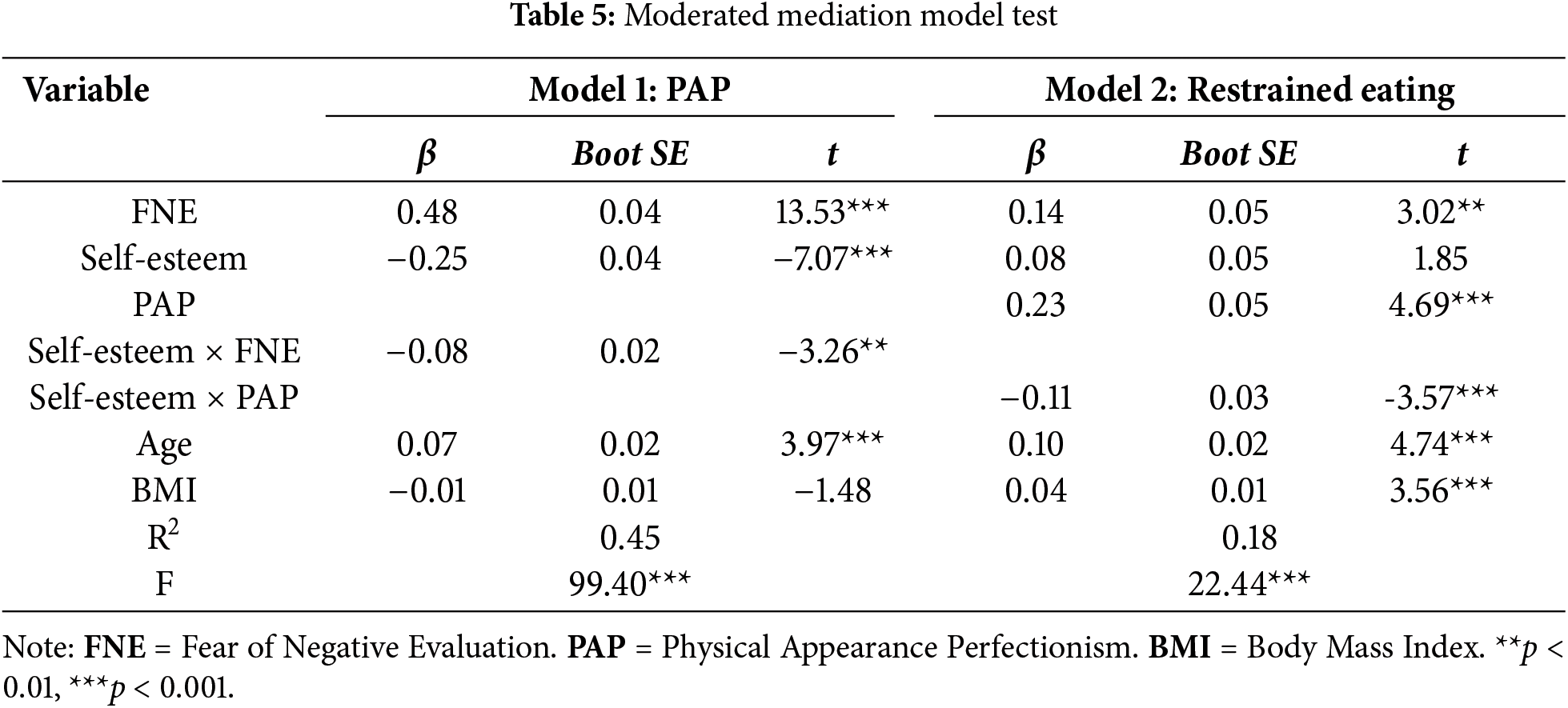
The present study continued to process the data using Model58 model, an SPSS macro program developed by Hayes et al. [65]. As mentioned above, to conduct a moderated mediation model test controlling for the variables of age and BMI as the independent variable of negative appraisal of fear, restrictive diet as the dependent variable, appearance perfectionism as the mediator variable, and self-esteem as the moderating variable, and the results are shown in Table 5. Results indicated that after placing self-esteem level as a moderating variable in the model FNE significantly positively predicted physical appearance perfectionism (β = 0.48, t = 13.53, p < 0.001), and physical appearance perfectionism significantly positively predicted restrained eating (β = 0.14, t = 3.02, p < 0.001). The interaction terms of self-esteem and FNE significantly negatively predicted physical appearance perfectionism (β = −0.08, t = −3.26, p < 0.01), and self-esteem and physical appearance perfectionism significantly negatively predicted restrained eating (β = −0.11, t = −3.57, p < 0.001). The results indicated that self-esteem significantly moderated the relationship between FNE and physical appearance perfectionism, as well as the effect of physical appearance perfectionism on restrained eating. This suggests that self-esteem plays a key role in influencing both the development of perfectionist tendencies related to appearance and the tendency to engage in restrained eating.
In order to further investigate the substance of the interaction terms between self-esteem and FNE and self-esteem and physical appearance perfectionism as well as the trend of the moderating effect of self-esteem, the mean of self-esteem was added and subtracted by one standard deviation, and divided into groups with high self-esteem level and low self-esteem level for simple slope analysis. The moderating role of self-esteem between FNE and physical appearance perfectionism was first analyzed. FNE significantly positively predicted physical appearance perfectionism for female college students with low self-esteem levels (β = 0.58, t = 12.28, p < 0.001), and FNE had a diminished positive predictive effect on physical appearance perfectionism for female college students with high self-esteem levels (β = 0.40, t = 10.44, p < 0.001). This indicates that the predictive effect of FNE on physical appearance perfectionism is on a decreasing trend as self-esteem levels increase. As shown in Fig. 2.
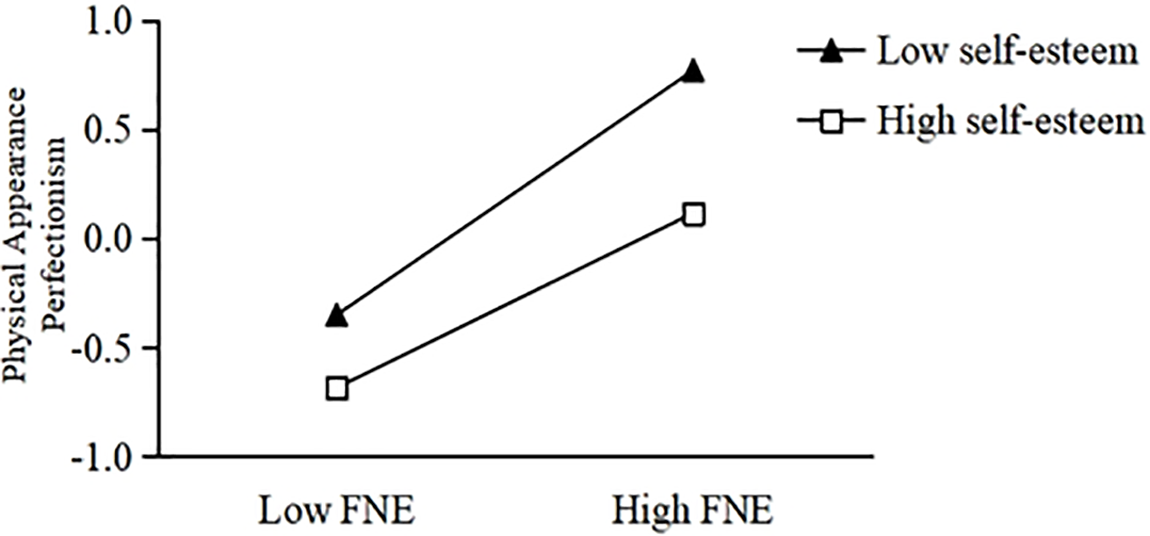
Figure 2: Self-esteem’s moderating effect between FNE and appearance perfectionism. Note: FNE = Fear of Negative Evaluation
The moderating role of self-esteem between physical appearance perfectionism and restrained eating was analyzed next. Using simple slope analysis, we can find that physical appearance perfectionism significantly positively predicts restrained eating for female college students at low self-esteem levels (β = 0.38, t = 6.66, p < 0.001), and Restrained Eating is a weaker predictor of predicting restrained eating for female college students at high self-esteem levels (β = 0.14, t = 2.31, p < 0.001). This indicates that the predictive effect of physical appearance perfectionism on predicting restrained eating tends to decrease as the level of self-esteem increases. That is, as the level of self-esteem increases, physical appearance perfectionism decreases as a predisposition to restrained eating behaviors among female college students. As shown in Fig. 3.
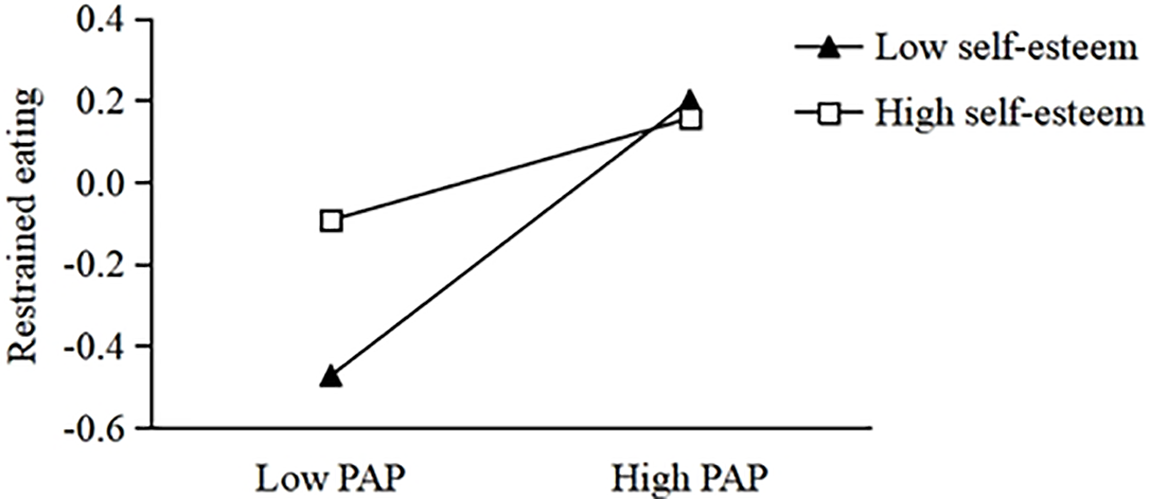
Figure 3: Self-esteem’s moderating effect between PAP and restrained eating. Note: PAP = Physical Appearance Perfectionism
Study 2
Study 2 was conducted on the basis of Study 1, which have demonstrated that FNE can not only have an effect on restrained eating through physical appearance perfectionism, but also have a direct effect on restrained eating. Therefore, Study 2 designed an intervention program based on Acceptance Commitment Therapy (ACT) to intervene in female college students’ FNE, exploring whether it can effectively reduce female college students’ negative emotions and self-pleasing, and then reduce the occurrence of restrained eating by improving their psychological flexibility and reducing the level of FNE.
Participant
This study employed the Brief FNE Scale and the Dutch Eating Behavior Questionnaire to select subjects for intervention. According to prior research, participants with an FNE mean score of ≥3 points are classified as having high levels of FNE [58]. If the mean score for restrictive eating behavior is ≥3 points, they are identified as restrictive eaters; if the mean score is <3 points, they are identified as non-restrictive eaters. Based on these criteria, a total of 143 individuals with high levels of FNE and restrictive eating behavior were selected. Among these, 45 individuals who expressed a willingness to participate in the study and committed to ongoing participation were chosen as the final subjects. These subjects were randomly assigned to the experimental group, control group, and placebo group, with 15 participants in each group. Upon completion of the study, participants will receive a small gift as a token of appreciation.
6.1 Group Psychological Intervention Program Based on ACT
It has already been mentioned that in some studies, cognitive behavioral therapy has been used to intervene in the FNE to improve the emotional state of participants with social anxiety disorder, and some results have been achieved [51]. Acceptance and commitment therapy, as one of the third-generation cognitive behavioral therapy theories, is based on the development of positive thinking techniques, which are widely used in various fields [66], and it has been a great supplement to the insufficiency of cognitive behavioral therapy, with its core techniques and there are six main aspects of the treatment mechanism: 1. Focus on the present moment; 2. Acceptance; 3. Cognitive dissociation; 4. Using oneself as a mirror; 5. Clarifying values; and 6. Commitment to action. Acceptance and Commitment Therapy has been introduced to China and is now widely applied within the country [67]. An overarching goal of ACT is to increase the visitor’s psychological flexibility, which is a mediator of changes in self-compassion, anxiety, depression, stress, and general psychological distress [68]. Acting on one’s values and accepting one’s self. Researchers have found that psychological rigidity and negative appraisal fear are highly correlated, and that ACT can increase psychological flexibility, so it can be assumed that ACT can reduce the level of FNE by increasing an individual’s psychological flexibility and increasing the level of psychological resilience [60]. Combining the above studies with the therapeutic mechanism of ACT, the present study suggests that ACT can be used to reduce the level of FNE through guiding and encouraging the participants to accept the negative emotions triggered by FNE, and at the same time promoting participants to increase their attention to themselves, change their cognition, follow their values to change their perception and understanding of the present moment, reduce experiential avoidance, and finally change their behavior and psychology by committing to action. Therefore, based on the theory and intervention techniques of ACT, a group counseling intervention program was developed. It runs for a total of eight days, with each day having a different theme (e.g., “It was nice to meet you” on day 1 and “Commitment to action” on day 8). The exact steps and details of the experiment we have posted in: https://www.protocols.io/private/7A7EC8C40D4E11EFA8660A58A9FEAC02, accessed on 12 January 2025.
6.2 Fear of Negative Evaluation Scale
Consistent with Study 1.
Consistent with Study 1.
The study was set up with three study phases: pre-test, post-test, and tracking measurement (One month after the intervention). The participants needed to be given basic training and popularization of the intervention knowledge before conducting the intervention, including the concepts and basic theoretical knowledge of ACT, FNE, and restrained eating. Both the experimental and placebo groups were scheduled to have group counseling interventions twice a week for 2 h each, for a total of 8 interventions lasting about 4 weeks before and after the trial, and participants were tracking measured one month after the trial. The participants were required to fill out the group counseling protocol before the group counseling started, and the group counseling evaluation questionnaire after the whole group counseling intervention in order to facilitate the main test to grasp the situation of the whole activity carried out and the participant’s evaluation of this activity. The experimental group used the ACT intervention protocol for the group counseling intervention; the control group did not do any treatment, but had to report the weekly diet and emotional status; the placebo group was treated with music appreciation, and all the participants had no previous experience in participating in group counseling, had no organic disease, and had normal mental status. All data were standardized and statistical methods such as descriptive statistics and comparison of differences were used.
7.1 Pre-intervention Homogeneity Tests for Experimental, Control, and Placebo Groups
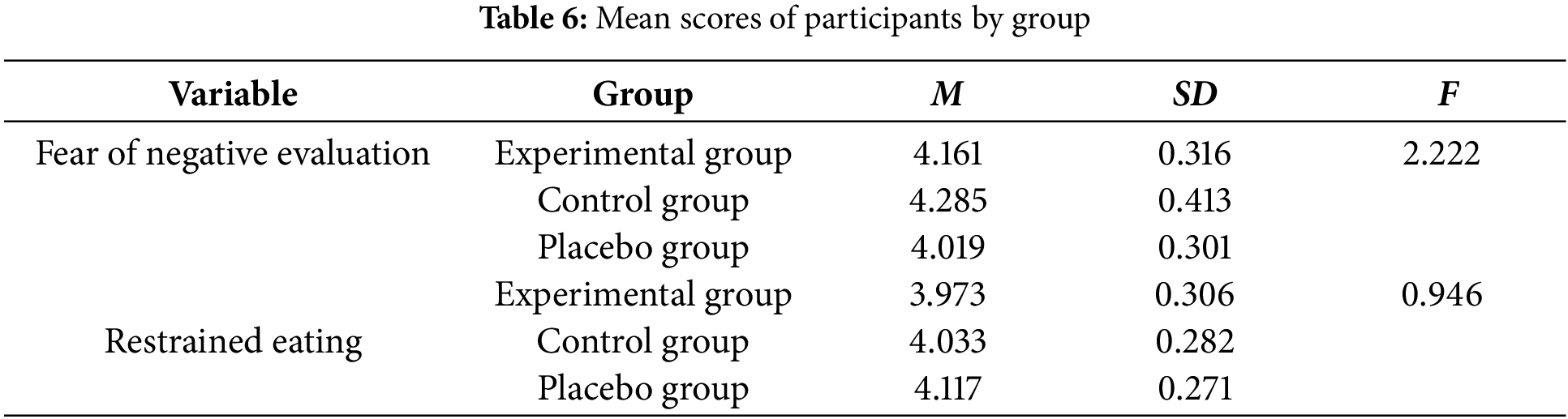
The test of difference was conducted to determine the homogeneity of the three groups of participants in the experimental, control and placebo groups, and the results of the data analysis showed that there was no significant difference between the mean scores of the three groups of participants on FNE (F = 2.222, p > 0.05) and restrained eating (F = 0.946, p > 0.05), and therefore we can regard the three groups of participants as being homogeneous and relatively well-balanced. The specific results are shown in Table 6.
7.2 Analysis of Variance for Participants Measured at Post-Intervention as well as at Follow-Up
Further analysis of the differences between the mean scores of FNE and restrained eating in the experimental, control and placebo groups at the three time points was performed by using the three measurement times, pre-test, post-test and tracking measurement as within-subjects variable (Test time), and the three groups, experimental, control and placebo, as between-subjects variable (Group), and by using the mean score of FNE as the dependent variable in a 3 × 3 repeated measures ANOVA with the Mauchly’s spherical hypothesis test, the covariance matrices of the dependent variables were equal (p > 0.05), and the interaction term “test time × group” was consistent with the spherical hypothesis analysis. The results are shown in Table 7.
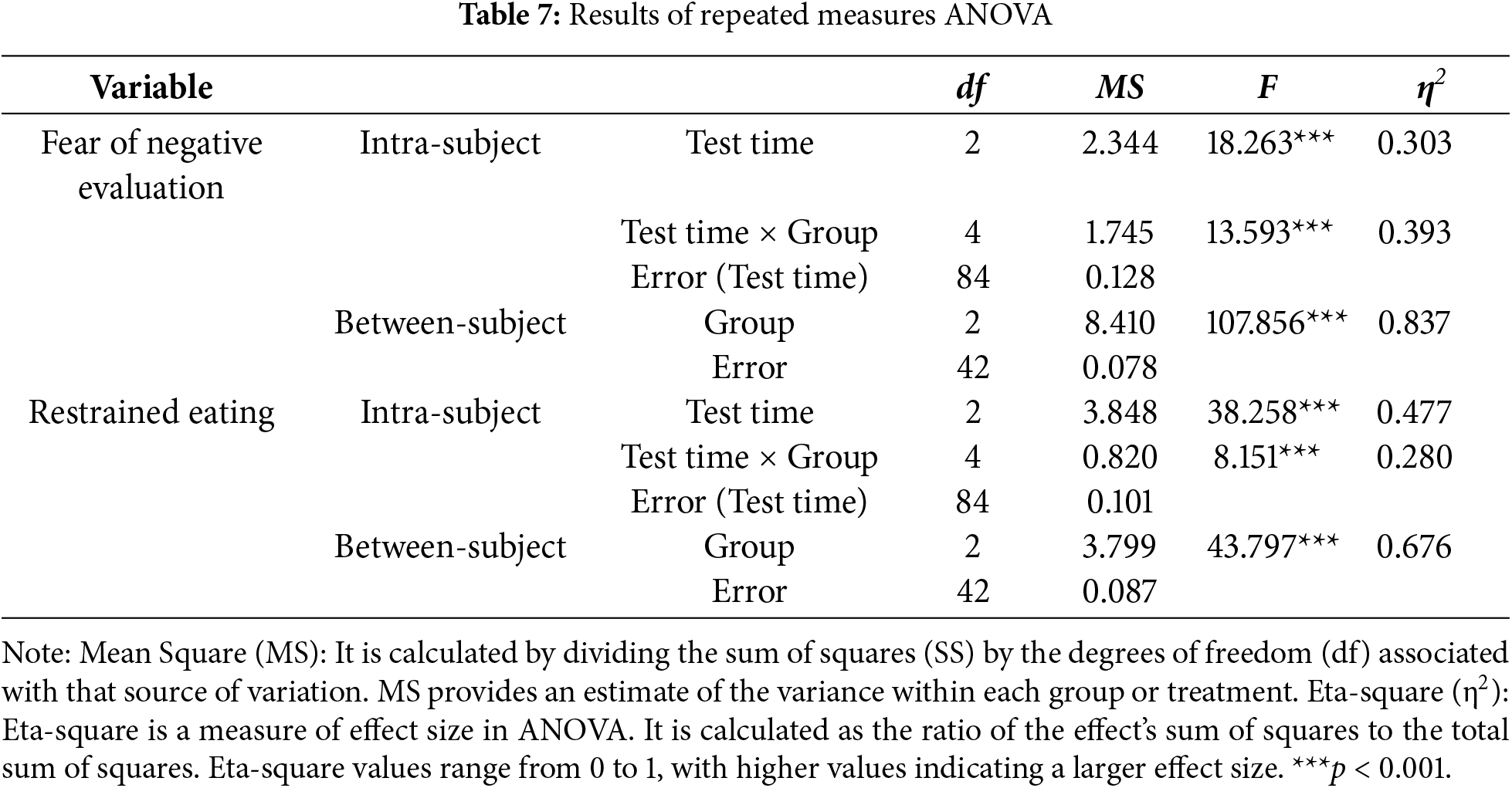
From the results of the table above, it can be seen that FNE mean scores differed significantly in terms of test time (F = 18.263, η2 = 0.303, p < 0.001) and interaction item test time × group (F = 13.593, η2 = 0.393, p < 0.001) and group (F = 107.856, η2 = 0.837, p < 0.001); in terms of restrained eating mean scores, the experimental, control, and placebo groups (F = 43.797, η2 = 0.676, p < 0.001) differed significantly; and the interaction item test time × group (F = 8.151, η2 = 0.28, p < 0.001) and test time (F = 38.258, η2 = 0.477, p < 0.001) were significant. Further simple effects analyses were necessary because the interaction between test time and group was significant for both FNE and restrained eating. The results are shown in Table 8.
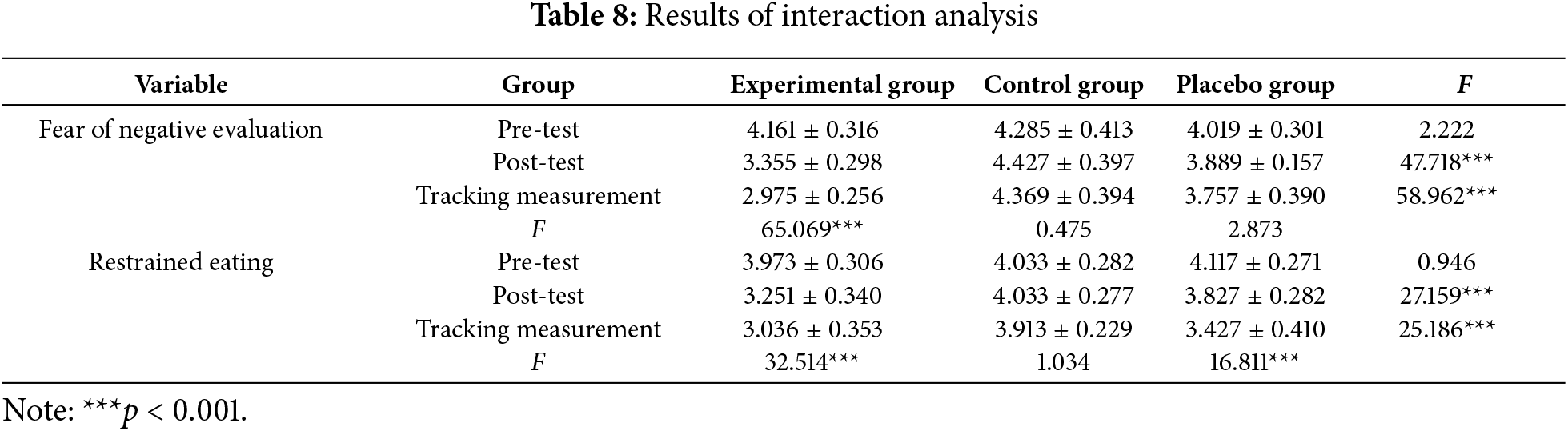
From the results of the above table, it can be seen that the mean score of FNE (F = 2.222, p > 0.05) and the mean score of restrained eating (F = 0.946, p > 0.05) at the pre-test did not differ significantly between the experimental group, the control group, and the placebo group, while at the post-test, there were significant differences between the mean scores of the three groups in terms of the mean scores of FNE (F = 47.718, p < 0.001) and the mean scores of the restrained eating (F = 27.159, p < 0.001) were significantly different, and after two-by-two comparisons, it was found that the mean FNE scores and the mean restrained eating scores of the participants in the experimental group were significantly lower than those of the participants in the control group as well as the placebo group. After measuring the three groups of participants again one month later, it was found that the participants’ FNE mean scores (F = 58.962, p < 0.001) and restrained eating mean scores (F = 25.186, p < 0.001) were still significantly different, and that the experimental group’s participants’ FNE mean scores and restrained eating mean scores were significantly lower than those of the control group and the placebo group. At different time points, there was a significant difference between the mean FNE scores (F = 65.069, p < 0.001) and the mean restrained eating scores (F = 32.514, p < 0.001) of the participants in the experimental group, and two-by-two comparisons revealed that the mean FNE scores and the mean restrained eating scores of the experimental group were significantly lower than those in the control group at the post-test and at the tracking measurement than they were at the pre-test. mean FNE scores (F = 0.475, p > 0.05) and mean restrained eating scores (F = 1.034, p > 0.05) were not significantly different, while there was no significant difference in the mean FNE scores of the participants in the placebo group (F = 2.873, p > 0.05), and there was a significant difference in the mean restrained eating scores (F = 16.811, p < 0.001).
To summarize the results, it can be stated that the intervention in this study can significantly reduce the level of FNE among female college students, which in turn reduces their restrained eating behaviors, and the intervention effect can be maintained after one month. The interaction between group and test time is depicted in Figs. 4 and 5.
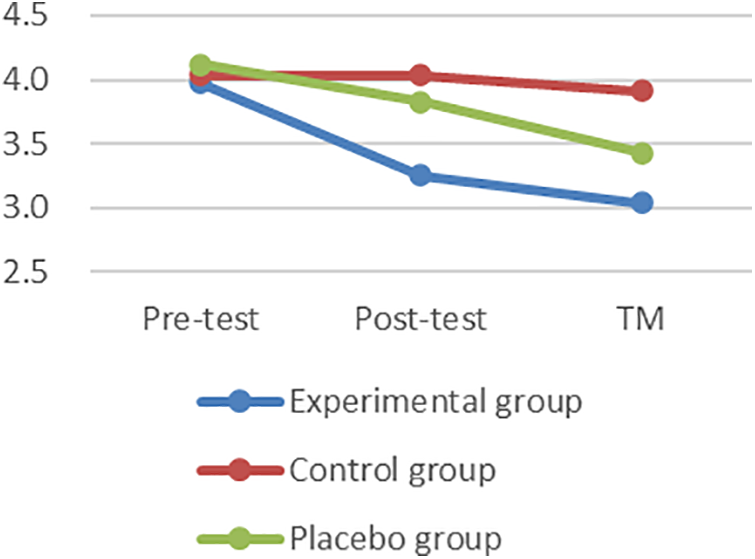
Figure 4: Interaction effect figure of fear of negative evaluation. TM = Tracking measurement
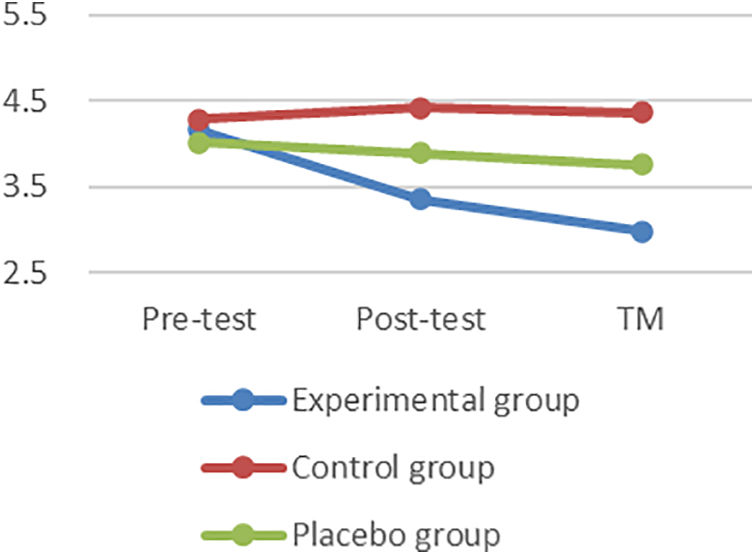
Figure 5: Interaction effect figure of Restrained Eating. TM = Tracking measurement
A comprehensive analysis of the literature reveals that a significant proportion of female college students experience or have experienced restrained eating, highlighting the need for intervention [69]. To effectively address this issue, it is essential to identify the factors influencing restrained eating. This study consists of two parts: Study 1 explores the relationship between FNE, physical appearance perfectionism, self-esteem, and restrained eating, while Study 2 develops a group psychological intervention based on Acceptance and Commitment Therapy to reduce FNE and evaluate its effectiveness.
Study 1 found that the detection rate of restrained eating among female college students in this study was 29.34%, which is relatively high. The results indicated that FNE positively predicts restrained eating, consistent with existing research [16]. Female college students with higher levels of FNE tend to be more concerned about others’ judgments and their own body image. As a result, some resort to dieting to achieve an ideal appearance, leading to long-term restrained eating behaviors. Additionally, physical appearance perfectionism partially mediated the relationship between FNE and restrained eating. Higher levels of FNE were associated with higher levels of physical appearance perfectionism, which in turn contributed to restrained eating. Female students who fear being judged negatively for their appearance may pursue a “perfect” body through restrictive eating. However, this often leads to failure in maintaining such behaviors, triggering a cycle of “restrained eating → failure → fear of appearance → FNE → desire for appearance perfection,” which exacerbates the risk of eating disorders and causes significant physical and psychological harm over time [70]. Furthermore, Study 1 found that self-esteem moderated the relationship between physical appearance perfectionism and restrained eating. Female college students with higher self-esteem exhibited lower levels of physical appearance perfectionism and engaged in fewer restrained eating behaviors. This finding aligns with prior research [38], suggesting that higher self-esteem is associated with greater body acceptance and a more positive mindset toward negative body image feedback. Those with higher self-esteem tend to view negative evaluations of their appearance more positively and are less likely to engage in extreme dieting behaviors [71]. Conversely, individuals with lower self-esteem are more likely to experience body dissatisfaction, which can lead to maladaptive behaviors such as restrained eating and further contribute to the development of eating disorders [10]. These findings underscore the importance of addressing both FNE and self-esteem in interventions aimed at reducing restrained eating among female college students.
Building on the findings of Study 1, Study 2 aimed to further investigate the impact of FNE on restrained eating. A literature review revealed that Acceptance and Commitment Therapy (ACT) effectively alleviates negative emotions, such as fear and anxiety, through techniques like mindfulness and cognitive reframing [48]. ACT has also demonstrated success in addressing eating-related behaviors and promoting psychological well-being [72,73]. Based on this theoretical foundation, Study 2 developed a group psychological intervention program using ACT to target the negative emotions contributing to restrained eating among female college students. The goal was to empirically validate the influencing factors and mechanisms behind restrained eating, while evaluating the effectiveness of ACT in reducing eating problems. The study also sought to explore whether ACT could improve mental health and prevent the development of eating disorders in the future. Through this intervention, the study aimed to provide practical insights into using ACT as a tool for addressing restrained eating behaviors.
Study 2 further confirmed the role of ACT in alleviating negative emotions such as fear and anxiety, consistent with previous studies [74]. Meanwhile, Study 1 found that self-esteem modulates the mediating pathway through physical appearance perfectionism, and existing studies suggest that group psychological interventions using ACT can enhance self-esteem [75]. As a third-generation behavioral therapy, ACT emphasizes proactive acceptance of negative emotions and cognitive restructuring, which helps female college students reduce avoidant behaviors and interrupt negative thinking patterns. Identifying and disrupting these negative thought processes during the intervention process holds significant potential for cognitive restructuring, thus enhancing psychological flexibility.
ACT alleviates negative emotions, such as apprehension, through techniques like positive breathing exercises. These techniques help participants focus on the present moment and themselves, reducing repetitive rumination on painful experiences. As participants’ levels of positive thinking increased, they reported improvements in their sleep, executive function, and clarity of values, which helped them move toward committing to action, accepting negative comments, and focusing on healthier ways of achieving a fit body, such as exercise, instead of restricting their diet for the sake of a perfect body. The metaphorical short story intervention, based on relational framing theory [76], helped participants realize the similarities between their own situations and those in the stories. It showed that avoidance and struggle might only worsen negative emotions, and participants were encouraged to reduce resistance to their own emotions and accept negative evaluations from others and themselves.
While ACT has shown positive effects in alleviating negative emotions and reducing restrictive eating behaviors, there are several challenges in its practical implementation. First, ACT interventions require trained therapists, which can be resource-intensive. Additionally, its application needs to be highly individualized to cater to the unique needs and cultural backgrounds of participants, which raises questions about its generalizability [77]. Future studies should explore how to adapt ACT interventions to different populations and settings, ensuring their effectiveness across diverse contexts.
In terms of scaling up ACT interventions, it is important to address potential barriers such as limited resources, participant engagement, and the sustainability of the intervention effects. One possible solution is the integration of online ACT interventions, which can reach a wider audience and reduce the resource burden [78]. However, ensuring long-term engagement and the continued effectiveness of online interventions presents its own set of challenges. To overcome these, future research could explore the use of Artificial Intelligence (AI) technologies in combination with ACT [79]. AI could assist in monitoring emotional states, tailoring intervention content, and providing real-time support, thereby increasing the flexibility and efficiency of the intervention.
In summary, ACT has proven effective in alleviating negative emotions and reducing restrictive eating behaviors among female college students, but its practical application faces challenges related to resource requirements, individualization, and scalability. Future research should investigate how to address these challenges, particularly in terms of adapting ACT for diverse cultural contexts and integrating new technologies such as AI to enhance its reach and effectiveness.
Our study has some limitations. First, the sample in this study is predominantly focused on female college students from Chinese universities, which limits the generalizability of the findings to other populations. To improve the representativeness and broaden the scope of the research, future studies could extend the sample to include female college students from different countries and cultural backgrounds, providing a more global perspective. Second, the data and results of this study are based on a cross-sectional design, which captures a snapshot of the variables at one point in time. This does not allow us to determine causal relationships or the long-term development of these variables. Therefore, future research should incorporate longitudinal designs to track changes over time and more accurately assess the relationships between the variables. Third, the group psychological intervention in this study was conducted offline, which may limit its accessibility and scalability. Future studies could explore the feasibility of online interventions and consider combining different methods, such as online and offline approaches, to enhance the effectiveness and reach of the intervention.
First, fear of negative evaluation significantly and positively predicted both restrained eating and physical appearance perfectionism. Additionally, physical appearance perfectionism was found to significantly and positively predict restrained eating, and it partially mediated the relationship between fear of negative evaluation and restrained eating. Second, self-esteem moderated the partial mediation process of physical appearance perfectionism in the relationship between fear of negative evaluation and restrained eating. Third, a group psychological intervention based on Acceptance and Commitment Therapy was effective in reducing the occurrence of restrained eating behaviors by lowering the level of fear of negative evaluation among female college students.
Acknowledgement: We extend our sincere gratitude to all the participants in this study, as well as the editors and reviewers for their assistance.
Funding Statement: This research received no external funding.
Author Contributions: Study conception and design: Sisi Li, Weijian Fu; data collection: Wenyi Liu; analysis and interpretation of results: Sisi Li, Weijian Fu, Nailiang Zhong; draft manuscript preparation: Weijian Fu and Wenyi Liu. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: Data supporting the results of this study are available upon reasonable request by contacting the corresponding author.
Ethics Approval: The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Hechi University (No. H24016, date of approval: 10 March 2024). All participants signed the informed consent in this study.
Conflicts of Interest: The authors declare no conflicts of interest to report regarding the present study.
References
1. Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9(7):446–61. doi:10.1016/S2213-8587(21)00118-2. [Google Scholar] [PubMed] [CrossRef]
2. Strodl E, Markey C, Aimé A, Rodgers RF, Dion J, Lo Coco G, et al. A cross-country examination of emotional eating, restrained eating and intuitive eating: measurement invariance across eight countries. Body Image. 2020;35(2):245–54. doi:10.1016/j.bodyim.2020.09.013. [Google Scholar] [PubMed] [CrossRef]
3. Salimi N, Gere B, Talley W, Irioogbe B. College students mental health challenges: concerns and considerations in the COVID-19 pandemic. J Coll Stud Psychother. 2021;37(1):39–51. doi:10.1080/87568225.2021.1890298. [Google Scholar] [CrossRef]
4. Wood CI, Yu Z, Sealy D-A, Moss I, Zigbuo-Wenzler E, McFadden C, et al. Mental health impacts of the COVID-19 pandemic on college students. J Am Coll Health. 2022;72(2):463–8. doi:10.1080/07448481.2022.2040515. [Google Scholar] [PubMed] [CrossRef]
5. D’Adamo L, Ghaderi A, Rohde P, Gau JM, Shaw H, Stice E. Evaluating whether a peer-led dissonance-based eating disorder prevention program prevents onset of each eating disorder type. Psychol Med. 2023;53(15):7214–21. doi:10.1017/S0033291723000739. [Google Scholar] [PubMed] [CrossRef]
6. Lee A, Chan W, Ng JCK. The role of fear of negative evaluation on the effects of self-control on affective states and life satisfaction: a moderated mediation analysis. Curr Psychol. 2023;42(35):31280–93. doi:10.1007/s12144-022-04130-7. [Google Scholar] [PubMed] [CrossRef]
7. Rais O, Norton PJ. The effects of fear of evaluation as a mediator of the relationship between perfectionism and social anxiety in college students. Curr Psychol. 2024;43(48):36921–32. doi:10.1007/s12144-024-06978-3. [Google Scholar] [CrossRef]
8. Blanco-Ferreiro A, Candal-Pedreira C, Sendón B, Santiago-Pérez MI, Rey-Brandariz J, Varela-Lema L, et al. Self-perceived body weight and weight status: analysis of concordance by age group and sex. Pub Health. 2024;229(2):160–6. doi:10.1016/j.puhe.2024.02.007. [Google Scholar] [PubMed] [CrossRef]
9. Miles S, Nedeljkovic M, Phillipou A. Investigating differences in cognitive flexibility, clinical perfectionism, and eating disorder-specific rumination across anorexia nervosa illness states. Eat Disord. 2023;31(6):610–31. doi:10.1080/10640266.2023.2206751. [Google Scholar] [PubMed] [CrossRef]
10. Petersson S, Johnsson P, Perseius K-I. A sisyphean task: experiences of perfectionism in patients with eating disorders. J Eat Disord. 2017;5(1):3. doi:10.1186/s40337-017-0136-4. [Google Scholar] [PubMed] [CrossRef]
11. Beckers D, Burk WJ, Larsen JK, Cillessen AH. The bidirectional associations between self-esteem and problematic eating behaviors in adolescents. Int J Eat Disord. 2024;57(1):104–15. doi:10.1002/eat.24083. [Google Scholar] [PubMed] [CrossRef]
12. Gloster AT, Walder N, Levin ME, Twohig MP, Karekla M. The empirical status of acceptance and commitment therapy: a review of meta-analyses. J Contextual Behav Sci. 2020;18(1):181–92. doi:10.1016/j.jcbs.2020.09.009. [Google Scholar] [CrossRef]
13. Bai Z, Luo S, Zhang L, Wu S, Chi I. Acceptance and commitment therapy (ACT) to reduce depression: a systematic review and meta-analysis. J Affect Disord. 2020;260(2):728–37. doi:10.1016/j.jad.2019.09.040. [Google Scholar] [PubMed] [CrossRef]
14. Downing VR, Cooper KM, Cala JM, Gin LE, Brownell SE. Fear of negative evaluation and student anxiety in community college active-learning science courses. CBE Life Sci Educ. 2020;19(2):ar20. doi:10.1187/cbe.19-09-0186. [Google Scholar] [PubMed] [CrossRef]
15. Sander J, Moessner M, Bauer S. Depression, anxiety and eating disorder-related impairment: moderators in female adolescents and young adults. Int J Environ Res Public Health. 2021;18(5):2779. doi:10.3390/ijerph18052779. [Google Scholar] [PubMed] [CrossRef]
16. Trompeter N, Austen E, Bussey K, Reilly EE, Cunningham ML, Mond J, et al. Examination of bidirectional relationships between fear of negative evaluation and weight/shape concerns over 3 years: a longitudinal cohort study of Australian adolescents. Int J Eat Disord. 2023;56(3):646–53. doi:10.1002/eat.23881. [Google Scholar] [PubMed] [CrossRef]
17. Breton É, Dufour R, Côté SM, Dubois L, Vitaro F, Boivin M, et al. Developmental trajectories of eating disorder symptoms: a longitudinal study from early adolescence to young adulthood. J Eat Disord. 2022;10(1):84. doi:10.1186/s40337-022-00603-z. [Google Scholar] [PubMed] [CrossRef]
18. Hagerman CJ, Stock ML, Beekman JB, Yeung EW, Persky S. The ironic effects of dietary restraint in situations that undermine self-regulation. Eat Behav. 2021;43(11):101579. doi:10.1016/j.eatbeh.2021.101579. [Google Scholar] [PubMed] [CrossRef]
19. Linardon J, Messer M, Shatte A, Skvarc D, Rosato J, Rathgen A, et al. Targeting dietary restraint to reduce binge eating: a randomised controlled trial of a blended internet-and smartphone app-based intervention. Psychol Med. 2023;53(4):1277–87. doi:10.1017/S0033291721002786. [Google Scholar] [PubMed] [CrossRef]
20. Kukk K, Akkermann K. Emotion regulation difficulties and dietary restraint independently predict binge eating among men. Eat Weight Disord. 2020;25(6):1553–60. doi:10.1007/s40519-019-00791-9. [Google Scholar] [PubMed] [CrossRef]
21. Stewart TM, Martin CK, Williamson DA. The complicated relationship between dieting, dietary restraint, caloric restriction, and eating disorders: is a shift in public health messaging warranted? Int J Environ Res Public Health. 2022;19(1):491. doi:10.3390/ijerph19010491. [Google Scholar] [PubMed] [CrossRef]
22. Sigurvinsdottir R, Soring K, Kristinsdottir K, Halfdanarson SG, Johannsdottir KR, Vilhjalmsson HH, et al. Social anxiety, fear of negative evaluation, and distress in a virtual reality environment. Behav Chang. 2021;38(2):109–18. doi:10.1017/bec.2021.4. [Google Scholar] [CrossRef]
23. Hazzard VM, Hooper L, Larson N, Loth KA, Wall MM, Neumark-Sztainer D. Associations between severe food insecurity and disordered eating behaviors from adolescence to young adulthood: findings from a 10-year longitudinal study. Prev Med. 2022;154(5):106895. doi:10.1016/j.ypmed.2021.106895. [Google Scholar] [PubMed] [CrossRef]
24. Ferrara M, Langiano E, Falese L, Diotaiuti P, Cortis C, De Vito E. Changes in physical activity levels and eating behaviours during the COVID-19 pandemic: sociodemographic analysis in university students. Int J Environ Res Public Health. 2022;19(9):5550. doi:10.3390/ijerph19095550. [Google Scholar] [PubMed] [CrossRef]
25. Zuroff DC, Clegg KA, Levine SL, Haward B, Thode S. Contributions of trait, domain, and signature components of self-criticism to stress generation. Pers Individ Dif. 2021;173(1):110603. doi:10.1016/j.paid.2020.110603. [Google Scholar] [CrossRef]
26. Khossousi V, Greene D, Shafran R, Callaghan T, Dickinson S, Egan SJ. The relationship between perfectionism and self-esteem in adults: a systematic review and meta-analysis. Behav Cogn Psychother. 2024;1–20. doi:10.1017/S1352465824000249. [Google Scholar] [PubMed] [CrossRef]
27. Shafique N, Gul S, Raseed S. Perfectionism and perceived stress: the role of fear of negative evaluation. Int J Ment Health. 2017;46(4):312–26. doi:10.1080/00207411.2017.1345046. [Google Scholar] [CrossRef]
28. Neshat Z, Farah Bijari A, Dehshiri G. The relationship between perfectionism and interpersonal sensitivity with self-compassion in university students: the mediation of repetitive negative thinking. Cogn Process. 2024;25(1):107–20. doi:10.1007/s10339-023-01163-z. [Google Scholar] [PubMed] [CrossRef]
29. Barnett MD, Sharp KJ. Maladaptive perfectionism, body image satisfaction, and disordered eating behaviors among U.S. college women: the mediating role of self-compassion. Pers Individ Diff. 2016;99(4):225–34. doi:10.1016/j.paid.2016.05.004. [Google Scholar] [CrossRef]
30. Miranda S, Duarte M. How perfectionism reduces positive word-of-mouth: the mediating role of Perceived Social Risk. Psychol Mark. 2021;39(2):255–70. doi:10.1002/mar.21593. [Google Scholar] [CrossRef]
31. Linardon J, McClure Z, Tylka TL, Fuller-Tyszkiewicz M. Body appreciation and its psychological correlates: a systematic review and meta-analysis. Body Image. 2022;42:287–96. doi:10.1016/j.bodyim.2022.07.003. [Google Scholar] [PubMed] [CrossRef]
32. Williams BM, Levinson CA. Intolerance of uncertainty and maladaptive perfectionism as maintenance factors for eating disorders and obsessive-compulsive disorder symptoms. Eur Eat Disord Rev. 2021;29(1):101–11. doi:10.1002/erv.2807. [Google Scholar] [PubMed] [CrossRef]
33. Flett GL, Hewitt PL, Nepon T, Sherry SB, Smith M. The destructiveness and public health significance of socially prescribed perfectionism: a review, analysis, and conceptual extension. Clin Psychol Rev. 2022;93(12):102130. doi:10.1016/j.cpr.2022.102130. [Google Scholar] [PubMed] [CrossRef]
34. Howard TLM, Williams MO, Woodward D, Fox JRE. The relationship between shame, perfectionism and Anorexia Nervosa: a grounded theory study. Psychol Psychother. 2023;96(1):40–55. doi:10.1111/papt.12425. [Google Scholar] [PubMed] [CrossRef]
35. Polivy J, Garner DM, Garfinkel PE. Causes and consequences of the current preference for thin female physiques. In: Herman CP, Zanna MP, Higgins ET, editors. Physical appearance, stigma, and social behavior. New York: Routledge; 2022. p. 89–112. doi:10.4324/9781003308928-5. [Google Scholar] [CrossRef]
36. Orth U, Robins RW. Is high self-esteem beneficial? Revisiting a classic question. Am Psychol. 2022;77(1):5–17. doi:10.1037/amp0000922. [Google Scholar] [PubMed] [CrossRef]
37. Cao X, Liu X. Self-esteem as a predictor of anxiety and academic self-efficacy among Chinese university students: a cross-lagged analysis. Curr Psychol. 2024;43(22):19628–38. doi:10.1007/s12144-024-05781-4. [Google Scholar] [CrossRef]
38. Junghans-Rutelonis AN, Suorsa KI, Tackett AP, Burkley E, Chaney JM, Mullins LL. Self-esteem, self-focused attention, and the mediating role of fear of negative evaluation in college students with and without asthma. J Am Coll Health. 2015;63(8):554–62. doi:10.1080/07448481.2015.1057146. [Google Scholar] [PubMed] [CrossRef]
39. Wang Y, Qiao X, Wang J, Wang H, Lei L. Peer appearance teasing and restrained eating among Chinese adolescent girls: a mediation model of fear of negative appearance evaluation and body surveillance. Child Psychiatry Hum Dev. 2024;55(4):1127–34. doi:10.1007/s10578-022-01478-6. [Google Scholar] [PubMed] [CrossRef]
40. Caso D, Miriam C, Rosa F, Mark C. Unhealthy eating and academic stress: the moderating effect of eating style and BMI. Health Psychol Open. 2020;7(2):2055102920975274. doi:10.1177/2055102920975274. [Google Scholar] [PubMed] [CrossRef]
41. Miegel F, Moritz S, Wagener F, Cludius B, Jelinek L. Self-esteem mediates the relationship between perfectionism and obsessive-compulsive symptoms. Pers Individ Differ. 2020;167(2):110239. doi:10.1016/j.paid.2020.110239. [Google Scholar] [CrossRef]
42. Chai L, Yang W, Zhang J, Chen S, Hennessy DA, Liu Y. Relationship between perfectionism and depression among Chinese college students with self-esteem as a mediator. OMEGA J Death Dying. 2020;80(3):490–503. doi:10.1177/0030222819849746. [Google Scholar] [PubMed] [CrossRef]
43. Park H, Jeong DY. Psychological well-being, life satisfaction, and self-esteem among adaptive perfectionists, maladaptive perfectionists, and nonperfectionists. Pers Individ Diff. 2015;72:165–70. doi:10.1016/j.paid.2014.08.031. [Google Scholar] [CrossRef]
44. Han GB, Wang CDC, Jin L, Bismar D. Insecure attachment, maladaptive perfectionism, self-esteem, depression, and bulimic behaviors for college women: a cross-cultural comparison. Int J Adv Counselling. 2022;44(2):197–219. doi:10.1007/s10447-021-09462-w. [Google Scholar] [CrossRef]
45. Zamani Sani SH, Fathirezaie Z, Gerber M, Pühse U, Bahmani DS, Bashiri M, et al. Self-esteem and symptoms of eating-disordered behavior among female adolescents. Psychol Rep. 2020;124(4):1515–38. doi:10.1177/0033294120948226. [Google Scholar] [PubMed] [CrossRef]
46. Lo Coco G, Salerno L, Ingoglia S, Tasca GA. Self-esteem and binge eating: do patients with binge eating disorder endorse more negatively worded items of the Rosenberg self-esteem scale? J Clin Psychol. 2020;77(3):818–36. doi:10.1002/jclp.23065. [Google Scholar] [PubMed] [CrossRef]
47. Kim S. Eating disorders, body dissatisfaction, and self-esteem among South Korean women. Soc Behav Pers. 2018;46(9):1537–46. doi:10.2224/sbp.6801. [Google Scholar] [CrossRef]
48. Stojcic I, Dong X, Ren X. Body image and sociocultural predictors of body image dissatisfaction in Croatian and Chinese women. Front Psychol. 2020;11:731. doi:10.3389/fpsyg.2020.00731. [Google Scholar] [PubMed] [CrossRef]
49. Norton AR, Abbott MJ, Dobinson KA, Pepper KL, Guastella AJ. Rescripting social trauma: a pilot study investigating imagery rescripting as an adjunct to cognitive behaviour therapy for social anxiety disorder. Cogn Ther Res. 2021;45(6):1180–92. doi:10.1007/s10608-021-10221-9. [Google Scholar] [CrossRef]
50. Auyeung K, Hawley LL, Grimm K, McCabe R, Rowa K. Fear of negative evaluation and rapid response to treatment during cognitive behaviour therapy for social anxiety disorder. Cogn Ther Res. 2020;44(3):526–37. doi:10.1007/s10608-020-10077-5. [Google Scholar] [CrossRef]
51. van Dis EAM, Hagenaars MA, Bockting CLH, Engelhard IM. Reducing negative stimulus valence does not attenuate the return of fear: two counterconditioning experiments. Behav Res Ther. 2019;120(3):103416. doi:10.1016/j.brat.2019.103416. [Google Scholar] [PubMed] [CrossRef]
52. Hosseini M, Ghasemtabar S, Fayyaz I, Arab S, Naghashian H, Poudineh Z. Music therapy: an effective approach in improving social skills of children with autism. Adv Biomed Res. 2015;4(1):157. doi:10.4103/2277-9175.161584. [Google Scholar] [PubMed] [CrossRef]
53. Feruglio S, Matiz A, Grecucci A, Pascut S, Fabbro F, Crescentini C. Differential effects of mindfulness meditation conditions on repetitive negative thinking and subjective time perspective: a randomized active-controlled study. Psychol Health. 2020;36(11):1275–98. doi:10.1080/08870446.2020.1836178. [Google Scholar] [PubMed] [CrossRef]
54. Melnyk BM, Amaya M, Szalacha LA, Hoying J, Taylor T, Bowersox K. Feasibility, acceptability, and preliminary effects of the cope online cognitive-behavioral skill-building program on Mental Health Outcomes and academic performance in freshmen college students: a randomized controlled pilot study. J Child Adolesc Psychiatr Nurs. 2015;28(3):147–54. doi:10.1111/jcap.12119. [Google Scholar] [PubMed] [CrossRef]
55. Nuttall FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. 2015;50(3):117–28. doi:10.1097/NT.0000000000000092. [Google Scholar] [PubMed] [CrossRef]
56. Zaccagni L, Rinaldo N, Bramanti B, Mongillo J, Gualdi-Russo E. Body image perception and body composition: assessment of perception inconsistency by a new index. J Transl Med. 2020;18(1):20. doi:10.1186/s12967-019-02201-1. [Google Scholar] [PubMed] [CrossRef]
57. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9(6):373–92. doi:10.1016/S2213-8587(21)00045-0. [Google Scholar] [PubMed] [CrossRef]
58. Weeks JW, Heimberg RG, Rodebaugh TL. The fear of positive evaluation scale: assessing a proposed cognitive component of social anxiety. J Anxiety Disord. 2008;22(1):44–55. doi:10.1016/j.janxdis.2007.08.002. [Google Scholar] [PubMed] [CrossRef]
59. Chen Z. For fear of negative evaluation and test anxiety in middle school students. Chin Ment Health J. 2002;16(12):855–7 (In Chinese). [Google Scholar]
60. Shen ZL, Cai TS. Disposal to the 8th item of rosenberg self-esteem scale. Chin Ment Health J. 2008;22(9):661–3 (In Chinese). [Google Scholar]
61. Yang H, Stoeber J. The physical appearance perfectionism scale: development and preliminary validation. J Psychopathol Behav Assess. 2012;34(1):69–83. doi:10.1007/s10862-011-9260-7. [Google Scholar] [CrossRef]
62. van Strien T, Frijters JE, Bergers GP, Defares PB. The dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. J Eat Disord. 1986;5:295–315. doi:10.1002/1098-108X(198602)5:2%3C295::AID-EAT2260050209%3E3.0.CO;2-T. [Google Scholar] [CrossRef]
63. Li YN, Liu Y, Bao J. The applicability of Dutch eating behavior questionnaire (DEBQ) in Chinese college students. Chin J Clin Psychol. 2018;2:277–81. (In Chinese). [Google Scholar]
64. Kim HY. Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restor Dent Endod. 2013;38(1):52–4. doi:10.5395/rde.2013.38.1.52. [Google Scholar] [PubMed] [CrossRef]
65. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44(1):1–25. doi:10.1016/j.brat.2005.06.006. [Google Scholar] [PubMed] [CrossRef]
66. Hayes SC, Levin ME, Plumb-Vilardaga J, Villatte JL, Pistorello J. Acceptance and commitment therapy and contextual behavioral science: examining the progress of a distinctive model of behavioral and cognitive therapy. Behav Ther. 2013;44(2):180–98. doi:10.1016/j.beth.2009.08.002. [Google Scholar] [PubMed] [CrossRef]
67. Fang S, Ding D. The efficacy of group-based acceptance and commitment therapy on psychological capital and school engagement: a pilot study among Chinese adolescents. J Contextual Behav Sci. 2020;16(1):134–43. doi:10.1016/j.jcbs.2020.04.005. [Google Scholar] [CrossRef]
68. Ma TW, Yuen ASK, Yang Z. The efficacy of acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. Clin J Pain. 2023;39(3):147–57. doi:10.1097/AJP.0000000000001096. [Google Scholar] [PubMed] [CrossRef]
69. Yao L, Niu G, Sun X. Body image comparisons on social networking sites and Chinese female college students’ restrained eating: the roles of body shame, body appreciation, and body mass index. Sex Roles. 2021;84:465–76. doi:10.1007/s11199-020-01179-1. [Google Scholar] [CrossRef]
70. House ET, Gow ML, Lister NB, Baur LA, Garnett SP, Paxton SJ, et al. Pediatric weight management, dietary restraint, dieting, and eating disorder risk: a systematic review. Nutr Rev. 2021;79(10):1114–33. doi:10.1093/nutrit/nuaa127. [Google Scholar] [PubMed] [CrossRef]
71. Wang R, Gan Y, Wang X, Li J, Lipowska M, Izydorczyk B, et al. The mediating effect of negative appearance evaluation on the relationship between eating attitudes and sociocultural attitudes toward appearance. Front Psychiatry. 2022;13:776842. doi:10.3389/fpsyt.2022.776842. [Google Scholar] [PubMed] [CrossRef]
72. Fogelkvist M, Gustafsson SA, Kjellin L, Parling T. Acceptance and commitment therapy to reduce eating disorder symptoms and body image problems in patients with residual eating disorder symptoms: a randomized controlled trial. Body Image. 2020;32(Suppl. 20):155–66. doi:10.1016/j.bodyim.2020.01.002. [Google Scholar] [PubMed] [CrossRef]
73. Iturbe I, Echeburúa E, Maiz E. The effectiveness of acceptance and commitment therapy upon weight management and psychological well-being of adults with overweight or obesity: a systematic review. Clin Psychol Psychother. 2022;29(3):837–56. doi:10.1002/cpp.2695. [Google Scholar] [PubMed] [CrossRef]
74. Ruiz FJ, Luciano C, Flórez CL, Suárez-Falcón JC, Cardona-Betancourt V. A multiple-baseline evaluation of acceptance and commitment therapy focused on repetitive negative thinking for comorbid generalized anxiety disorder and depression. Front Psychol. 2020;11:356. doi:10.3389/fpsyg.2020.00356. [Google Scholar] [PubMed] [CrossRef]
75. Kianpour Barjoee L, Amini N, Keykhosrovani M, Shafiabadi A. Effectiveness of positive thinking training on perceived stress, metacognitive beliefs, and death anxiety in women with breast cancer. Arch Breast Cancer. 2022;9(2):195–203. doi:10.32768/abc.202292195-203. [Google Scholar] [CrossRef]
76. Barnes-Holmes D, Harte C. Relational frame theory 20 years on: the Odysseus voyage and beyond. J Exp Anal Behav. 2022;117(2):240–66. doi:10.1002/jeab.733. [Google Scholar] [PubMed] [CrossRef]
77. Towey-Swift KD, Lauvrud C, Whittington R. Acceptance and commitment therapy (ACT) for professional staff burnout: a systematic review and narrative synthesis of controlled trials. J Ment Health. 2023;32(2):452–64. doi:10.1080/09638237.2021.2022628. [Google Scholar] [PubMed] [CrossRef]
78. Trindade IA, Guiomar R, Carvalho SA, Duarte J, Lapa T, Menezes P, et al. Efficacy of online-based acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. J Pain. 2021;22(11):1328–42. doi:10.1016/j.jpain.2021.04.003. [Google Scholar] [PubMed] [CrossRef]
79. Naor N, Frenkel A, Winsberg M. Improving well-being with a mobile artificial intelligence-powered acceptance commitment therapy tool: pragmatic retrospective study. JMIR Form Res. 2022;6(7):e36018. doi:10.2196/36018. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2025 The Author(s). Published by Tech Science Press.
Copyright © 2025 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools