
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

The Effects of Childhood Trauma on College Students’ Depressive Symptoms: The Mediation Role of Subjective Well-Being and the Moderation Role of Resilience
1 School of information, Yunnan University of Chinese Medicine, Kunming, 650500, China
2 Yunnan Key Laboratory of Dai and Yi Medicines, Yunnan University of Chinese Medicine, Kunming, 650500, China
3 Faculty of Education, Yunnan Normal University, Kunming, 650500, China
* Corresponding Author: Keli Yin. Email:
(This article belongs to the Special Issue: Social Stress, Adversity, and Mental Health in Transitional China)
International Journal of Mental Health Promotion 2024, 26(9), 757-766. https://doi.org/10.32604/ijmhp.2024.049922
Received 22 January 2024; Accepted 01 August 2024; Issue published 20 September 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: The enduring and detrimental impact of childhood trauma on later health and well-being is now well established. However, research on the relationship between childhood trauma and depressive symptoms, along with the potential risk and protective factors, is insufficient in the context of Chinese college student population. Methods: Data on childhood trauma, depressive symptoms, resilience, and subjective well-being were collected through surveys conducted with 367 Chinese university students. The data collected in this study were analyzed using SPSS 26.0 and PROCESS 3.5. Results: The results revealed that subjective well-being mediated the relationship between childhood trauma and depressive symptoms among college students, with direct and indirect effects accounting for 59.46% and 40.54% of the total effect, respectively. The pathway process between subjective well-being and depressive symptoms was moderated by resilience, whereby an increase in resilience levels corresponded to a gradual escalation in the predictive power of subjective well-being on depressive symptoms. Conclusion: The study indicates that childhood trauma significantly and positively predicts depressive symptoms among college students, and it can also directly predict depressive symptoms through the mediating effect of subjective well-being. Elevating levels of psychological resilience and subjective well-being among college students can mitigate depression and promote psychological well-being. From the perspective of positive psychology, the present study provides a new perspective for the prevention and intervention of depressive symptoms among college students.Keywords
Depression as the most prevalent mood disorder [1], stands as a significant risk factor influencing the holistic well-being of individuals and has emerged as the second leading cause of disability worldwide [2]. Depression is projected to become the leading cause of disease burden and mortality worldwide by 2030 [3]. Typically, in the early adulthood stage ranging from 18 to 25 years old, college students, due to their ongoing physical and psychological development, often experience inner conflicts when confronted with various academic and life stressors, which can lead to the onset of adverse emotional states such as depression [4]. Research indicates that college students constitute a high-risk group for depression, with incidence rates steadily increasing [5,6]. Prolonged depression among college students can result in difficulties in interpersonal relationships, impaired cognitive functions, sleep disturbances [7], academic maladjustment, leading to negative outcomes such as retention or dropping out [8], and may even culminate in suicidal ideation and behavior, posing a threat to life safety [9,10].
Influenced by academic pressures, interpersonal dynamics, emotional factors, and employment prospects, the detection rate of depression among Chinese university students exceeds that of the general population or non-university student cohorts [11,12]. Moreover, according to findings from the “China National Mental Health Development Report (2019–2020)”, 18.5% of university students exhibit depressive tendencies, with 4.2% displaying a high risk of depression [13], a trend that is showing a yearly increase [14,15]. Without appropriate intervention and guidance during this period, depressive tendencies can escalate into more severe depressive disorders. Previous studies indicate that both the occurrence and duration of trauma during childhood significantly impact individual psychological well-being [16], with research confirming childhood trauma as a crucial risk factor for depression [17,18]. Individuals with early trauma experiences are 2.03 times more likely to develop depression compared to those without such experiences [19]. Childhood trauma, therefore, acts as a latent “time bomb” within some college students, posing a potential threat to their mental health. Given the high prevalence of depression among college students and its severe consequences, further exploration of the influencing factors and developmental mechanisms underlying depression in this population is of paramount importance, providing valuable theoretical support for the prevention and intervention of psychological issues among college students.
Childhood trauma and depression
Childhood trauma, as a significant factor impacting the physical and mental health development of children, has garnered increasing attention in recent years [20]. Childhood trauma refers to one or more experiences of exposure to trauma, neglect, dysfunctional family dynamics, or other adverse circumstances before the age of 18 [21]. Existing research indicates that childhood trauma can have profound and enduring effects on the physical and mental health of children, persisting into adulthood and throughout life. Compared to individuals without traumatic experiences, children who experience trauma are more susceptible to mental health disorders such as depression [22,23], bipolar disorder [24,25], anxiety disorders [26,27], as well as alcohol and substance trauma [28–30].
Beyond genetic and biological factors, childhood trauma, as a negative stress experienced in early life, has been substantiated by multiple studies as a predictive factor for depression in adulthood [31,32]. Research indicates that exposure to a greater number of childhood trauma experiences is associated with a higher occurrence of depressive symptoms [33]. According to the perspective of emotion regulation theory, children who have experienced childhood trauma find it more challenging to control their negative thoughts when faced with negative events, thereby increasing susceptibility to depression [34,35]. Furthermore, previous studies have shown a significant correlation between childhood trauma and depressive symptoms. Moreover, research indicates that the longer and more frequent the duration of trauma, the greater the likelihood of elevated levels of depression [36,37].
The mediating role of subjective well-being
Subjective well-being, as a crucial positive emotional experience, entails individuals’ overall evaluation of their life quality based on certain external or internal standards [38]. Serving as a positive psychological experience for individuals, subjective well-being significantly positively predicts levels of mental health [39]. Moreover, higher levels of subjective well-being can enhance individuals’ positive resources and serve as a protective factor in reducing the incidence of depression [40]. For instance, Corcoran and McNulty observed that childhood adversities indirectly diminished subjective well-being through attachment mechanisms among university students [41]. Additionally, Zhang found a significant negative correlation between subjective well-being and depression in a study examining the relationship between subjective well-being and depression among 348 teacher trainees [42]. Research on childhood trauma and subjective well-being also indicates that children who experience childhood trauma lack a sense of security, leading to long-term emotional downturns and reduced subjective well-being, consequently resulting in various emotional symptoms and psychological distress [43,44]. Greger study results demonstrate that childhood trauma can negatively predict adolescents’ subjective well-being [45]. Similarly, Oshio et al. indicated that childhood trauma significantly reduced subjective well-being during adulthood [46]. The neurobiological perspective emphasizes that childhood trauma over-activates brain structures responsible for emotion-laden memories while disrupting neutral memories [47,48].
While a substantial body of research indicates that childhood maltreatment is a risk factor for depressive symptoms among college students, not all individuals who experience childhood trauma ultimately develop depression or poor psychological states [49]. One important protective factor against the toxic stress of childhood trauma is resilience [50]. Resilience refers to an individual’s ability to maintain an optimistic, confident, positive, and adaptive psychological state in the face of adversity, pressure, and setbacks, which can assist individuals in better adapting to life’s changes and challenges [51,52]. Individuals with higher level of resilience have better well-being and a lower risk of developing psychopathology [53].
Resilience as a protective factor against childhood maltreatment, not only reduces the impact of childhood trauma on adult depression [54] but also lowers the risk of developing mental illness and enhances subjective well-being [55]. For individuals with childhood trauma, resilience can mitigate the effects of trauma [56] and regulate the impact of negative life events on depression [57]. However, most previous studies have not explored the cumulative effect of childhood trauma on subjective well-being and the underlying mediating factors (both risk and protective) in university students.
In summary, the relationships between childhood trauma, depression, resilience, and subjective well-being are complex and may involve bidirectional causality [58]. With the global rise in common mental health issues among young people [59,60], childhood trauma emerges as a potential threat factor for adolescent depression, potentially leading to harmful lifelong effects on their development. As university students represent the future talent pool for national development, their psychological well-being is crucial. However, childhood trauma, like a time bomb hidden in some students’ minds, poses a potential threat to their psychological health. This study constructed a moderated mediation model (conceptual model depicted in Fig. 1) to examine whether subjective well-being mediates the relationship between childhood maltreatment and depression symptoms in university students, and whether psychological resilience moderates this mediated model. Specifically, drawing from the literature mentioned above, the following hypotheses were proposed: (1) Childhood trauma significantly predicts depression symptoms in university students; (2) Subjective well-being mediates the relationship between childhood trauma and depression symptoms in university students; (3) Resilience moderates the impact of childhood trauma and subjective well-being on depression symptoms.
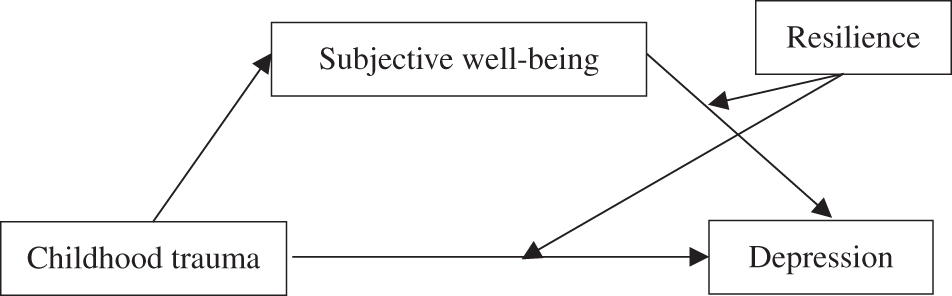
Figure 1: The proposed moderated mediation model.
This study focused on undergraduate students at a medical college in Kunming, Yunnan Province, China. All data were automatically collected using Questionnaire Star. The participants did not receive any incentive. Before collecting data, informed consent was obtained from all the university students. The principles of voluntary participation and confidentiality of the responses were emphasized. The study design was approved by Yunnan University of Chinese Medicine (IRB number: XXLW-2024-002) ethics review board.
The study employed convenience sampling, distributing a total of 367 questionnaires and obtaining 339 valid responses, resulting in a response rate of 92.4%. The participants’ ages ranged from 17 to 24 years old (mean age = 20.10 ± 1.90). Among them, there were 155 freshmen, 62 sophomores, 35 juniors, 22 seniors, and 65 fifth-year students. Regarding the participants’ backgrounds, 69 were from large or medium-sized cities (20.4%), while 270 were from rural areas or small towns (79.6%).
Childhood trauma questionnaire
The study utilized a shortened version of the Childhood Trauma Questionnaire (CTQ) developed by Bernstein et al. [61] and revised by Zhao et al. [62]. This version consists of 28 items, categorized into five dimensions: sexual trauma, emotional neglect, emotional trauma, physical neglect, and physical trauma. Responses were scored on a Likert 5-point scale (1–5). The questionnaire has been previously employed with Chinese participants and demonstrated good reliability and validity [63]. In the present study, the Cronbach’s α coefficient for this scale was calculated to be 0.853, indicating good internal consistency.
The subjective well-being Scale used in this study is the Index of well-being developed by Campbell et al. [64]. This scale is concise, user-friendly, and capable of reflecting the overall condition of subjective well-being. Comprising 9 items, questions 1 to 8 belong to the overall emotional index section, while question 9 pertains to the life satisfaction section [65]. The calculation method for subjective well-being is as follows: (average score of questions 1 to 8) + (score of question 9) × 1.1. The scale yields scores ranging from 2.1 to 14.7, with higher scores indicating stronger subjective well-being. In this study, the Cronbach’s α coefficient for this scale was determined to be 0.917, demonstrating robust internal consistency.
Center for epidemiologic studies depression
The Center for Epidemiologic Studies Depression Scale (CES-D), developed by Radloff et al., was employed in this study. This scale consists of 20 items, encompassing four factors: depression and positive emotions, interpersonal factors, as well as physical and activity-related symptoms. The total score on the scale ranges from 0 to 60, with a commonly used cutoff point of 16 to indicate a tendency toward depression—scores below 16 are considered normal, while scores equal to or greater than 16 suggest a tendency toward depression. Higher scores indicate more severe depressive symptoms. The CES-D has demonstrated good reliability and validity and is applicable to Chinese university students [66,67]. In this study, the Cronbach’s α coefficient for the scale was calculated to be 0.86, indicating strong internal consistency.
The Psychological Resilience Scale, revised by Singh et al. [68], was utilized in this study. This scale comprises three dimensions: resilience, fortitude, and optimism, totaling 25 items. Responses are scored on a 5-point Likert scale, where higher scores indicate a higher level of psychological resilience. The scale has demonstrated good reliability and validity in research involving domestic university student populations [69]. In this study, the Cronbach’s α coefficient for the scale was calculated to be 0.930, indicating excellent internal consistency.
The data collected in this study were analyzed using SPSS 26.0 and PROCESS 3.5. First, Harman’s one-way test was conducted to prevent potential common method bias. Next, descriptive statistics were examined, and correlation analyses were performed to explore the relationships between variables. Finally, Model 14 of the PROCESS macro was used to test the moderated mediation model of childhood trauma and college students’ depressive symptoms, followed by a simple slope analysis. To test the mediation and moderated mediation effects, a bias-corrected bootstrapping procedure (n = 5000) was applied, and 95% confidence intervals (CI) were calculated. Effects were considered significant when the confidence intervals did not contain zero. A threshold p-value of 0.05 was used to determine statistical significance.
The exploratory factor analysis of all items from the four questionnaires was conducted using Harman’s single-factor method. The results revealed 18 eigenvalues greater than 1, indicating the presence of common factors. The first common factor accounted for 24.93% of the total variance. Although this percentage falls below the critical threshold of 40%, suggesting that there is no severe issue of common method bias in this study.
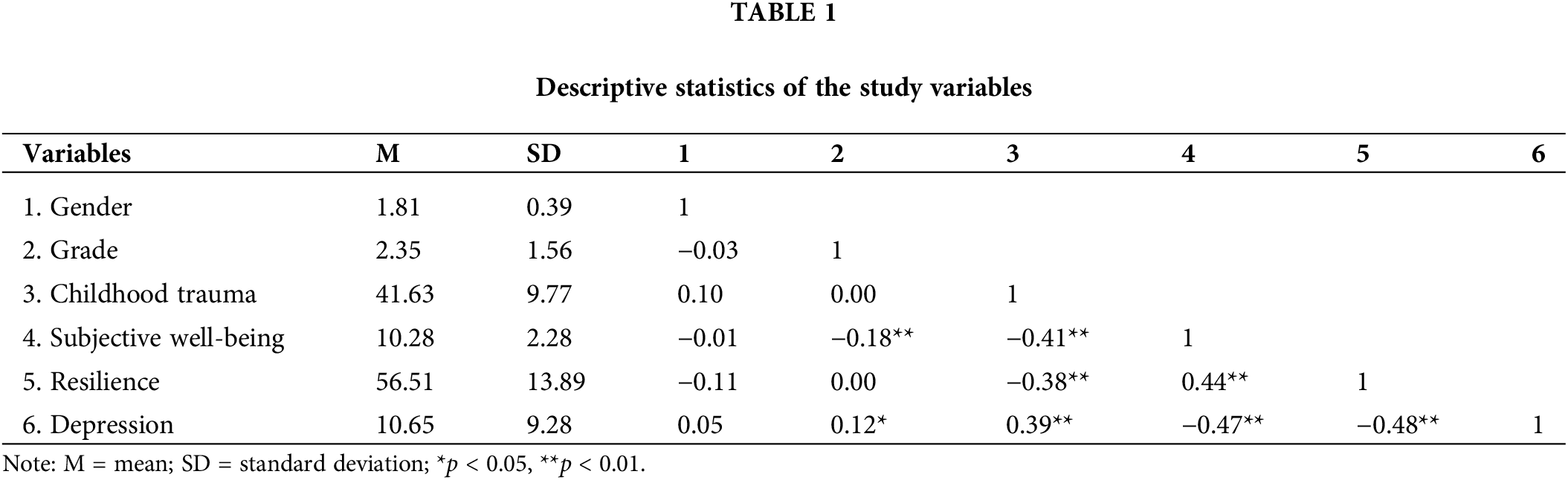
Descriptive statistical analysis
The mean values, standard deviations, and correlation coefficients among variables are presented in Table 1. The results indicate that Childhood Trauma is negatively correlated with subjective well-being and psychological resilience, while positively correlated with depression. Subjective well-being exhibits a positive correlation with psychological resilience and a negative correlation with depression. Psychological resilience is negatively correlated with depression. Furthermore, grade level was significantly correlated with subjective well-being and depression. Gender did not show significant correlations with the study variables. Therefore, grade level will be treated as a control variable in subsequent analyses.
Childhood trauma and depression: moderated mediation model
Utilizing Model 15 from the PROCESS macro, a simple mediation model was employed to examine the relationship among college students’ depressive symptoms (dependent variable), childhood trauma (independent variable), and subjective well-being (mediating variable). The results indicated that childhood trauma positively predicted depressive symptoms among college students (β = 0.37, p < 0.001, 95% CI: [0.28, 0.46]). Even after including subjective well-being in the regression equation, childhood trauma still significantly predicted depressive symptoms among college students (β = 0.19, p < 0.001, 95% CI: [0.09, 0.29]). Additionally, childhood trauma negatively predicted subjective well-being (β = −0.10, p < 0.001, 95% CI: [−0.12, −0.07]), and subjective well-being negatively predicted depressive symptoms among college students (β = −1.26, p < 0.001, 95% CI [−1.67, −0.85]). These findings suggest that subjective well-being partially mediates the relationship between childhood trauma and depressive symptoms among college students, with direct effects (effect size = 0.19) and mediating effects (effect size = 0.13) accounting for 60.13% and 39.87% of the total effect (effect size = 0.32), respectively. Refer to Fig. 2 for visualization.
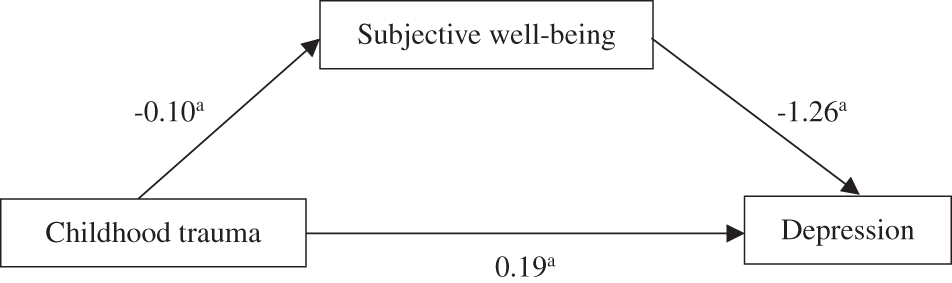
Figure 2: The mediating effect of subjective well-being on the relationship between childhood trauma and depression (ap < 0.01).
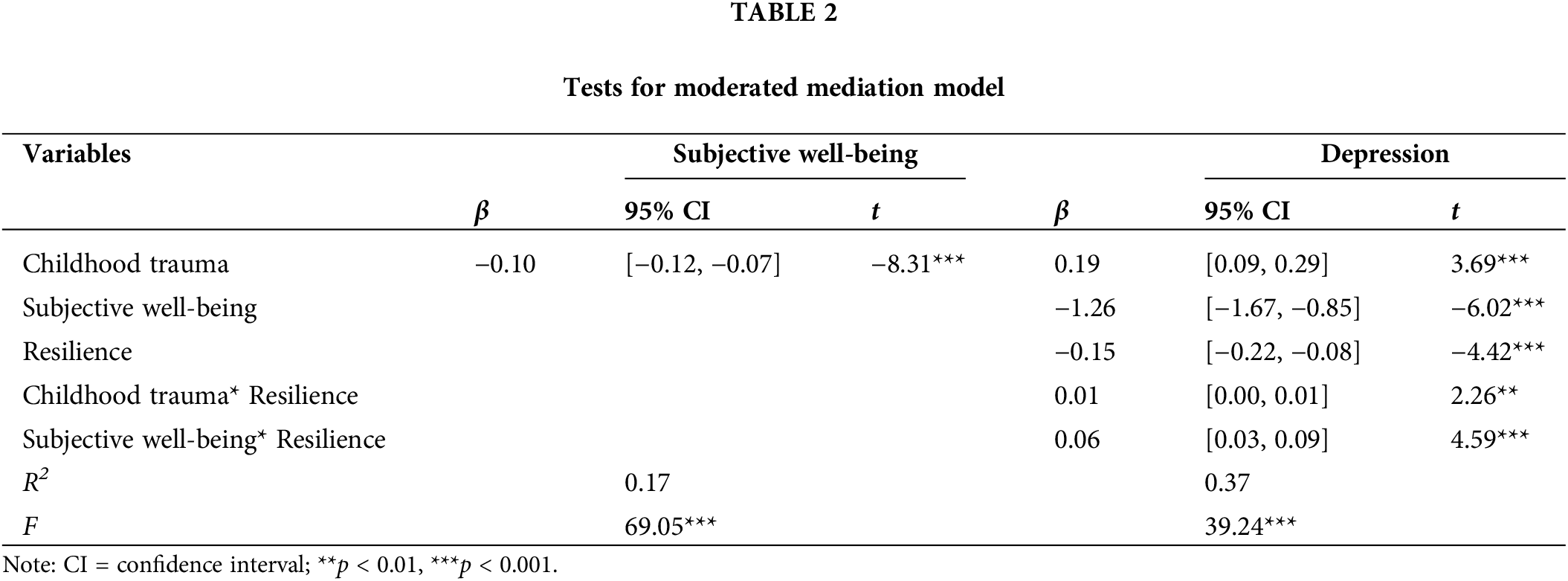
Using Model 15 from the PROCESS macro for analysis, with college students’ depressive symptoms as the dependent variable, childhood trauma as the independent variable, subjective well-being as the mediating variable, and psychological resilience as the moderating variable, the results revealed significant predictive effects of the interaction term between childhood trauma and psychological resilience (β = 0.01, p = 0.02, 95% CI [0.00, 0.01]), as well as the interaction term between subjective well-being and psychological resilience (β = 0.06, p < 0.001, 95% CI [0.03, 0.09]) on college students’ depressive symptoms. These findings suggest that psychological resilience moderates the relationship between childhood trauma and depressive symptoms among college students, as well as the relationship between subjective well-being and depressive symptoms among college students. Refer to Table 2 for details.
To elucidate how psychological resilience moderates the relationship between subjective well-being and depressive symptoms, simple slope tests were conducted by categorizing psychological resilience into high and low groups based on one standard deviation above and below the mean. Refer to Fig. 3 for visualization. The results revealed that when psychological resilience was relatively low, the negative predictive effect of subjective well-being on depressive symptoms was not significant (β = −0.38, p > 0.05, 95% CI [−0.89, 0.14]); however, when psychological resilience was relatively high, subjective well-being significantly negatively predicted depressive symptoms (β = −2.02, p < 0.001, 95% CI [−2.58, −1.46]). This suggests that as individual psychological resilience increases, the predictive effect of subjective well-being on depressive symptoms gradually increases.
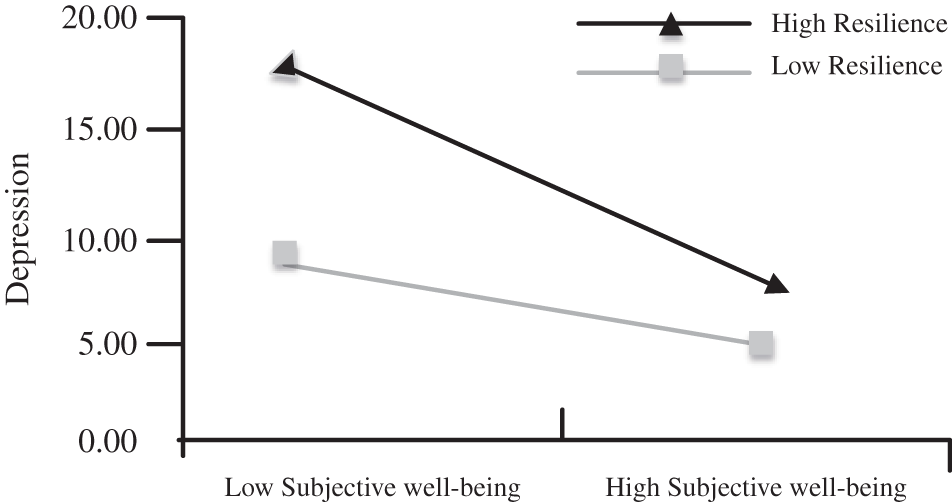
Figure 3: The moderating effect of mental resilience on subjective well-being and depression.
To further elucidate how psychological resilience moderates the relationship between childhood maltreatment and depressive symptoms, simple slope tests were conducted by categorizing psychological resilience into high and low groups based on one standard deviation above and below the mean. Refer to Fig. 4 for visualization. The results indicated that when psychological resilience was relatively low, childhood trauma did not significantly predict depressive symptoms (β = 0.09, p > 0.05, 95% CI [−0.01, 0.19]); however, when psychological resilience was relatively high, childhood trauma significantly predicted depressive symptoms positively (β = 0.30, p < 0.001, 95% CI [0.13, 0.46]). This suggests that as individual psychological resilience increases, the predictive effect of childhood maltreatment on depressive symptoms shows a gradual decrease.
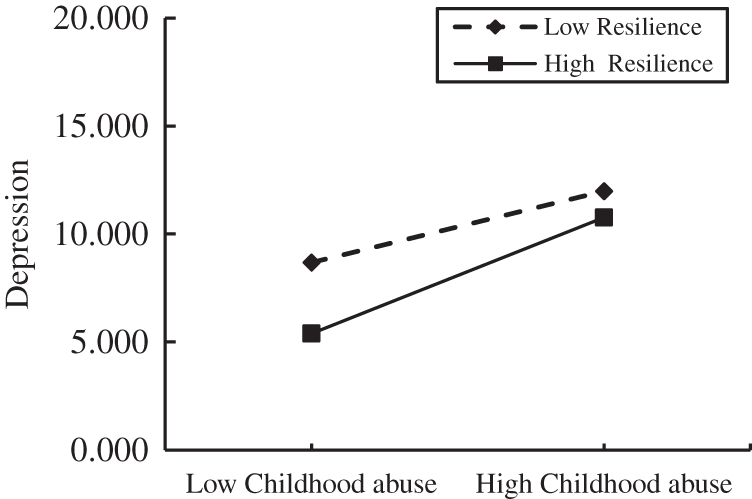
Figure 4: The moderating effect of mental resilience on childhood trauma and depression.
The association between childhood trauma and depressive symptoms
The research findings reveal that childhood trauma significantly and positively predicts depressive symptoms in college students, aligning with previous study outcomes [70]. This may be attributed to the heightened sensitivity of brain circuits involved in stress and emotional regulation (such as the hypothalamic-pituitary-adrenal axis, amygdala, and hippocampus) during active brain development in childhood [71]. The potential neurobiological effects of these adverse experiences and prolonged toxic stress make individuals highly sensitive, vigilant, and prone to exaggerated responses to threatening stimuli later in life [72]. Childhood trauma not only alters the neurobiological systems but also disrupts other epigenetic and socio-psychological stress pathways, leading to lowered stress thresholds and compromised coping mechanisms [73], thereby increasing the risk of developing depression. Individuals with adverse experiences in childhood may encounter challenges in regulating emotions and establishing positive interpersonal relationships, significantly impacting their mental well-being [74]. Additionally, based on the positive psychology perspective on depression, this study introduces subjective well-being and psychological resilience to further explore the impact of childhood trauma on depressive symptoms in college students. The research outcomes hold crucial implications for guiding interventions aimed at improving the mental health levels of college students.
Childhood trauma experiences can lead to the development of negative cognitive styles, thereby triggering depression. Research by Rose et al., among others, also suggests that childhood trauma may contribute to the development of negative cognitive styles [75]. Childhood neglect often results in a lack of confidence and feelings of insecurity in children, making them susceptible to cognitive distortions and negative self-beliefs, thereby increasing the risk of developing depressive symptoms. Therefore, in the context of school mental health education, it is crucial to pay special attention to individuals who have experienced childhood trauma, as the negative schema as formed during their development make them more vulnerable to the effects of traumatic experiences. Additionally, for those students who have suffered from childhood maltreatment, leading to heightened depressive symptoms and a lack of self-healing abilities, schools should, under the premise of ensuring their safety, provide psychological counseling services, mental health education courses, and psychological support groups to help them alleviate their emotions and reduce depressive symptoms.
The mediating role of subjective well-being
Children grow through interactions with their surrounding environment, and adverse experiences during childhood can have profound and lasting effects on their psychological development throughout life [76]. They may be prone to experiencing more pessimistic and anxious negative emotions, with a higher likelihood of developing depressive symptoms [77]. The results of the mediating analysis indicate that subjective well-being plays a mediating role between childhood trauma and depressive symptoms in college students. Subjective well-being significantly negatively predicts depressive symptoms, and enhancing subjective well-being contributes to a reduction in the occurrence of depressive symptoms, aligning with the explanation from positive psychology [78]. Research has found that positive psychological interventions effectively enhance subjective well-being [79]. Subjective well-being, as a crucial assessment indicator, decreasingly correlates with the occurrence of depression [80]. The reason childhood trauma can impact the occurrence of depressive symptoms in college students through subjective well-being is that individuals with a history of childhood trauma may reduce their subjective well-being through early-onset depression and other health-harming behaviors [81]. Subjective well-being as a significant positive emotional state, is associated with increased individual positive resources and serves as a protective factor in reducing the incidence of depression [82].
Positive psychology posits that depression arises not merely as a consequence of negative cognition but rather due to a lack of positive resources. Children who have experienced trauma may struggle to form a sense of psychological safety, leading to a decrease in subjective well-being. As a crucial positive resource, low levels of subjective well-being contribute to the onset of depression [83]. Therefore, this study posits that enhancing the subjective well-being of college students can reduce the occurrence and progression of depression. Universities can incorporate courses in mental health education, focusing on emotional regulation, stress management, and the cultivation of positive mindsets, to help students enhance their awareness of mental health and develop relevant skills. Additionally, fostering the establishment of robust social support networks among students, including interactions with peers, educators, and family members, as well as engagement in extracurricular activities and volunteering, is imperative. Furthermore, encouraging students to maintain regular sleep patterns, healthy dietary habits, and moderate exercise routines is essential for promoting a balanced mind-body health equilibrium. Finally, providing opportunities for students to participate in diverse activities to cultivate their interests, skills, and potentials can enhance their self-esteem and sense of fulfillment.
The discovery of this mediating mechanism, exploring the developmental process through which childhood trauma influences the occurrence of depressive symptoms via subjective well-being from a positive psychology perspective, provides theoretical support.
The regulatory role of psychological resilience
The results of this study reveal a significant moderating effect of psychological resilience on the pathway from childhood trauma to subjective well-being to depressive symptoms. Specifically, the interactive effect between subjective well-being and psychological resilience significantly predicts depressive symptoms. The path process from subjective well-being to depressive symptoms is influenced by the moderation of psychological resilience, showing a gradual increase in the predictive effect of subjective well-being on depressive symptoms with an elevation in psychological resilience levels. There is a negative correlation between psychological resilience and both childhood trauma and depressive symptoms, while a positive correlation exists between psychological resilience and subjective well-being. These findings align with previous research conclusions, highlighting the role of psychological resilience in enhancing happiness and reducing depressive symptoms through positive emotions and cognitive reappraisal [84,85]. Numerous studies confirm that individuals with higher levels of psychological resilience demonstrate greater resilience in the face of adversity, employing a positive mindset to cope with stress and crises, enabling them to adeptly handle life’s challenges [86,87].
Psychological resilience as a relatively stable yet cultivable trait, can be enhanced through targeted educational campaigns, psychological counseling activities, and initiatives such as offering specialized courses on resilience and organizing student support groups. These efforts aim to elevate students’ levels of psychological resilience. Furthermore, research findings indicate that metacognitive intervention techniques are efficient and stable in enhancing resilience. Metacognitive intervention can continuously reinforce individuals’ positive emotions, allowing their psychological state to enter a virtuous cycle. Through continuous reinforcement and consolidation in daily life, individuals can become more optimistic and confident, thereby significantly enhancing their psychological resilience [88].
Childhood is the most distinctive developmental stage in one’s life. For children who have experienced childhood trauma, they lack the ability to choose their birth and upbringing environment and cannot alter their family of origin or parents’ parenting styles. However, it is essential to recognize that individuals in such circumstances are not limited to a path of self-destruction. This study, grounded in positive psychology, offers a novel perspective on inhibiting the occurrence and development of depression in college students. Childhood trauma can positively predict depressive symptoms in college students, and this prediction can also occur indirectly through the mediating role of subjective well-being. This implies that subjective well-being is a crucial factor influencing depressive symptoms in college students. Therefore, effectively enhancing the level of subjective well-being in college students can contribute to reducing depressive symptoms. While childhood trauma is an unchangeable factor, subjective well-being, as a cognitive and emotional element, can be improved through self-regulation or external interventions (such as implementing altruistic behaviors, expressing gratitude, and setting personal goals) to modify the occurrence and development of depressive symptoms in college students. Future research could explore positive psychological intervention techniques to address depression issues in college students at the source.
Limitations and Future Research Implications
There are also some limitations in this study, which need to be improved upon in future research. First, this study was cross-sectional by design, so the results of the study cannot extrapolate causality. Future research should employ longitudinal designs or experimental methods and utilize data analysis approaches such as correlation design with intercross-lag group or hierarchical linear models to further investigate the causal relationship between childhood trauma and depression. Second, this study is a retrospective survey research, and it is important to acknowledge the potential presence of recall bias among students during the questionnaire completion process. Participants may experience memory biases, and there is a possibility of information bias, especially in relation to sensitive items. Finally, the limited sample size of our study, comprising solely Chinese college students, limits the cross-cultural validity of our findings. Therefore, future research should replicate the study using a more diverse and expansive sample.
Childhood trauma significantly and positively predicts depressive symptoms in college students. Moreover, it can directly predict depressive symptoms through the mediating effect of subjective well-being. Enhancing psychological resilience and levels of subjective well-being in college students can reduce depressive symptoms and promote psychological well-being. This research, approached from the perspective of positive psychology, offers a novel outlook for the prevention and intervention of depressive symptoms in college students.
Acknowledgement: We would like to express our sincere gratitude to the respondents for their time to complete the survey.
Funding Statement: Yunnan Provincial Department of Education Science Research Fund (2024J0412).
Author Contributions: The authors confirm their contribution to the paper as follows: study conception and design: Fuhua Yang, Keli Yin; data collection: Fuhua Yang, Rong Chen, Maoying Cui; analysis and interpretation of results: Jiaci Lin, Chunlin Gao; draft manuscript preparation: Fuhua Yang, Jiaci Lin, Keli Yin. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: Due to institutional ethical specifications, the data used in this study is not publicly available. On reasonable request, data will be made available by the corresponding author.
Ethics Approval: Before collecting data, informed consent was obtained from all the university students. The principles of voluntary participation and confidentiality of the responses were emphasized. The study design was approved by Yunnan University of Chinese Medicine (IRB number: XXLW-2024-002) Ethics Review Board.
Conflicts of Interest: This study was carried in the absence of any personal, professional, or financial relationships that could potentially be constructed as a conflict of interest.
References
1. Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. The Lancet Psychiat. 2019;6(3):211–24. doi:10.1016/S2215-0366(18)30511-X. [Google Scholar] [PubMed] [CrossRef]
2. Mokdad AH, Forouzanfar MH, Daoud F, Mokdad AA, El Bcheraoui C, Moradi-Lakeh M, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet. 2016;387(10036):2383–401. doi:10.1016/S0140-6736(16)00648-6. [Google Scholar] [PubMed] [CrossRef]
3. Malhi GS, Mann JJ. Depression. The Lancet. 2018;392(10161):2299–312. doi:10.1016/S0140-6736(18)31948-2. [Google Scholar] [PubMed] [CrossRef]
4. Greenberg PE, Fournier A-A, Sisitsky T, Pike CT, Kessler RC. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatr. 2015;76(2):155–62. doi:10.4088/JCP.14m09298. [Google Scholar] [PubMed] [CrossRef]
5. Wang MY, Han FF, Liu J, Huang KS, Peng HY, Huang MT, et al. Meta-analysis of the detection rate of depressive symptoms and related factors in college students. Chin J Ment Health. 2020;34(12):1041–7 (In Chinese). [Google Scholar]
6. Zhang R, Yang C, Zhang Y. Meta-analysis of factors influencing depression in Chinese university students. Chin Gen Pract. 2020;23(35):4497–502 (In Chinese). [Google Scholar]
7. Kpolou CKK, Jumageldinov A, Park S, Nieuviarts N, Cénat JM. Prevalence of depressive symptoms and associated psychosocial risk factors among university students: the moderating and mediating effects of resilience. Psychiatr Q. 2020;92(2):443–57. doi:10.1007/s11126-020-09812-8. [Google Scholar] [PubMed] [CrossRef]
8. Ridner SL, Newton KS, Staten RR, Crawford TN, Hall LA. Predictors of well-being among college students. J Am Coll Health. 2016;64(2):116–24. doi:10.1080/07448481.2015.1085057. [Google Scholar] [PubMed] [CrossRef]
9. Zhao Y, Wang YQ, Wang J, Jiang MM, Wang J, Jin YL. Current situation and correlation analysis of self-harm behaviors, depression, and anxiety in college students. Chin J Sch Health. 2021;42:92–95 (In Chinese). [Google Scholar]
10. Griggs S. Hope and mental health in young adult college students: an integrative review. J Psychosoc Nurs Ment Health Serv. 2017;55(2):28. doi:10.3928/02793695-20170210-04. [Google Scholar] [PubMed] [CrossRef]
11. Zheng X, Wu S, Liu L. The relationship between optimism and depression among college students: the chain-mediated effect of negative cognitive bias and negative emotions. Psychol Explor. 2024;44:66–73 (In Chinese). [Google Scholar]
12. Wang MY, Liu J, Wu X, Li L, Hao XD, Shen Q, et al. Meta-analysis of the prevalence of depression among Chinese college students in the past decade. J Hainan Med Univ. 2020;26:686–693 (In Chinese). [Google Scholar]
13. Fu X, Zhang K, Chen X. China national mental health development report 2021. Beijing, China: Social Sciences Academic Press; (2019–2020) (In Chinese). [Google Scholar]
14. Tang H, Ding LL, Song XL, Haung ZW, Qi Q, He LP, et al. Meta-analysis of the detection rate of depression among Chinese college students from 2002 to 2011. J Jilin Univ (Medicine Edition). 2013;39(5):965–9 (In Chinese). [Google Scholar]
15. Hu Y, Liu Z. Intervention study on the psychological health of depressed college students: differential effects of support from different types of schools. J Hunan Normal Univ (Educ Sci). 2019;18(5):120–5 (In Chinese). [Google Scholar]
16. Lei H, Zhu T, Yang Y, Zhang X. The relationship between childhood trauma and depression in adolescents: the longitudinal mediating role of insecure attachment. Chin J Clin Psychol. 2024;32(1):71–5 (In Chinese). [Google Scholar]
17. Ding HS, Han J, Zhang ML, Wang KQ, Gong JL, Yang SB. Moderating and mediating effects of resilience between childhood trauma and depressive symptoms in Chinese children. J Affect Disord. 2017;211:130–5. doi:10.1016/j.jad.2016.12.056. [Google Scholar] [PubMed] [CrossRef]
18. Wang J, He X, Chen Y, Lin C. Association between childhood trauma and depression: a moderated mediation analysis among normative Chinese college students. J Affect Disord. 2020;276:519–24. doi:10.1016/j.jad.2020.07.051. [Google Scholar] [PubMed] [CrossRef]
19. Li M, D’Arcy C, Meng X. Maltreatment in childhood substantially increases the risk of adult depression and anxiety in prospective cohort studies: systematic review, meta-analysis, and proportional attributable fractions. Psychol Med. 2016;46(4):717–30. doi:10.1017/S0033291715002743. [Google Scholar] [PubMed] [CrossRef]
20. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. 2019;56(6):774–86. doi:10.1016/j.amepre.2019.04.001. [Google Scholar] [PubMed] [CrossRef]
21. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. the cost of child maltreatment: who pays? Am J Prev Med. 1998;14(4):53–69. doi:10.1186/1471. [Google Scholar] [CrossRef]
22. Batten SV, Aslan M, Maciejewski PK, Mazure CM. Childhood maltreatment as a risk factor for adult cardiovascular disease and depression. J Clin Psychiatr. 2004;65(2):249–54. doi:10.4088/JCP.v65n0217. [Google Scholar] [PubMed] [CrossRef]
23. Nanni V, Uher R, Danese A. Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: a meta-analysis. Am J Psychiatr. 2012;169(2):141–51. doi:10.1176/appi.ajp.2011.11020335. [Google Scholar] [PubMed] [CrossRef]
24. Daruy-Filho L, Brietzke E, Lafer B, Grassi-Oliveira R. Childhood maltreatment and clinical outcomes of bipolar disorder. Acta Psychiatr Scand. 2011;124(6):427–34. doi:10.1111/j.1600-0447.2011.01756.x. [Google Scholar] [PubMed] [CrossRef]
25. Fisher HL, Hosang GM. Childhood maltreatment and bipolar disorder: a critical review of the evidence. Mind & Brain. 2010;1(1):75–85. [Google Scholar]
26. Bruce LC, Heimberg RG, Blanco C, Schneier FR, Liebowitz MR. Childhood maltreatment and social anxiety disorder: implications for symptom severity and response to pharmacotherapy. Depress Anxiety. 2012;29(2):132–9. doi:10.1002/da.20909. [Google Scholar] [PubMed] [CrossRef]
27. Simon NM, Herlands NN, Marks EH, Mancini C, Stein MB. Childhood maltreatment linked to greater symptom severity and poorer quality of life and function in social anxiety disorder. Depress Anxiety. 2010;26(11):1027–32. doi:10.1002/da.20604. [Google Scholar] [PubMed] [CrossRef]
28. Brown J, Cohen P, Johnson JG, Salzinger S. A longitudinal analysis of risk factors for child maltreatment: findings of a 17-year prospective study of officially recorded and self-reported child abuse and neglect. Child Abuse & Negl. 1998;22(11):1065–78. doi:10.1016/S0145-2134(98)00087-8. [Google Scholar] [PubMed] [CrossRef]
29. Downs WR, Harrison L. Childhood maltreatment and the risk of substance problems in later life. Health Soc Care Community. 1998;6(1):35–46. doi:10.1007/978-3-319-02591-9_11. [Google Scholar] [CrossRef]
30. Young-Wolff KC, Kendler KS, Prescott CA. Interactive effects of childhood maltreatment and recent stressful life events on alcohol consumption in adulthood. J Stud Alcohol Drugs. 2012;73(4):559–69. doi:10.1111/j.1465-3362.2012.00462.x. [Google Scholar] [CrossRef]
31. Schulz A, Becker M, Van der Auwera S, Barnow S, Appel K, Mahler J, et al. The impact of childhood trauma on depression: does resilience matter? Population-based results from the study of health in Pomerania. J Psychosom Res. 2014;77(2):97–103. doi:10.1016/j.jpsychores.2014.06.008. [Google Scholar] [PubMed] [CrossRef]
32. Pompili M, Innamorati M, Lamis DA, Erbuto D, Venturini P, Ricci F, et al. The associations among childhood maltreatment, male depression and suicide risk in psychiatric patients. Psychiatry Res. 2014;220(1–2):571–8. doi:10.1016/j.psychres.2014.07.056. [Google Scholar] [PubMed] [CrossRef]
33. Blum RW, Li M, Naranjo-Rivera G. Measuring adverse child experiences among young adolescents globally: relationships with depressive symptoms and violence perpetration. J Adolesc Health. 2019;65(1):86–93. doi:10.1016/j.jadohealth.2019.01.020. [Google Scholar] [PubMed] [CrossRef]
34. Reffi AN, Boykin DM, Orcutt HK. Examining pathways of childhood maltreatment and emotional dysregulation using self-compassion. J Aggress, Maltreatment Trauma. 2019;28(10):1269–85. doi:10.1080/10926771.2018.1485810. [Google Scholar] [CrossRef]
35. Christ C, de Waal MM, Dekker JJM, van Kuijk I, van Schaik DJF, Kikkert MJ, et al. Linking childhood emotional abuse and depressive symptoms: the role of emotion dysregulation and interpersonal problems. PLoS One. 2019;14(2):e0211882. doi:10.1371/journal.pone.0211882. [Google Scholar] [PubMed] [CrossRef]
36. Song C, Yao L, Chen H, Zhang J, Liu L. The relationship between adverse childhood experiences and depressive symptoms in rural left-behind adolescents: a cross-sectional survey. Heliyon. 2024;10(4):e26587. doi:10.1016/j.heliyon.2024.e26587. [Google Scholar] [PubMed] [CrossRef]
37. Capretto JJ, Capretto JJ. Developmental timing of childhood physical and sexual maltreatment predicts adult depression and post-traumatic stress symptoms. J Interpers Violence. 2020;35(13–14):2558–82. doi:10.1177/0886260517704963. [Google Scholar] [PubMed] [CrossRef]
38. Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: three decades of progress. Am Psychol Assoc. 1999;125(2):276–302. doi:10.1037/0033-2909.125.2.276. [Google Scholar] [CrossRef]
39. Aghababaei N, Arji A. Well-being and the hexaco model of personality. Pers Individ Differ. 2014;56(4):139–42. doi:10.1016/j.paid.2013.08.037. [Google Scholar] [CrossRef]
40. Palomar-Lever J, Victorio-Estrada A. Determinants of subjective well-being in adolescent children of recipients of the oportunidades human development program in Mexico. Soc Indic Res. 2014;118(1):103–24. doi:10.1007/s11205-013-0407-7. [Google Scholar] [CrossRef]
41. Corcoran M, McNulty M. Examining the role of attachment in the relationship between childhood adversity, psychological distress and subjective well-being. Child Abuse & Neglect. 2017;76(6):297–309. doi:10.1016/j.chiabu.2017.11.012. [Google Scholar] [PubMed] [CrossRef]
42. Zhang LY. The influence of depression and social support on subjective well-being among normal university students. Chin J Health Psychol. 2006;(5):595–7(In Chinese). doi:10.13342/j.cnki.cjhp.2006.05.050. [Google Scholar] [CrossRef]
43. Diener E, Scollon CN, Lucas RE. The evolving concept of subjective well-being: the multifaceted nature of happiness. Adv Cell Aging Gerontol. 2003;15(4):187–219. doi:10.1016/S1566-3124(03)15007-9. [Google Scholar] [CrossRef]
44. Fingerman KL. Psychosocial resources and associations between childhood physical abuse and adult well-being. J Gerontol. 2010;65(4):425–33. doi:10.1093/geronb/gbq031. [Google Scholar] [PubMed] [CrossRef]
45. Greger HK, Myhre AK, Klöckner CA, Jozefiak T. Childhood maltreatment, psychopathology and well-being: the mediator role of global self-esteem, attachment difficulties and substance use. Child Abuse Negl. 2017;70(1):122–33. doi:10.1016/j.chiabu.2017.06.012. [Google Scholar] [PubMed] [CrossRef]
46. Oshio T, Umeda M, Kawakami N. Childhood adversity and adulthood subjective wellbeing: evidence from Japan. J Happiness Stud. 2013;14(3):843–60. doi:10.1007/s10902-012-9358-y. [Google Scholar] [CrossRef]
47. Payne JD, Jackson ED, Hoscheidt S, Ryan L, Jacobs WJ, Nadel L. Stress administered prior to encoding impairs neutral but enhances emotional long-term episodic memories. Learn Mem. 2007;14(12):861–8. doi:10.1101/lm.743507. [Google Scholar] [PubMed] [CrossRef]
48. Sheikh MA, Abelsen B, Olsen JA. Differential recall bias, intermediate confounding, and mediation analysis in life course epidemiology: an analytic framework with empirical example. Front Psychol. 2016;7:1828. doi:10.3389/fpsyg.2016.01828. [Google Scholar] [PubMed] [CrossRef]
49. Werner EE. Risk, resilience, and recovery: perspectives from the Kauai Longitudinal Study. Dev Psychopathol. 1993;5(4):503–15. doi:10.1017/S095457940000612X. [Google Scholar] [CrossRef]
50. Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113. [Google Scholar] [PubMed] [CrossRef]
51. Nadia A, Sarah T, Stefan P. Conceptualizing resilience in adult mental health literature: a systematic review and narrative synthesis. Psychol Psychothe. 2019;92(3):299–341. doi:10.1111/papt.12185. [Google Scholar] [PubMed] [CrossRef]
52. Denckla CA, Cicchetti D, Kubzansky LD, Seedat S, Teicher MH, Williams DR, et al. Psychological resilience: an update on definitions, a critical appraisal, and research recommendations. Eur J Psychotraumatol. 2020;11(1):1–11. doi:10.1080/20008198.2020.1822064. [Google Scholar] [PubMed] [CrossRef]
53. Zautra AJ, Arewasikporn A, Davis MC. Resilience: promoting well-being through recovery, sustainability, and growth. Res Hum Dev. 2010;7(3):221–38. doi:10.1080/15427609.2010.504431. [Google Scholar] [CrossRef]
54. Troy AS, Mauss IB. Resilience in the face of stress: emotion regulation as a protective factor. In: Resilience and mental health: Challenges across the lifespan. Cambridge University Press. 2011. vol. 1, no. 2, p. 30–44. doi:10.1017/CBO9780511994791. [Google Scholar] [CrossRef]
55. Meng X, Fleury MJ, Xiang YT, Li M, D’Arcy C. Resilience and protective factors among people with a history of child maltreatment: a systematic review. Soc Psychiatry Psychiatr Epidemiol. 2018;53(5):453–75. doi:10.1007/s00127-018-1485-2. [Google Scholar] [PubMed] [CrossRef]
56. Roy A, Carli V, Sarchiapone M. Resilience mitigates the suicide risk associated with childhood trauma. J Affect Disord. 2011;133(3):591–4. doi:10.1016/j.jad.2011.05.006. [Google Scholar] [PubMed] [CrossRef]
57. Zhu Q, Guo HY, Pan J, Yang DH. Perceived discrimination and behavior problems in migrant children: the moderating role of psychological resilience. Chin J Clin Psychol. 2015;23(3):529–33 (In Chinese). [Google Scholar]
58. Diener E, Pressman SD, Hunter J, Delgadillo-Chase D. If, why, and when subjective well-being influences health, and future needed research. Appl Psychol: Health Well. 2017;9(2):133–67. doi:10.1111/aphw.12090. [Google Scholar] [PubMed] [CrossRef]
59. Eisenberg D, Lipson SK, Posselt J. Promoting resilience, retention, and mental health. New Dir Stud Serv. 2016;2016(156):87–95. doi:10.1002/ss.20194. [Google Scholar] [CrossRef]
60. Evans-Lacko S, Thornicroft G. Viewpoint: WHO world mental health surveys international college student initiative: implementation issues in low- and middle-income countries. Int J Methods Psychiatr Res. 2019;28(2):e1756. doi:10.1002/mpr.1756. [Google Scholar] [PubMed] [CrossRef]
61. Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse & Neglect. 2003;27(2):169–90. doi:10.1016/s0145-2134(02)00541-0. [Google Scholar] [PubMed] [CrossRef]
62. Zhao XF, Zhang YL, Li LF, Zhou YF, Li HZ, Yang SC. Reliability and validity of the Chinese version of childhood trauma questionnaire. Chin J Clin Rehabil. 2005;9(20):105–7 (In Chinese). [Google Scholar]
63. Zeng ZH, Peng LY, Zhan L, Liu SJ, Ouyang XY, Ding DQ, et al. The impact of childhood abuse on depression symptoms in college students: The mediating role of subjective well-being and the moderating effect of genetics. Psychol Dev Edu. 2023;39:276–85 (In Chinese). [Google Scholar]
64. Campbell A, Converse PE, Rodgers WL. The quality of american life: perceptions, evaluations and satisfactions. New York: Russell Sage Foundation; 1976. vol. 10, p. 583. [Google Scholar]
65. Wang X, Ma H. Handbook of the mental health assessment scale. Beijing: Chinese Association for Mental Health; 1996 (In Chinese). [Google Scholar]
66. Chen Z, Yang X, Li X. Application of the depression scale in the epidemiological survey center among chinese adolescents. Chin J Clin Psychol. 2009;17:443–8 (In Chinese). [Google Scholar]
67. Yang WH, Xiong G, Garrido LE, Zhang JX, Wang MC, Wang C. Factor structure and criterion validity across the full scale and ten short forms of the CES-D among chinese adolescents. Psychol Assess. 2018;30(9):1186–98. doi:10.1037/pas0000559. [Google Scholar] [PubMed] [CrossRef]
68. Singh K, Yu XN. Psychometric evaluation of the connor-davidson resilience scale (CD-RISC) in a sample of indian students. J Psychol. 2010;1(1):23–30. doi:10.1080/09764224.2010.11885442. [Google Scholar] [CrossRef]
69. Hu A, Gao X. Impact of ADHD symptoms on quality of life in female college students: the chain mediating role of self-esteem and psychological resilience. Chin J Clin Psychol. 2020;28:829–33 (In Chinese). [Google Scholar]
70. Li M, Liu S, D’Arcy C, Gao T, Meng X. Interactions of childhood maltreatment and genetic variations in adult depression: a systematic review. J Affect Disord. 2020;276(1):19–36. doi:10.1016/j.jad.2020.06.055. [Google Scholar] [PubMed] [CrossRef]
71. Herzog JI, Schmahl C. Adverse childhood experiences and the consequences on neurobiological, psychosocial, and somatic conditions across the lifespan. Front Psychiatr. 2018;9(1):420. doi:10.3389/fpsyt.2018.00420. [Google Scholar] [PubMed] [CrossRef]
72. Teicher MH, Samson JA, Anderson CM, Ohashi K. The effects of childhood maltreatment on brain structure, function and connectivity. Nat Rev Neurosci. 2016;17(10):652–66. doi:10.1038/nrn.2016.111. [Google Scholar] [PubMed] [CrossRef]
73. Nurius PS, Green S, Logan-Greene P, Borja S. Life course pathways of adverse childhood experiences toward adult psychological well-being: a stress process analysis. Child Abuse Negl. 2015;45(6):143–53. doi:10.1016/j.chiabu.2015.03.008. [Google Scholar] [PubMed] [CrossRef]
74. Mc Elroy S, Hevey D. Relationship between adverse early experiences, stressors, psychosocial resources and wellbeing. Child Abuse Negl. 2014;38(1):65–75. doi:10.1016/j.chiabu.2013.07.017. [Google Scholar] [PubMed] [CrossRef]
75. Rose DT, Abramson LY. Developmental predictors of depressive cognitive style: research and theory. In: Rochester Symposium of Developmental Psychopathology, 1992; Rochester, NY: University of Rochester Press. [Google Scholar]
76. Kim SC, Gostin LO, Cole TB. Child abuse reporting: rethinking child protection. JAMA. 2012;308(1):37–8. doi:10.1001/jama.2012.6414. [Google Scholar] [PubMed] [CrossRef]
77. Song XB, Wang SS, Wang R, Xu HQ, Jiang ZC, Li SQ, et al. Mediating effects of specific types of coping styles on the relationship between childhood maltreatment and depressive symptoms among chinese undergraduates: the role of sex. Int J Environ Res Public Health. 2020;17(9):958–60. doi:10.3390/ijerph17093120. [Google Scholar] [PubMed] [CrossRef]
78. Tomyn AJ, Weinberg MK, Cummins RA. Intervention efficacy among ‘at risk’ adolescents: a test of subjective wellbeing homeostasis theory. Soc Indic Res. 2015;120(3):883–95. doi:10.1007/s11205-014-0619-5. [Google Scholar] [CrossRef]
79. Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F, Bohlmeijer E. Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health. 2013;13(1):119. doi:10.1186/1471-2458-13-119. [Google Scholar] [PubMed] [CrossRef]
80. Seligman ME, Seligman MEP. Positive health. Appl Psychol. 2008;57(s1):3–18. doi:10.1111/j.1464-0597.2008.00351.x. [Google Scholar] [CrossRef]
81. Giovanelli A, Reynolds AJ, Mondi CF, Ou SR. Adverse childhood experiences and adult well-being in a low-income, urban cohort. Pediatrics. 2016;137(4):e20154016. doi:10.1542/peds.2015-4016. [Google Scholar] [PubMed] [CrossRef]
82. Moreno RL, Godoy-Izquierdo D, Vázquez Pérez ML, García AP, Araque Serrano F, Godoy García JF. Multidimensional psychosocial profiles in the elderly and happiness: a cluster-based identification. Aging Ment Health. 2014;18(4):489–503. doi:10.1080/13607863.2013.856861. [Google Scholar] [PubMed] [CrossRef]
83. Seligman MEP, Steen TA, Park N, Peterson C. Positive psychology progress: empirical validation of interventions. Am Psychol. 2005;60(5):410–21. doi:10.1037/0003-066X.60.5.410. [Google Scholar] [PubMed] [CrossRef]
84. Mehta MH, Grover RL, Didonato TE, Kirkhart MW, Examining the positive cognitive triad: a link between resilience and well-being. Los Angeles: SAGE Publications Sage CA; 2019. vol. 22, p. 776–88. doi:10.1177/0033294118773722. [Google Scholar] [CrossRef]
85. Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health. 2017;2(8):e356–66. doi:10.1016/S2468-2667(17)30118-4. [Google Scholar] [PubMed] [CrossRef]
86. Werner E. Risk, resilience, and recovery. Reclaiming Children & Youth. 2012;21(1):18–23. doi:10.1057/978-1-137-52577-2_13. [Google Scholar] [CrossRef]
87. Luthar SS, Crossman EJ, Small PJ. Resilience and adversity. In: Handbook of child psychology and developmental science; 2015. vol. 7, no. 3, p. 247–86. doi:10.1002/9781118963418.childpsy307. [Google Scholar] [CrossRef]
88. Yan KJ. The intervention effect of metacognitive intervention techniques on psychological resilience in college students. China: Liaoning Normal University; 2019 (In Chinese). [Google Scholar]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools