
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Linking Perceived Risk of Public Health Emergency to Psychological Distress among Chinese College Students: The Chain Mediation Role of Balanced Time Perspective and Negative Coping Styles
1 School of Education Science, Nanjing Normal University, Nanjing, 210024, China
2 Center of Clinical Psychology, The Third People’s Hospital of Heze City, Heze, 274031, China
3 School of Education Science, Northwest Normal University, Lanzhou, 730070, China
4 Mental Health Center, Hubei Polytechnic University, Huangshi, 435003, China
5 College of Teacher Education, Zhejiang Normal University, Jinhua, 321004, China
* Corresponding Author: Biru Chang. Email:
(This article belongs to the Special Issue: Social Stress, Adversity, and Mental Health in Transitional China)
International Journal of Mental Health Promotion 2024, 26(8), 599-610. https://doi.org/10.32604/ijmhp.2024.050302
Received 01 February 2024; Accepted 18 July 2024; Issue published 30 August 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: With public health emergencies (PHE) worldwide increasing, the perceived risk of PHE has been one of the critical factors influencing college students’ psychological distress. However, the mechanisms by which the perceived risk of PHE affects college students’ psychological distress are not clear. The study’s purpose was to investigate the mediation roles of deviation from a balanced time perspective (DBTP) and negative coping styles between the perceived risk of PHE and psychological distress. Methods: A convenience sampling method was used to survey 1054 Chinese college students with self-reporting. Data was collected using the Public Risk Perception Scale (PRPS), the Zimbardo Time Perspective Inventory (ZTPI), the Simplified Coping Style Questionnaire (SCSQ), the PHE Anxiety Scale, and the Chinese version of the Patient Health Questionnaire (PHQ). The associations between the perceived risk of PHE, DBTP, negative coping styles, and psychological distress were clarified using the correlation analysis. Additionally, the mediating roles of DBTP and negative coping styles between the perceived risk of PHE and psychological distress were investigated using a structural equation model. Results: The findings revealed low to moderate correlations between the variables studied. Students’ perceived risk of PHE was a positive predictor of their psychological distress (β = 0.219, p < 0.01). DBTP and negative coping styles played chain mediation roles between them with the effect being 0.009 and a 95% Boot CI of [0.003, 0.023]. This chain mediation model had an excellent fit index (χ2/df = 4.732, CFI = 0.973, TLI = 0.930, RMSEA = 0.048, SRMR = 0.047). Conclusion: These findings showed how the perceived risk of PHE affected college students’ psychological distress. Specifically, these results suggested that improving students’ mental ability to switch effectively among different time perspectives depending on task features and situational considerations and reducing their negative coping styles might be effective ways to promote their mental health.Keywords
Recently, public health emergencies (PHE) have become more commonplace globally [1]. Only in the first two decades of the 21st century there were five severe PHEs caused by major infectious diseases, including the severe acute respiratory syndrome (SARS) in 2003, the type A H1N1 influenza (H1N1) in 2009, the Middle East respiratory syndrome (MERS) in 2012, the Ebola virus disease (EVD) in 2014, and the novel coronavirus pneumonia (COVID-19) at the end of 2019. With the characteristics of high contagiousness, unpredictability, and inability to be managed with routine resources [2], PHE is not only prone to cause increased illness, injury, or death, but also has resulted in a range of psychological distress, such as anxiety and depression [3]. For example, various surveys indicated that 27.5% to 83.3% of EVD survivors had obvious anxiety symptoms and that 12% to 75% were diagnosed with depression [4]. Another survey indicated that COVID-19 has resulted in a 27.6% increase in cases of major depressive disorders and a 25.6% increase in cases of anxiety disorders worldwide throughout 2020 [5].
For the reason why individuals are vulnerable to psychological distress under PHE, the social risk theory poses that specific risk factors, such as epidemics, could potentially endanger society or individuals under particular social circumstances and conditions [6]. Furthermore, individuals’ perception of risks might significantly impact their mental health. Specifically, when the risk of epidemics becomes unpredictable, individuals’ risk perception might increase, consequently triggering negative emotions such as anxiety and depression. Risk perception describes an individual’s subjective perception and comprehension of different objective risks in the external environment, including the assessment of the likelihood and possible hazards of crisis occurrences [7]. The uncertain direction and severity of sudden PHE could result in increased risk perception, thereby intensifying individuals’ psychological pressure and negative emotions [8]. Indeed, most studies have indicated that there was a substantial correlation between risk perception and mental health [9–13]. For example, it was discovered that greater perceived risk was linked to increased mental health problems during the H1N1 and EVD outbreaks [9,10]. According to a survey conducted among 924 college students, the perceived risk of COVID-19 was strongly correlated with psychological distress and internet addiction [11]. Moreover, with the data from the Avon Longitudinal Study of Parents and Children (ALSPAC), Dyer et al. found higher COVID-19 risk perceptions were cross-sectionally associated with higher anxiety, higher depression, and lower well-being [12]. A systematic review and Meta-analysis with 81 papers also indicated that there were strong relationships between risk perception and fear and moderate relationships between risk perception and anxiety [13].
Although previous studies above have shown that risk perception was positively linked to psychological distress, more and more scholars stated that stress did not inevitably turn into psychological distress. Individuals might respond differently to stressful life experiences because of various psychological mechanisms [11,14]. Only a small number of research, meanwhile, have looked into possible inner psychological mechanisms. A survey among 204 healthcare professionals found resilience played a mediating role between risk and mental health problems [15]. Although this study might shed light on the possible mechanism underlying risk perception and psychological distress, it only focused on individual psychological resources and ignored the effects of other potential mediators, such as individual cognitive and behavioral resources. Some studies also revealed that cognitive and behavioral resources could improve personal resilience and reduce negative emotions [16,17]. Additionally, according to the theory of time perspective [18], the stress process model [19], the model of diathesis-stress interaction [20], and the dual-pathway framework for time perspectives and subjective well-being [21], balanced time perspective (BTP) and coping styles might play significant mediators between stress and mental health. Facing a high-pressure event, individuals commonly reported that time seems to have moved in slow motion [22]. Individuals with BTP possess the mental ability to switch flexibly between the past, present, and future perspectives in response to situational requirements, consequently increasing their satisfaction with life, happiness, and mental health [18,23]. Moreover, during exposure to stress, different individuals, or the same individual under various conditions, may adopt different coping styles. During the outbreak of COVID-19, individuals with higher perceived stress or risks more frequently adopted negative coping styles [24]. Therefore, BTP and negative coping styles might also play mediating roles between risk perception of PHE and psychological distress.
The mediating role of balanced time perspective
Since Frank theorized that traumatic experience might be an essential factor affecting individual time perspective in 1939 [25], more and more studies have begun to focus on the relationships between trauma exposures or stress and individual time perspective. Frank conceptualized time perspectives being relative dimensions of time that emphasized the past, present, and future. In his viewpoint, alarming previous experiences were hard to erase from memory, resulting in the past having power over the present rather than the present controlling the past. Meanwhile, the past also distorted the future, resulting in a compromise of the future to the present further. Put simply, an individual’s reality is a complicated interplay of past, present, and future time perspectives. Zimbardo and Boyd also argued that the ability to alternate between the five time-perspective domains (i.e., past-negative, past-positive, present-fatalistic, present-hedonistic, and future) based on situational demands allowed individuals to operate at peak levels of functioning [18]. Since then, more and more studies have focused on the importance of BTP [26–28]. BTP refers to the ability to switch effectively between temporal horizons depending on situational and environmental demands. Indeed, more BTP would help to increase individuals’ satisfaction with life, happiness, and mental health and decrease their negative effects [18,23]. Although there were various approaches to operationalizing BTP, the most commonly used method was to compute a deviation from a balanced time perspective (DBTP) [26,28].
Recently, numerous studies have examined the mediating role of DBTP between trauma exposures or stress and mental health [23,29–31]. A survey conducted among 280 motor vehicle survivors found that the association between temperament and degree of post-traumatic stress disorder (PTSD) was mediated by DBTP. When individuals were exposed to more severe trauma, they were prone to strong emotional reactions and were less flexible in coping with trauma, consequently triggering PTSD [29]. Similarly, more studies have also indicated that DBTP could play a mediating role between lifetime trauma exposure and optimism [23], between lifetime trauma exposure and life quality [30], and between lifetime trauma exposure and PTSD [31].
Taken together, when exposed to stressful or traumatic events, such as PHE, individuals are prone to form DBTP, which leads to psychological distress. Thus, this study hypothesized that college students’ DBTP played the mediating role between risk perception of PHE and psychological distress (Hypothesis 1, H1).
The mediating role of negative coping styles
Coping style pertains to the cognitive and behavioral approaches that individuals apply to deal with their psychological distress in response to stressful events and situations [32]. Faced with stressful or traumatic events, individuals always have a variety of ways to deal with these events. Some of them employ positive coping styles, including deploying cognitive resources and seeking social support, while some employ negative coping styles, including cognitive avoidance and substance abuse [33]. All these coping styles are significantly correlated with mental health. Indeed, most studies have indicated that positive coping styles could generate positive emotions and behaviors, while negative coping styles were significantly associated with severe psychological distress [11,34]. Moreover, a meta-analysis with 307 primary studies has indicated a significantly positive correlation between positive coping styles and well-being and a moderately positive correlation between negative coping styles and mental symptoms among 147,523 Chinese populations [35]. Similarly, a longitudinal study with 553 Switzerland adolescents found negative coping styles were significantly associated with more anxiety and depression [36].
Regarding the associations between stress and mental health, more and more theories, such as the stress process model [19] and the model of diathesis-stress interaction [20], assumed that stress was only a risk factor affecting an individual’s mental health rather than a direct factor. There were many mediating variables between them, including coping styles. For example, a study with 356 Chinese rural older adults found that perceived stress linked to their mental health mainly through coping styles, with a contribution rate above 42.11% [37]. With a longitudinal cross-lagged study in a sample of 231 university students, coping styles were found as mediators between perceived stress and life satisfaction at both two waves [38]. Moreover, risk perception was mainly constructed by uncertainties about the environment [39]. Under PHE, individuals often perceive uncertainties in all aspects of life and are prone to adopt more negative coping styles, which increase psychological stress [40]. Indeed, compared with positive coping styles, negative coping styles’ contribution rate between stress and mental health was larger [37]. Most studies indeed indicated that positive coping styles did not mediate the relationship between stress and mental health, while negative coping styles did mediate the relationship between stress and mental health [11]. Thus, college students’ risk perception of PHE might be linked to psychological distress via negative coping styles (Hypothesis 2, H2).
The chain mediating roles of balanced time perspective and negative coping styles
Based on a dual-pathway framework for time perspectives and subjective well-being [41], BTP not only directly predicts mental health, but also indirectly affects mental health through behavioral coping [21]. Indeed, time perspective could predict anxiety through coping style [42]. Li et al. summarized that when negative, unsustainable time perspective (e.g., negative past/future, present fatalism) predominates, individuals tend to behave more impulsively and un-developmentally (e.g., aggression, substance addiction, etc.), disrupting mental health. On the contrary, a positive and sustainable time perspective combination motivates individuals to adopt a series of adaptive behaviors to support mental health. That means when individuals develop DBTP, they are prone to apply negative coping styles, which lead to psychological distress. To our knowledge, there is no research to prove it.
Based on all these literature reviews above, DBTP and negative coping styles might have a chain mediating effect between risk perception and psychological distress (Hypothesis 3, H3). Fig. 1 describes the hypothetical conceptual model.
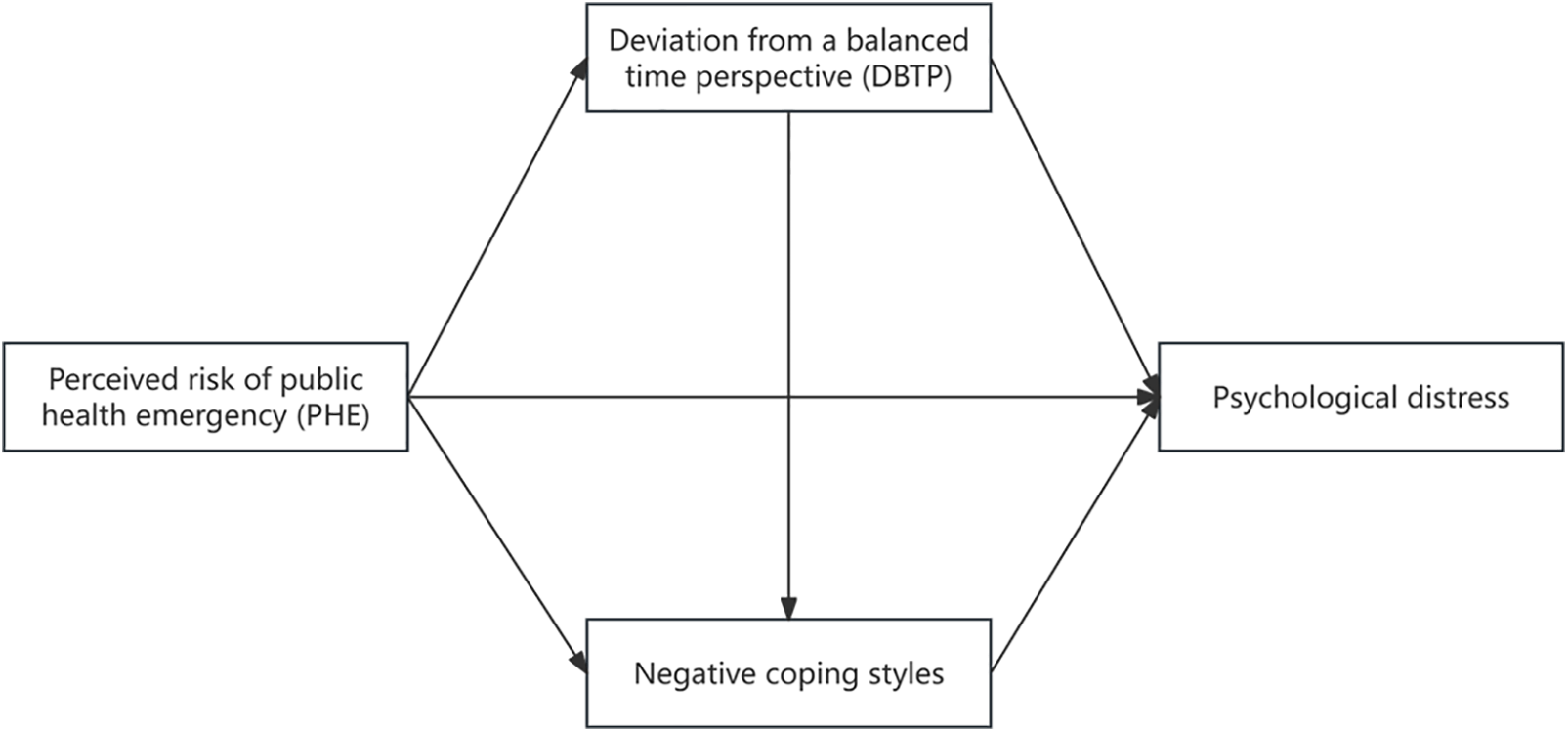
Figure 1: The hypothetical conceptual model.
Although the effect of PHE on psychological distress exists among the overall population, such as patients, isolated patients, medical staff, and the general public [1], college students are a particular group that deserves attention. First, college students are in a crucial phase of neuro- and psychological maturation, and they are prone to psychological distress. Previous studies have reported that as much as 30% of college students experience anxiety and depression [3,11]. Second, during the outbreak of PHE, most colleges and universities would adopt various preventive measures, such as campus lockdowns for extended periods, which might significantly disrupt college students’ regular daily life, campus activities, and social connections, increasing their psychological distress [43]. College students’ prevalence of depressive symptoms was 71% during quarantining [44]. This study attempted to investigate the internal linking mechanism between risk perception of PHE and psychological distress among college students, namely the mediating roles of BTP and negative coping styles. Therefore, it offered a practical foundation for the efficient implementation of college students’ mental health education during a PHE. The main research question was whether BTP and negative coping styles could play mediating roles between risk perception of PHE and psychological distress among college students. Specific hypotheses were presented in the literature review above.
Since the present study was exploratory and there were no analyses regarding associations between the perceived risk of PHE, DBTP, negative coping styles, and psychological distress among college students, a cross-sectional design was applied [45]. Meanwhile, in line with the purpose and research question, the structural equation modeling (SEM) examined the mediation effects of DBTP and negative coping styles with 5000 bootstrap samples and estimates of indirect effects [46]. The sampling distribution of the indirect effect was obtained, enabling the output of point estimate, standard error, and 95% bias-corrected bootstrapped confidence intervals (95% Boot CI) of the mediation effect. Bootstrapping allowed for higher analytical power combined with a lower risk of committing Type I error [47]. 95% Boot CI helped to identify significant mediation effects [47].
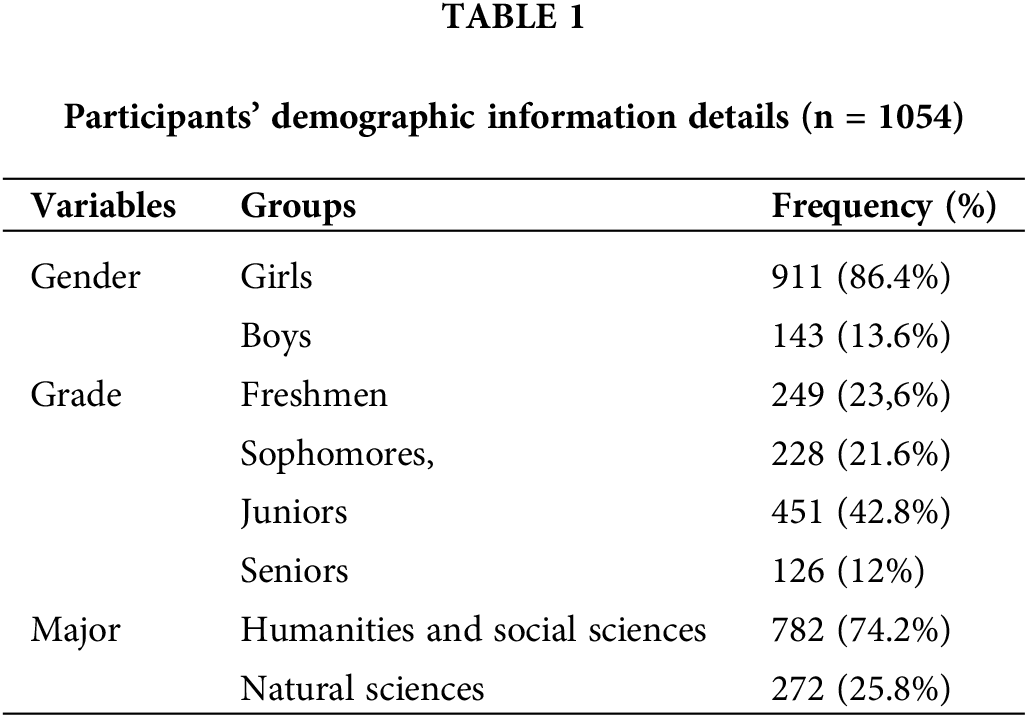
The present study used a convenient sampling method, which was frequently applied in the field of mental health under a PHE [48]. This sampling could assist researchers gather huge samples quickly and needs minimal cost [48]. The following were the sampling procedures. Reaching out to a few college deans at a university in Shaanxi Province, China, was the first step. Researchers introduced them to our main research purposes. Subsequently, the deans assigned the investigation tasks to several course teachers. Third, these teachers distributed an electronic Quick Response (QR) code from a reliable Chinese online platform “Wenjuanxing” to their class-attending students before or after class. All data was collected through self-report questionnaires. The study was approved by the Ethics committee at Nanjing Normal University (IRB number: NNU202401002). All participants signed the informed consent in this study. Finally, a total of 1106 college students participated in our investigation. Excluding cases of invalid answers (e.g., continuous usage of an option, too short or too long response time, missing data larger than 10%, etc.), the final number of participants was 1054. The valid response rate was 95.3%. The final participants ranged in age from 17 to 25 years (M = 20.4, SD = 1.6), with 86.4% of them being girls (n = 911) and 13.6% being boys (n = 143). There embraced 249 freshmen, 228 sophomores, 451 juniors, and 126 seniors. A total of 272 students majored in the scientific sciences while 782 students majored in the humanities and social sciences. Table 1 displays the participants’ demographic details.
The perceived risk for PHE was evaluated by the Public Risk Perception Scale (PRPS) [49]. There were 10 items assessing the severity, controllability, severity of health impact, and prevalence possibility. Participants rated each item with a Likert-5 point ranging from 1 (totally not compliance) to 5 (totally compliance). Higher scores indicated a higher perceived risk of PHE. Cronbach alpha for these dimensions and the whole scale were 0.802, 0.854, 0.824, 0.859, and 0.904, respectively.
Zimbardo time perspective inventory
Time perspective was evaluated by the Zimbardo Time Perspective Inventory (ZTPI), developed by Zimbardo et al. [18] and modified by Wang [50]. There were 25 items assessing the past positive (six items), the past negative (seven items), the present impulsive (four items), the present fatalistic (three items), and the future (five items). Participants rated each item with a Likert-5 point ranging from 1 (very untrue of me) to 5 (very true of me). Cronbach alpha for these dimensions were 0.910, 0.835, 0.775, 0.835, and 0.815, respectively. DBTP was calculated based on Stolarski and colleagues’ formula [26,28,51].
Simplified coping style questionnaire
Coping style was evaluated by the Chinese version of the Simplified Coping Style Questionnaire (SCSQ) [52]. This scale comprised 20 items, with 12 items for positive coping styles and eight items for negative coping styles. Participants rated each item with four choices (never used, occasionally used, sometimes used, often used). Higher scores indicated a higher related coping style. In the current study, we only adopted the negative coping style section. Cronbach’s alpha was 0.789.
The degree of anxious symptoms was evaluated by the PHE Anxiety Scale, developed based on the Chinese version of the Coronavirus Anxiety Scale (CAS) [53]. This scale comprised five items with a Likert-5 point ranging from 0 = not at all to 4 = nearly every day. Cronbach alpha for the current study was 0.968. The degree of depressive symptoms was evaluated by the Chinese version of the Patient Health Questionnaire (PHQ) [54]. This scale comprised nine items with a Likert-4-point ranging from 0 = not at all to 3 = nearly every day. Cronbach’s alpha for the current study was 0.907. By summing the Z-scores from these two scales, we were able to determine the degree of psychological distress.
Firstly, participants’ sample characteristics were analyzed using the frequency and percentage. Secondly, the effects of the unmeasured latent method factor were considered while testing the Common Method Bias (CMB). Meanwhile, we applied SPSS 23.0 to test the reliability and validity of the applied scales. Thirdly, three-way ANOVA was used to examine the effect of demographic variables on the main variables studied. Fourthly, we computed the mean and standard deviation and conducted the correlation matrix and descriptive statistics analyses. Lastly, SEM was used by the Mplus 7.20 program to examine the mediating effects. The statistical significance of each mediating effect was estimated using 5000 bootstrapped resamples and 95% Boot CI, with the value ‘zero’ falling outside indicating that mediation would be considered, structural equation model was used by Amos 26.0 program. A threshold p-value of 0.05 was used to determine statistical significance.
Common methodological deviations
Given that self-reporting measures might be influenced by some issues related to CMB, reverse scoring controls were implemented for some items while protecting participant privacy. Meanwhile, Harman’s one-way variance analysis was conducted throughout data processing to examine the effects of CMB. The findings showed 12 eigenvalues greater than 1, explaining 63.78% of the variance. The first factor’s variance explanation was 19.01%, significantly below the 40% cut-off, suggesting that CMB’s effect was insignificant.
Demographic information and bivariate correlation
The overall effects of gender, grade, and major, as well as their interactions, were examined through three-way ANOVA. According to Cohen’s guidelines for interpreting the F-test effect size (small = 0.01, medium = 0.059, and large = 0.138), no significant main effects or interaction effects were observed. Therefore, all these demographic variables were not further considered in the subsequent analyses. See more details in Table 2.
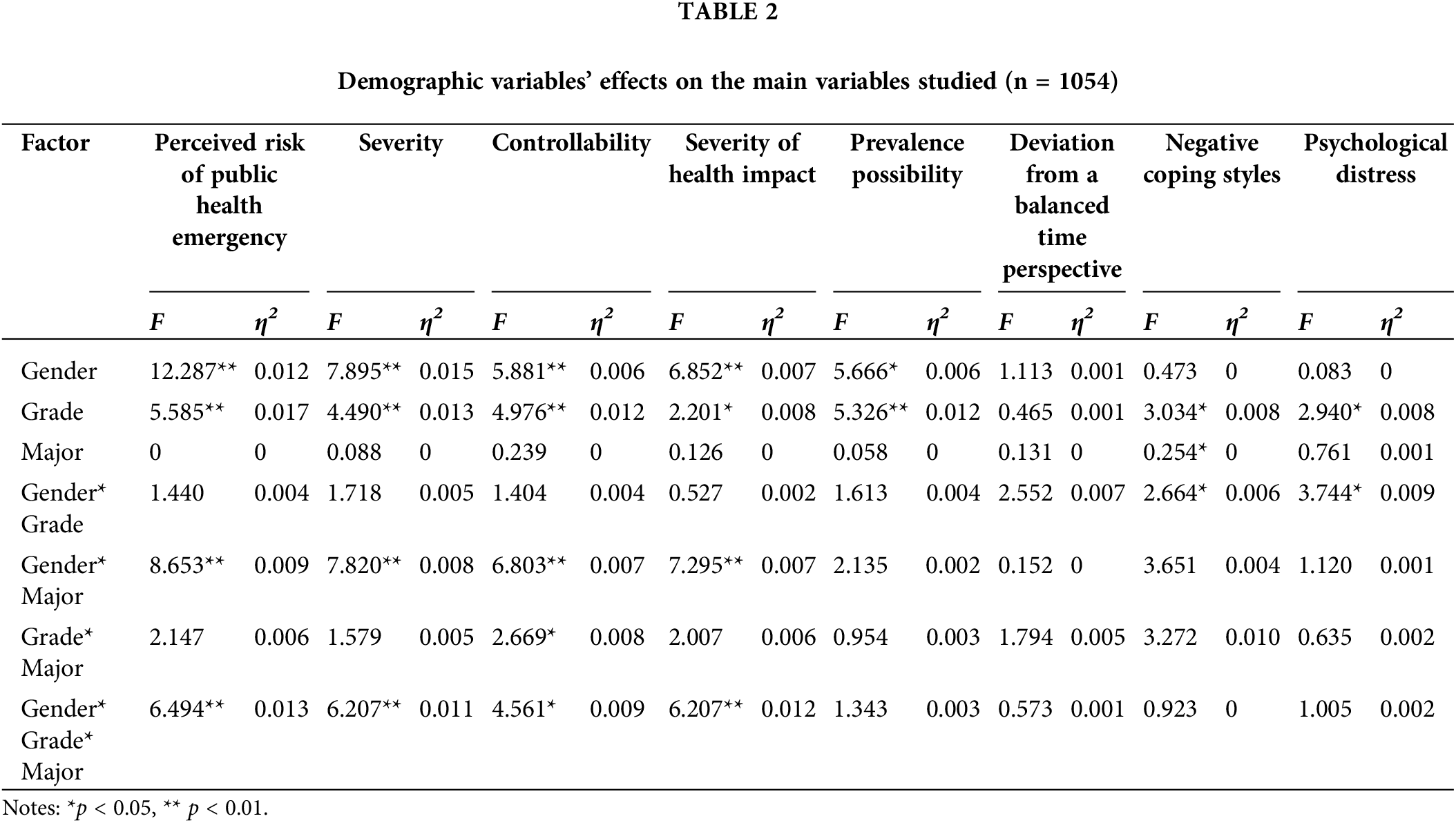
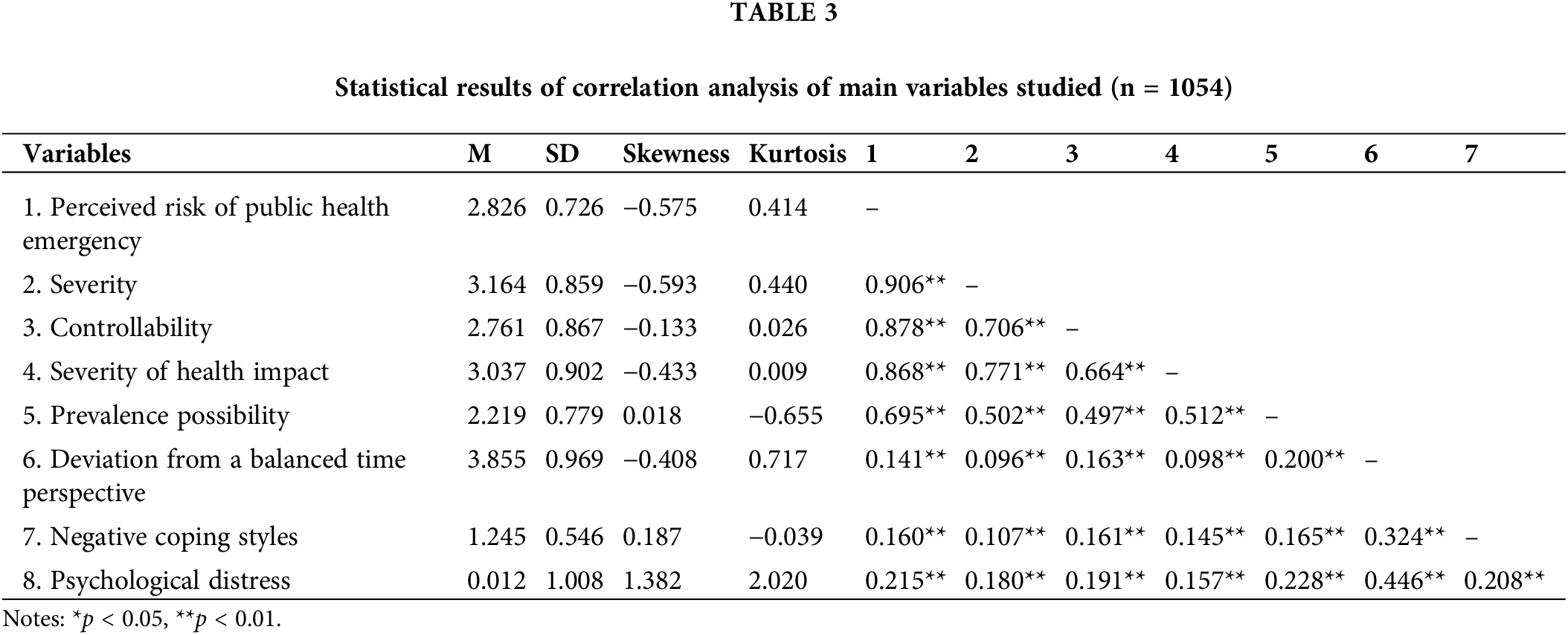
Table 3 shows the descriptive statistics of the variables studied and their correlations. For these main variables studied, the kurtosis ranged from −0.655 to 2.020, whereas the skewness fell between −0.593 and 1.382. According to Kim’s suggestion, our data did not violate the normal distribution [55]. The perceived risk of PHE (r = 0.141, p < 0.01), severity (r = 0.096, p < 0.01), controllability (r = 0.163, p < 0.01), the severity of health impact (r = 0.098, p < 0.01), and the prevalence possibility (r = 0.200, p < 0.01) exhibited significant positive associations with DBTP. The perceived risk of PHE (r = 0.160, p < 0.01), severity (r = 0.107, p < 0.01), controllability (r = 0.161, p < 0.01), the severity of health impact (r = 0.145, p < 0.01), and the prevalence possibility (r = 0.165, p < 0.01) exhibited significant positive associations with negative coping styles. The perceived risk of PHE (r = 0.215, p < 0.01), severity (r = 0.180, p < 0.01), controllability (r = 0.191, p < 0.01), the severity of health impact (r = 0.157, p < 0.01), and the prevalence possibility (r = 0.228, p < 0.01) exhibited significant positive associations with psychological distress. Additionally, DBTP exhibited significant positive associations with negative coping styles (r = 0.324, p < 0.01) and psychological distress (r = 0.446, p < 0.01). Finally, negative coping styles exhibited significant positive associations with psychological distress (r = 0.208, p < 0.01).
Mediating Effects of DBTP and Negative Coping Style
To examine all the hypotheses above, the current study constructed a chain model of DBTP and negative coping styles between the perceived risk of PHE and psychological distress. The results showed this model had an excellent fit index (χ2/df = 4.732, CFI = 0.973, TLI = 0.930, RMSEA = 0.048, SRMR = 0.047). The perceived risk of PHE positively affected DBTP (β = 0.152, p < 0.01), negative coping style (β = 0.091, p < 0.01), and psychological distress (β = 0.219, p < 0.01). DBTP positively affected negative coping style (β = 0.174, p < 0.01) and psychological distress (β = 0.429, p < 0.01). Negative coping styles positively affected psychological distress (β = 0.104, p < 0.01). See more details in Fig. 2.
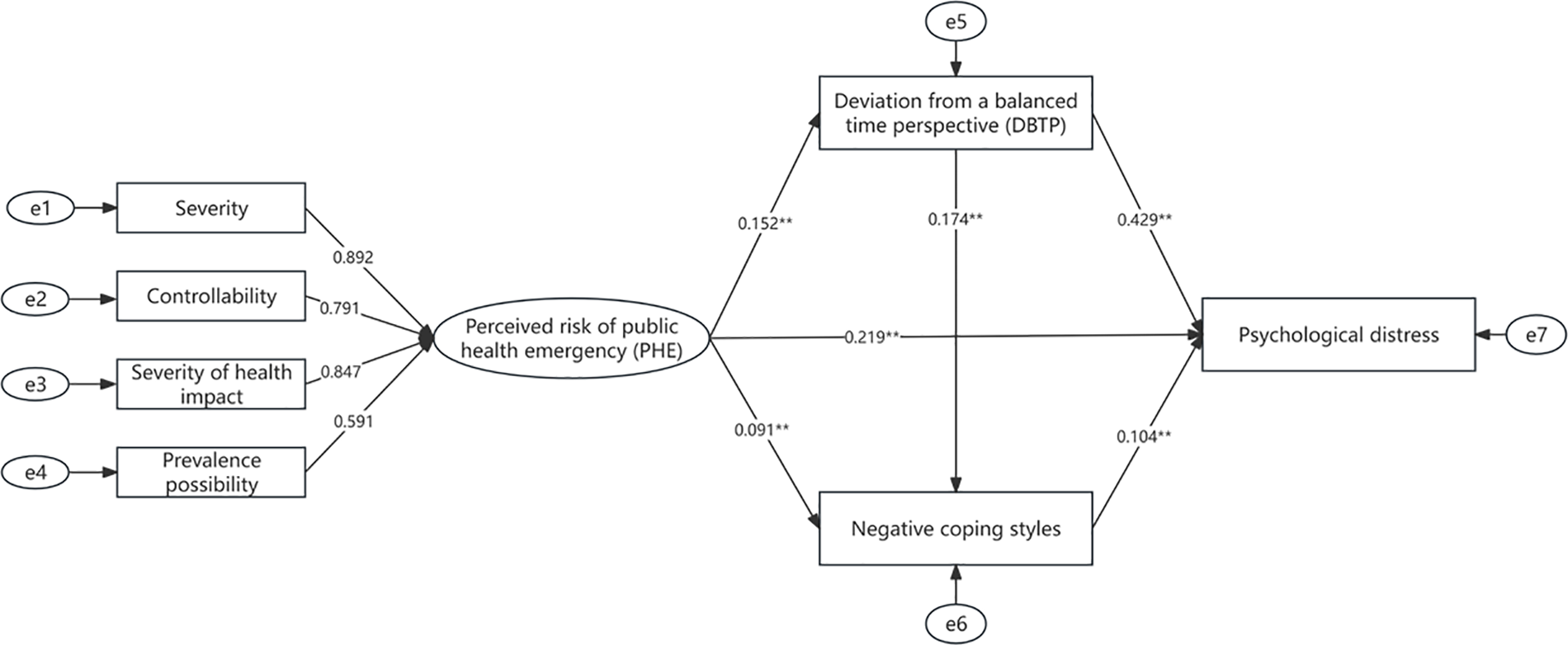
Figure 2: A chain model of DBTP and negative coping styles. Note: **p < 0.01.
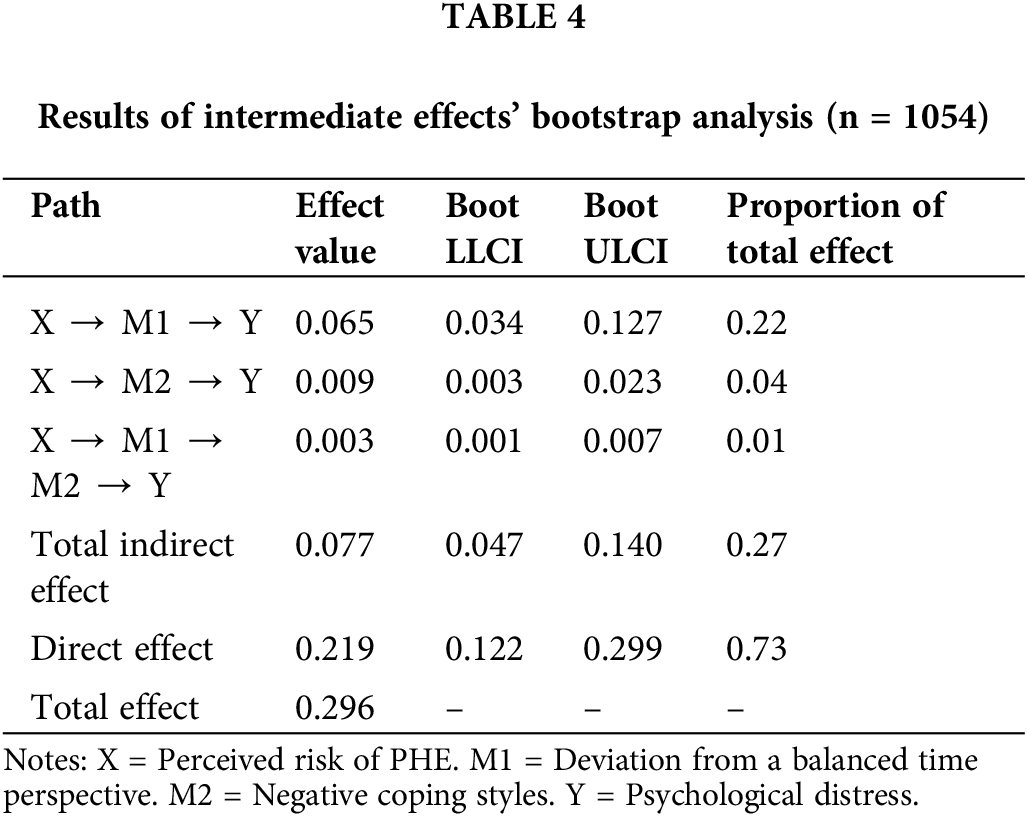
A bias-corrected nonparametric percentage Bootstrap was further applied to produce trustworthy findings of the mediation effect. The 95% Boot CI without 0 indicated an apparent mediating effect. The results are presented in Table 4. There were three indirect effect paths (see Table 4). First, the effect of the perceived risk of PHE → DBTP → psychological distress was 0.065, with a 95% Bootstrap confidence interval of [0.034, 0.127]. Second, the effect of the perceived risk of PHE → negative coping styles → psychological distress was 0.009, with a 95% Boot CI of [0.003, 0.023]. Third, the effect of the perceived risk of PHE → DBTP → negative coping styles → psychological distress was 0.003, with a 95% Boot CI of [0.001, 0.007].
Based on the theory of time perspective [18], the stress process model [19], the model of diathesis-stress interaction [20], and the dual-pathway framework for time perspectives and subjective well-being [21], this study explored the inner mechanism between college students’ risk perception of PHE and psychological distress. A higher perceived risk of PHE was linked to more significant psychological distress. In addition, college students’ experiencing risk perception of PHE also indirectly affected psychological distress through the mediating roles of DBTP, negative coping styles, and the chain of DBTP to negative coping styles. The current results validated the idea that risk perception of PHE might impact psychological distress and provided an in-depth discussion of the specific intermediary mechanisms between the factors, providing broader theoretical and practical contributions for relieving psychological distress related to PHE.
First, this study confirmed H1 that DBTP played a significant mediating role between the perceived risk of PHE and psychological distress. The perceived risk of PHE, as a typical risk perception, can cause individuals to experience significant stress [56] and get biased in focusing on the negative past [23]. Thereby, a negative past would control their present perspective, rather than the present taking control of the past. Meanwhile, a biased concentration on the negative past might also distort their future perspective and reduce their optimism for the present and the future [18,25]. All these circumstances likely result in the DBTP. Therefore, students with a higher perceived risk of PHE are less likely to be balanced among various time perspectives. Individuals with more BTP might be better equipped to deal with current stressful situations by learning from past experiences, living in the moment, and pursuing plans and other life goals. All these attitudes and behaviors would help individuals to increase their satisfaction with life, happiness, and mental health and decrease their negative effects [18,23]. Therefore, a higher perceived risk of PHE increases students’ psychological distress through DBTP, consistent with the previous research results [23,29–31]. Meanwhile, from the top-down perspective, individuals’ well-being is mostly determined by their habitual approaches to reflecting upon the circumstances and occurrences, instead of these circumstances and occurrences themselves [57]. Meanwhile, individuals’ appraisals and interpretations of the present events were not just by their immediate thoughts and current status, but also by the previous life moments and the anticipating future events [58]. Time perspective refers to how individuals categorize their experiences into different temporal states. Time perspective is always deemed as a critical source of what is chronologically available in one’s memory when one evaluates well-being [18]. The BTP was defined as a cognitive restructuring of time horizons in response to situational demands [18]. Namely, a BTP allows people to meet these demands with their “temporal flexibility”, such as knowing when to enjoy themselves and when to be goal-directed [26]. Consequently, a greater DBTP leads to decreased well-being and elevated psychological distress. A recent systematic review has shown a significantly positive correlation between DBTP and distress, anxiety, symptoms of affective disorders, and burnout [58]. Thus, paying more attention to college students’ temporal states and cultivating their ‘temporal flexibility’ might be effective ways to cope with PHE and mitigate their psychological distress.
Second, this study also confirmed H2 that college students’ perceived risk of PHE was linked to psychological distress via negative coping styles, consistent with the assumptions of several theories [19,20] and the conclusions of some previous studies [37–40]. Individuals who perceive themselves at a higher risk of PHE might be more prone to adopt negative coping styles, and further tend to experience a higher level of psychological distress. The reason why students tend to apply negative coping styles under PHE might be related to their low perceived control. Perceived control is the personal perception of having the ability to affect events and accomplish desired outcomes, rather than being dependent on external causes [59]. Individuals who have a strong sense of control can take control of their lives well. On the contrary, individuals who perceive low control always exhibit behavioral rigidity because they believe that the world is unchangeable [60]. When individuals feel threatened by risk, they frequently experience a lack of control [61]. That leads individuals to perceive that changes in the environment are not contingent upon their own actions, efforts, and choices [62], and thus adopt more negative coping styles [63]. Another explanation might be correlated to students’ low coping capacity for PHE. A survey among 7719 Chinese college students indicated that although students’ prevention ability before the event was relatively high, their incident precaution ability and post-event cooperation and disposal abilities both need to be strengthened [64]. The lack of these abilities often leads individuals to adopt negative coping styles to unexpected risk events. Negative coping styles are insufficient to deal with external threats and obstruct individuals from dealing with and solving problems actively, thereby increasing their psychological distress [11,34–36], consistent with the stress process model [19] and the model of diathesis-stress interaction [20]. The factors contributing to individual psychological distress with negative coping styles are as follows. Negative coping styles are typically linked to more passive coping behaviors, such as denial, disengagement, intentional avoidance, internet addiction, and misuse of substances. All these behaviors were significantly associated with psychological distress, including depression and anxiety [11]. With an in-depth exploration, an increasing number of studies have supported that the concept of helplessness was at the root of all the aforementioned passive behaviors [65,66]. Individuals who experience helplessness tend to internalize the negative aspects of the problem, magnify their limitations, and focus on the negative aspects of the current situation, which in turn intensifies their psychological distress [67]. Thus, future mental health interventions for college students under PHE should not only focus on individuals’ coping behaviors but also internalization beliefs and attitudes, such as helplessness.
Third, college students’ DBTP and negative coping styles could play chain mediation roles between the perceived risk of PHE and psychological distress, confirming H3. When college students perceive themselves at a higher risk of PHE, their mental ability to switch effectively among different time perspectives depending on task features, situational considerations, and personal resources would be weakened. As a result, college students were more likely to engage in more impulsive and underdeveloped coping, thereby intensifying their mental health. All these findings supported a dual-pathway framework for time perspectives and mental health [21,41]. Nonetheless, the effect size of chain mediation was small and its Boot LLCI was 0.001, which was actually close to 0. All these findings indicated that the chain mediation model was not ideal. The possible reason might be that time perspective had an impact on individuals’ mental health via specific behaviors, such as aggression, substance abuse, healthy lifestyle, etc. Coping styles were the sum of all cognitive and behavioral strategies used by an individual to manage the internal and external demands of stressful events behaviors [32] and did not refer to specific behaviors. The chain mediation roles of DBTP and coping styles between the perceived risk of PHE and psychological distress need to be further studied.
Finally, we want to take cultural factors into our discussion. Culture is a factor influencing one’s time perspective and coping styles. Regarding time perspective, while both the Eastern and the Western prioritize acknowledging the eternity, power, and value of “time”, there are notable distinctions [68]. The Western emphasizes the linear aspect of time, believing that only one task may be done within a given time frame. In contrast, the Eastern views the multi-faceted structure of time, believing that numerous tasks would be completed within the same time frame. In addition, the Western emphasis on the impact of time on individuals, whereas Chinese individuals have a long-standing appreciation for their experience of time and the “opportunities” it holds. Considering these cultural disparities, Fu et al. developed the Three-Dimensional Structural Model of Time Perspective specifically for the Chinese population. The Chinese individuals’ time perspective is characterized by the following features: (1) a focus on the interconnectedness of the past, present, and future; (2) a respect for the laws governing the occurrence and progression of time; (3) an emphasis on the role of individuals’ “active will” within historical time. When individuals lose their BTP, they will experience the negative effects of the “modern time syndrome” [69]. Individuals’ BTP generally remained reasonably consistent from adolescence to early adulthood but had a significant decline from early adulthood to Middle Ages [70], thus the college stage is a crucial period for developing a BTP. A sudden PHE would disrupt college students’ regular daily life, consequently resulting in a strong sense of fragmentation in their time perspective. They would be prone to ruminating on the past and losing hope for the present and the future. Furthermore, due to the unmanageable nature of the PHE, individuals will lose their sense of control and meaning in life. Multiple studies have demonstrated that a negative time perspective, less perception of control over one’s life, and meaning in life are all significantly related to college’s mental well-being and mental health [18,59–61,71]. Regarding coping styles, they are related to individuals’ social orientations [72]. Western culture is characterized by individuals who have autonomous social orientations that prioritize autonomy, self-direction, and self-expression. They view themselves as distinct from others. In contrast, individuals from East Asian cultures typically exhibit interdependent social orientations that prioritize harmony and relatedness, considering themselves as interconnected through relationships. During the outbreak of PHE, most Chinese colleges and universities adopted various preventive measures, such as campus lockdowns for extended periods, which might significantly affect their psychological distress [43,44]. The possible explanation for this result is that these preventive measures disrupt the interaction between college students and their social network, leading to a decline in the support they receive for their coping behaviors. Numerous studies have indicated that social support has a significant role in influencing college students’ coping styles. Specifically, a lack of social support is strongly associated with negative coping styles [11].
The current study investigated the effect of risk perception of PHE on psychological distress among college students. It extended this inquiry by examining the mechanisms through which DBTP, negative coping styles, and DBTP to negative coping styles mediated this association. Nevertheless, it is important to consider the limitations of our study when interpreting our findings. First, only self-report scales were used to rate students’ anxiety and depression, which failed to rule out memory biases and personal desirability when examining the immediate response of an individual’s emotional experiences [73]. Emotions are dynamic, and their nature depends on the current situation [74]. In the future, an experience sampling method can be used to understand students’ daily emotional experiences and daily emotional regulation habits [75]. Second, the present study applied a cross-sectional design, which limited further exploration of the cause-and-effect relation. Longitudinal designs or experimental studies might provide new insights into the causal relationships between risk perception of PHE and psychological distress. Third, the present study applied a variable-centered approach to determining the relative potency of risk perception of PHE on psychological distress, which failed to regard the individual as the unit of analysis [76]. Among 7 844 residents from 30 provinces in China, a survey found there were three various risk perception profiles, including low risk-perception (23.9%), high risk-perception (29.3%), and high risk-perception with low-susceptibility (46.8%) [77]. These three profiles had different effects on residents’ coping styles and mental health. Therefore, future studies need to apply person-centered approaches to identify the latent profiles of students’ risk perception of PHE and discover their different effects on coping styles and mental health. Fourth, the research was conducted in China, which limited the generalizability to other cultural backgrounds. Culture is a factor influencing one’s time perspective and coping styles. Chinese culture upholds the concept “he”(和), reflecting the idea of balance. That coincides with BTP. Compared with Westerners, whether deviation from the balance is more likely to cause psychological distress for Chinese is worthy of further exploration. When it comes to coping styles, Easterners prioritize self-discipline and strive to avoid inconveniencing others. In contrast, Westerners value self-expression and strive to solve problems by seeking various resources. Faced with psychological crises, self-discipline and implicit personality traits make Easterners less good at expressing their needs than Westerners [78]. A PHE distorts the balance of individuals’ temporal states. Faced with the stressful event and the imbalance, a Chinese individual may feel reluctant to openly express their need for assistance due to concerns about inconveniencing others, which gets them in more trouble and psychological distress. Whether there is cross-cultural invariance for these relations needs to be further explored with diverse cultural backgrounds.
This study revealed the psychological transformation mechanism of college students’ risk perception of PHE and psychological distress. DBTP was the critical factor in understanding perceived risk and psychological distress. When college students perceived the risk of PHE, they could not switch flexibly between the past, present, and future time perspectives depending on situational demand, leading to more psychological distress in the present. This process further supported the time perspective theory [18,25]. Therefore, cultivating a BTP might be an essential goal of psychological intervention in PHE. So far, the Time Perspective Therapy has proven to be an effective way to develop individual BTP [79]. According to this therapy, its primary objective was to enhance individuals’ flexibility as they anticipate the future, instead of concentrating on past negative experiences, by keeping the past, present, and future time perspectives balanced. Effective psychological counseling should help college students learn from the past time perspective, live in the present time perspective, and plan for the future to reduce the negative effects of PHE on their mental health.
Individuals with a higher level of perceived risk of PHE might adopt negative coping styles and further tend to a higher level of psychological distress. This process further supported the stress process model [19] and the model of diathesis-stress interaction. This process also reminded practitioners and counselors of colleges that decreasing students’ negative coping styles might be an effective way to improve students’ mental health under PHE. For example, a previous intervention study has revealed that the Satir Model group psychological intervention could significantly reduce college students’ negative coping styles of applying illusion, self-blame, and withdrawal [80]. Secondly, students with a higher perceived risk of PHE might perceive low self-control, leading to adopting negative coping styles. Thus, strengthening college students’ self-control under PHE might be crucial. A review showed interventions based on the strength model of self-control could build greater capacity for self-control resources [81]. Thirdly, given that Chinese college students’ abilities to respond to PHE are relatively lacking, colleges should construct an emergency education system according to their actual situations, which not only includes theoretical courses for PHE but also pays more attention to practical activities such as emergency drill conducting and emergency base visiting. Finally, helplessness might be at the root of most negative coping styles. When an individual perceives helplessness, there will be symptoms such as reduced self-confidence, dissipation of passion, artificial, reduced stress resistance, etc. Future mental health interventions need to focus on students’ hope traits during the process. The spot group intervention and clinical case counseling were both effective approaches to enhance the experience of stateful hope for college students [82].
The present study demonstrates the association between risk perception of PHE and psychological distress among college students, as well as the mediating roles of DBTP, negative coping styles, and the chain of DBTP to negative coping styles. By doing so, this study extends the theory of time perspective, the stress process model, the model of diathesis-stress interaction, and the dual-pathway framework for time perspectives and subjective well-being. Additionally, the findings could give some insights into the successful implementation of mental health education for college students under PHE, such as conducting and practicing the Time Perspective Therapy, the Satir Model group psychological intervention, interventions based on the strength model of self-control, and emergency education. It is recommended to carry out additional research using an experience sampling method, a person-centered approach, and a longitudinal research design. Lastly, it is also crucial to replicate the findings in many cultural backgrounds.
Acknowledgement: We would like to thank the study participants for sharing their experiences and time. We also would like to thank all research assistants and support staff for working on this study.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirmed contribution to the paper as follows: study conception and design: Biru Chang; data collection: Biru Chang, Shengqiang Zhu; analysis and interpretation of results: Shengqiang Zhu, Yanghui Dai; draft manuscript preparation: Biru Chang, Qian Xie. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The analyzed data sets generated during the study are available from the corresponding author upon reasonable request.
Ethics Approval: The study was approved by the Ethics committee at Nanjing Normal University (IRB number: NNU202401002). All participants signed the informed consent in this study.
Conflicts of Interest: The authors declared that they had no conflicts of interest to report regarding the present study.
References
1. Wang Z, Wang D. The influence and enlightenment of five public health emergencies on public psychology since a new century: a systematic review. Int J Soc Psychiatry. 2021;67(7):878–91. doi:10.1177/00207640211002222. [Google Scholar] [PubMed] [CrossRef]
2. Nelson C, Lurie N, Wasserman J, Zakowski S. Conceptualizing and defining public health emergency preparedness. Am J Public Health. 2007;97(1):9–11. doi:10.2105/AJPH.2007.114496. [Google Scholar] [PubMed] [CrossRef]
3. Gilbert W, Bureau JS, Poellhuber B, Guay F. Predicting college students’ psychological distress through basic psychological need-relevant practices by teachers, peers, and the academic program. Motiv Emot. 2021;45(4):436–55. doi:10.1007/s11031-021-09892-4. [Google Scholar] [CrossRef]
4. Kaputu-Kalala-Malu C, Musalu EM, Walker T, Ntumba-Tshitenge O, Ahuka-Mundeke S. PTSD, depression, and anxiety in Ebola virus disease survivors in Beni town, Democratic Republic of the Congo. BMC Psychiat. 2021;21(1):342. doi:10.1186/s12888-021-03343-7. [Google Scholar] [PubMed] [CrossRef]
5. Daly M, Robinson E. Depression and anxiety during COVID-19. Lancet. 2022;399(10324):518. doi:10.1016/s0140-6736(22)00187-8. [Google Scholar] [PubMed] [CrossRef]
6. Fischhoff B. Risk perception and communication unplugged: twenty years of process. Risk Anal. 1995;15(2):137–45. doi:10.1111/j.1539-6924.1995.tb00308.x. [Google Scholar] [PubMed] [CrossRef]
7. Slovic P. Perception of risk. Science. 1987;236(4799):280–5. doi:10.1126/science.3563507. [Google Scholar] [PubMed] [CrossRef]
8. Peng H, Ju Q, Nie S, Gan Y. COVID-19 risk perception and negative emotional symptoms: mediating role of self-control and moderating role of life history strategy. Psych J. 2023;12(6):857–67. doi:10.1002/pchj.685. [Google Scholar] [PubMed] [CrossRef]
9. Bults M, Beaujean DJ, de Zwart O, Kok G, van Empelen P, van Steenbergen JE, et al. Perceived risk, anxiety, and behavioral responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: results of three consecutive online surveys. BMC Public Health. 2011;11(1):1–13. doi:10.1186/1471-2458-11-2. [Google Scholar] [PubMed] [CrossRef]
10. Yang JZ, Chu H. Who is afraid of the Ebola outbreak? The influence of discrete emotions on risk perception. J Risk Res. 2016;21(7):834–53. doi:10.1080/13669877.2016.1247378. [Google Scholar] [CrossRef]
11. Chang B, Hou J. The association between perceived risk of COVID-19, psychological distress, and internet addiction in college students: an application of stress process model. Front Psychol. 2022;13:898203. doi:10.3389/fpsyg.2022.898203. [Google Scholar] [PubMed] [CrossRef]
12. Dyer ML, Sallis HM, Khouja JN, Dryhurst S, Munafò MR. Associations between COVID-19 risk perceptions and mental health, well-being, and risk behaviours. J Risk Res. 2022;25(11–12):1372–94. doi:10.1080/13669877.2022.2127849. [Google Scholar] [PubMed] [CrossRef]
13. Zhao Y, Jiang Y, Zhang W, Zhu YC. Relationship between risk perception, emotion, and coping behavior during public health emergencies: a systematic review and meta-analysis. Systems. 2023;11(4):181. doi:10.3390/systems11040181. [Google Scholar] [CrossRef]
14. Li T, Xie Q. Effects of college students’ perceived stress on anxiety in the time of COVID-19: the chain mediation role of psychological resilience and regulatory emotional self-efficacy. Int J Ment Health Promot. 2022;24(2):263–76. doi:10.32604/ijmhp.2022.019177. [Google Scholar] [CrossRef]
15. Yıldırım M, Arslan G, Özaslan A. Perceived risk and mental health problems among healthcare professionals during COVID-19 pandemic: exploring the mediating effects of resilience and coronavirus fear. Int J Ment Health Addict. 2020;20(2):1035–45. doi:10.1007/s11469-020-00424-8. [Google Scholar] [PubMed] [CrossRef]
16. Christine AP, Kathleen AM. Strengths-based cognitive-behavioural therapy: a four-step model to build resilience. Clin Psychol Psychother. 2012;19(4):283–90. doi:10.1002/cpp.1795. [Google Scholar] [PubMed] [CrossRef]
17. Johnsen TJ, Friborg O. The effects of cognitive behavioral therapy as an anti-depressive treatment is falling: a meta-analysis. Psychol Bull. 2015;141(4):747–68. doi:10.1037/bul0000015. [Google Scholar] [PubMed] [CrossRef]
18. Zimbardo PG, Boyd JN. Putting time in perspective: a valid, reliable individual-differences metric. J Pers Soc Psychol. 1999;77(6):1271–88. doi:10.1037/0022-3514.77.6.1271. [Google Scholar] [CrossRef]
19. Pearlin LI, Menaghan EG, Lieberman MA, Mullan JT. The stress process. J Health Soc Behav. 1981;22(4):337–56. doi:10.2307/2136676. [Google Scholar] [CrossRef]
20. Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: implications for the depressive disorders. Psychol Bull. 1991;110(3):406–25. doi:10.1037/0033-2909.110.3.406. [Google Scholar] [PubMed] [CrossRef]
21. Li X, Yu X, Lv H. Balanced time perspective and mental health: mechanisms and theoretical framework. Adv Psychol Sci. 2024;32(1):138–50. doi:10.3724/SP.J.1042.2024.00138. [Google Scholar] [CrossRef]
22. Stetson C, Fiesta MP, Eagleman DM. Does time slow down during a frightening event? PLoS One. 2007;2(12):e1295. doi:10.1371/journal.pone.0001295. [Google Scholar] [PubMed] [CrossRef]
23. Tomich PL, Tolich A. Life is a balancing act: deviation from a balanced time perspective mediates the relationship between lifetime trauma exposure and optimism. Curr Psychol. 2019;40(5):2472–80. doi:10.1007/s12144-019-00191-3. [Google Scholar] [CrossRef]
24. Yu H, Li M, Li Z, Xiang W, Yuan Y, Liu Y, et al. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry. 2020;20(1):426. doi:10.1186/s12888-020-02826-3. [Google Scholar] [PubMed] [CrossRef]
25. Frank L. Time perspectives. J Soc Philos. 1939;4:339–58. [Google Scholar]
26. Zhang JW, Howell RT, Stolarski M. Comparing three methods to measure a balanced time perspective: the relationship between a balanced time perspective and subjective well-being. J Happiness Stud. 2012;14(1):169–84. doi:10.1007/s10902-012-9322-x. [Google Scholar] [CrossRef]
27. Stolarski M, Vowinckel J, Jankowski KS, Zajenkowski M. Mind the balance, be contented: a balanced time perspective mediates the relationship between mindfulness and life satisfaction. Pers Individ Differ. 2016;93(3):27–31. doi:10.1016/j.paid.2015.09.039. [Google Scholar] [CrossRef]
28. Stolarski M, Bitner J, Zimbardo PG. Time perspective, emotional intelligence and discounting of delayed awards. Time Soc. 2011;20(3):346–63. doi:10.1177/0961463x11414296. [Google Scholar] [CrossRef]
29. Stolarski M, Cyniak-Cieciura M. Balanced and less traumatized: balanced time perspective mediates the relationship between temperament and severity of PTSD syndrome in motor vehicle accident survivor sample. Pers Individ Differ. 2016;101(1):456–61. doi:10.1016/j.paid.2016.06.055. [Google Scholar] [CrossRef]
30. Tomich PL, DeMalio IS, Tolich A. Seek balance: deviation from balance mediates trauma exposure and quality of life. J Loss Trauma. 2021;27(5):448–60. doi:10.1080/15325024.2021.2005329. [Google Scholar] [CrossRef]
31. Tomich PL, Tolich A, DeMalio I. Strive for balance: deviation from a balanced time perspective mediates the relationship between lifetime trauma exposure and PTSD symptoms. Curr Psychol. 2021;41(11):8103–11. doi:10.1007/s12144-020-01254-6. [Google Scholar] [CrossRef]
32. Lazarus RS, Folkman S. Stress, appraisal, and coping. In: Gellman MD, Turner JR. Encyclopedia of behavioral medicine. Springer Publishing Company. 1984. doi: 10.1007/978-1-4419-1005-9_215 [Google Scholar] [CrossRef]
33. Zou M, Liu B, Ji J, Ren L, Wang X, Li F. The relationship between negative coping styles, psychological resilience, and positive coping styles in military personnel: a cross-lagged analysis. Psychol Res Behav Manag. 2024;17:13–21. doi:10.2147/prbm.S447096. [Google Scholar] [PubMed] [CrossRef]
34. Ishwari AB, Bhagawati KC. Post traumatic stress disorder and coping strategies among adult survivors of earthquake, Nepal. BMC Psychiat. 2019;19(1):441. doi:10.1186/s12888-019-2090-y. [Google Scholar] [PubMed] [CrossRef]
35. Liao YG. Relationship between coping style and mental health: a meta-analysis. Chin J Clin Psychol. 2014;22(5) (In Chinese). doi:10.16128/j.cnki.1005-3611.2014.05.078. [Google Scholar] [CrossRef]
36. Foster S, Estévez-Lamorte N, Walitza S, Dzemaili S, Mohler-Kuo M. Perceived stress, coping strategies, and mental health status among adolescents during the COVID-19 pandemic in Switzerland: a longitudinal study. Eur Child Adolesc Psychiatry. 2022;32(6):937–49. doi:10.1007/s00787-022-02119-y. [Google Scholar] [PubMed] [CrossRef]
37. Li SS, Zhang JY, Wu CW, Lu YW, Xu LJ, Ni YY, et al. The mediating effect of coping style on the relationship between perceived stress and mental health in Chinese rural older adults living alone: a cross-sectional study. Geriatr Gerontol Int. 2022;22(7):523–8. doi:10.1111/ggi.14392. [Google Scholar] [PubMed] [CrossRef]
38. Rogowska A, Kuśnierz C, Ochnik D. Changes in stress, coping styles, and life satisfaction between the first and second waves of the COVID-19 pandemic: a longitudinal cross-lagged study in a sample of university students. J Clin Med. 2021;10(17):4025. doi:10.3390/jcm10174025. [Google Scholar] [PubMed] [CrossRef]
39. Cho J, Lee J. An integrated model of risk and risk-reducing strategies. J Bus Res. 2006;59(1):112–20. doi:10.1016/j.jbusres.2005.03.006. [Google Scholar] [CrossRef]
40. Li X, Lyu H. Perceived stress, and mental health during COVID-19 pandemic: a moderated mediating model. Front Psychol. 2021;11:77. doi:10.3389/fpsyg.2020.563741. [Google Scholar] [CrossRef]
41. Cunningham KF, Zhang JW, Howell RT. Time perspectives and subjective well-being: a dual pathway framework, time perspective theory. In: Stolarski M, Fieulaine N, van Beek W, editors. Time perspective theory; Review, research, and application. Cham: Springer; 2015. p. 403–15. [Google Scholar]
42. Dai BJ, Zhang GH. On the relationship between college students’ time perspective and anxiety: the mediating effect of coping styles. Chin J Spec Educ. 2011(8):77–80 (In Chinese). [Google Scholar]
43. Xu H, Wang Z, Peng L, Mi Y, Zeng P, Liu X. The study of psychological traits among Chinese college students during the COVID-19 campus lockdown. Front Psychol. 2022;13:1051770. doi:10.3389/fpsyg.2022.1051770. [Google Scholar] [PubMed] [CrossRef]
44. Saadeh H, Saadeh M, Almobaideen W, Al-Refaei A, Shewaikani N, Al-Fayez RQ, et al. Effect of COVID-19 quarantine on the sleep quality and the depressive symptom levels of university students in Jordan during the spring of 2020. Front Psychiat. 2021;12:605676. doi:10.3389/fpsyt.2021.605676. [Google Scholar] [PubMed] [CrossRef]
45. Benzing V, Siegwart V, Anzeneder S, Spitzhüttl J, Grotzer M, Roebers CM, et al. The mediational role of executive functions for the relationship between motor ability and academic performance in pediatric cancer survivors. Psychol Sport Exerc. 2022;60(9):102160. doi:10.1016/j.psychsport.2022.102160. [Google Scholar] [CrossRef]
46. Li R, Bunke S, Psouni E. Attachment relationships and physical activity in adolescents: the mediation role of physical self-concept. Psychol Sport Exerc. 2016;22(4):160–9. doi:10.1016/j.psychsport.2015.07.003. [Google Scholar] [CrossRef]
47. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–91. [Google Scholar] [PubMed]
48. Li Q, Hu J, Wan P. Serial multiple mediation of the relationship between positive coping style and post-traumatic growth among Chinese college students in the aftermath of COVID-19. Int J Ment Health Promotion. 2023;25(11):1173–86. doi:10.32604/ijmhp.2023.030343. [Google Scholar] [CrossRef]
49. Dai YJ, Hao YH, Wu QH. Establishment and evaluation on reliability and validity of public risk perception scale for public health emergencies. Chin J Public Health. 2020;36(2):227–31 (In Chinese). doi:10.11847/zgggws1119744. [Google Scholar] [CrossRef]
50. Wang C. Time perspective: the revision of the inventory and the influence on risky driving behavior (Master’s Dissertation). Southwest University: China; 2016 (In Chinese). [Google Scholar]
51. Li X, Lyu H. The effect of the subjective social status on well-being: mediating role of balancing time perspective. Chin J Clin Psychol. 2021;30(1):116–20 (In Chinese). doi:10.16128/j.cnki.1005-3611.2022.01.024. [Google Scholar] [CrossRef]
52. Xie Y. Reliability and validity of the simplified coping style questionnaire. Chin J Clin Psychol. 1998;6(2):114–5 (In Chinese). doi:10.13342/j.cnki.cjcp.2022.10.023. [Google Scholar] [CrossRef]
53. Chen JH, Tong KK, Su X, Yu EW, Wu AMS. Measuring COVID-19 related anxiety and obsession: validation of the coronavirus anxiety scale and the obsession with COVID-19 scale in a probability Chinese sample. J Affect Disord. 2021;295(5):1131–7. doi:10.1016/j.jad.2021.08.104. [Google Scholar] [PubMed] [CrossRef]
54. Tsai FJ, Huang YH, Liu HC, Huang KY, Huang YH, Liu SI. Patient health questionnaire for school-based depression screening among Chinese adolescents. Pediatrics. 2014;133(2):e402–9. doi:10.1542/peds.2013-0204. [Google Scholar] [PubMed] [CrossRef]
55. Kim HY. Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restor Dent Endod. 2013;38(1):52–4. doi:10.5395/rde.2013.38.1.52. [Google Scholar] [PubMed] [CrossRef]
56. Wang XL, Gao LY, Miu QF, Dong XD, Jiang XM, Su SM, et al. Perceived uncertainty stress and its predictors among residents in China during the COVID-19 pandemic. Psychol, Health & Med. 2020;27(1):265–79. doi:10.1080/13548506.2021.1883692. [Google Scholar] [PubMed] [CrossRef]
57. Schimmack U, Radhakrishnan P, Oishi S, Dzokoto V, Ahadi S. Culture, personality, and subjective well-being: integrating process models of life satisfaction. J Pers Soc Psychol. 2002;82(4):582–93. doi:10.1037/0022-3514.82.4.582. [Google Scholar] [CrossRef]
58. Stolarski M, Zajenkowski M, Jankowski KS, Kinga S. Deviation from the balanced time perspective: a systematic review of empirical relationships with psychological variables. Pers Individ Differ. 2020;156(2):109772. doi:10.1016/j.paid.2019.109772. [Google Scholar] [CrossRef]
59. Zhang HYT, Zhang BS, Jin D, Yao L. Perceived social support mediates the effects of residence identification on the sense of control in older adults: a longitudinal model. Stud Psychol Behav. 2020;18:854–60 (In Chinese). [Google Scholar]
60. Pagnini F, Bercovitz K, Langer E. Perceived control and mindfulness: implications for clinical practice. J Psychother Integr. 2016;26(2):91–102. doi:10.1037/int0000035. [Google Scholar] [CrossRef]
61. Li L, Cao H, Yang L, Yan C, Wang X, Ma Y. Risk perception and mental health among college students in China during the COVID-19 pandemic: a moderated mediation model. Front Psychiat. 2022;13:955093. doi:10.3389/fpsyt.2022.955093. [Google Scholar] [PubMed] [CrossRef]
62. Infurna FJ, Gerstorf D, Ram N, Schupp J, Wagner GG. Long-term antecedents and outcomes of perceived control. Psychol Aging. 2011;26(3):559–75. doi:10.1037/a0022890. [Google Scholar] [PubMed] [CrossRef]
63. Park CL, Folkman S, Bostrom A. Appraisals of controllability and coping in caregivers and HIV+ men: testing the goodness-of-fit hypothesis. J Consult Clin Psychol. 2001;69(3):481–8. doi:10.1037/0022-006X.69.3.481. [Google Scholar] [PubMed] [CrossRef]
64. Zhang W, Cao XH, Du J, Wang N, Zhao M, Lin JC. Analysis of coping capacity and influencing factors of public health emergencies among college students in Shandong Province. Chin J School Health. 2022;43(4):514–7 (In Chinese). doi:10.16835/j.cnki.1000-9817.2022.04.008. [Google Scholar] [CrossRef]
65. Knoll N, Rieckmann N, Schwarzer R. Coping as a mediator between personality and stress outcomes: a longitudinal study with cataract surgery patients. Eur J Pers. 2005;19(3):1–19. doi:10.1002/per.546. [Google Scholar] [CrossRef]
66. Doron J, Trouillet R, Gana K, Boiché J, Neveu D, Ninot G. Examination of the hierarchical structure of the BRIEF COPE in a French sample: empirical and theoretical convergences. J Pers Assess. 2014;96:567–75. doi:10.1080/00223891.2014.886255. [Google Scholar] [PubMed] [CrossRef]
67. Stanislawski K. The coping circumplex model: an integrative model of the structure of coping with stress. Front Psychol. 2019;10:694. doi:10.3389/fpsyg.2019.00694. [Google Scholar] [PubMed] [CrossRef]
68. Li T. Comparative study on difference of time perspective between Chinese and Western countries. J Shenyang Univ Technol (Soc Sci Ed). 2016;9(4):381–4 (In Chinese). [Google Scholar]
69. Fu AG, Wen PC, Wu N, Yue T. Qualitative research into the “time perspective” of Chinese people. J Suzhou Univ. 2024;1:107–18 (In Chinese). doi:10.19563/j.cnki.sdik.2024.01.011. [Google Scholar] [CrossRef]
70. Chen T, Liu LL, Cui JF, Qin XJ, Gan MY, Tan SP, et al. Dynamic attention regulation for prospective goals in Schizophrenia. Clin Psychol Sci. 2021;9(6):1035–44. doi:10.1177/21677026211004543. [Google Scholar] [CrossRef]
71. Zheng X, Wang W. Time perspective in the self-regulatory mechanism of meaning in life. J Happiness Stud. 2022;23(2):747–67. doi:10.1007/s10902-021-00424-y. [Google Scholar] [CrossRef]
72. Han J, Lee H, Ohtsubo Y, Masuda T. Culture and stress coping: cultural variations in the endorsement of primary and secondary control coping for daily stress across European Canadians, East Asian Canadians, and the Japanese. Jpn Psychol Res. 2022;64(2):141–55. doi:10.1111/jpr.12406. [Google Scholar] [CrossRef]
73. Gross JJ. Emotion regulation: taking stock and moving forward. Emotion. 2013;13(3):369–75. doi:10.1037/a0032135. [Google Scholar] [PubMed] [CrossRef]
74. Selby EA, Joiner TE. Emotional cascades as prospective predictors of dysregulated behaviors in borderline personality disorder. Personal Disord: Theory, Res, Treat. 2013;4(2):168–74. doi:10.1037/a0029933. [Google Scholar] [PubMed] [CrossRef]
75. Deng X, Ding X, Sang B. The application of experience sampling method and its advantages in emotion regulation research. J East China Normal Univ (Educ Sci). 2015;33(1):77–83 (In Chinese). doi:10.16382/j.cnki.1000-5560.2015.01.003. [Google Scholar] [CrossRef]
76. Bergman LR, Magnusson D, El Khouri BM. Studying individual development in an interindividual context: a person-oriented approach. Mahwah, NJ: Psychology Press; 2003. [Google Scholar]
77. Sun H, Tao J, Xu H, Dong C. Latent profile analysis of community residents’ risk perception in public health emergencies. J Wenzhou Med Univ. 2023;53(7):595–602 (In Chinese). doi:10.3969/j.issn.2095-9400.2023.07.011. [Google Scholar] [CrossRef]
78. Zhou H, Li GJ, Li CB, Zhu ZY. Esearch progress on the relationship between emotion regulation strategies and mental disorders in the eastern and western cultures. J Neurosci Mental Health. 2020;20(6):425–30. doi:10.3969/j.issn.1009-6574.2020.06.010. [Google Scholar] [CrossRef]
79. Sword RM, Sword RKM, Brunskill SR, Zimbardo PG. Time perspective therapy: a new time-based metaphor therapy for PTSD. J Loss Trauma. 2014;19(3):197–201. doi:10.1080/15325024.2013.763632. [Google Scholar] [CrossRef]
80. Hu CH, Wang Q, Zhong D, Jiang D. Effect of using satir model group psychological intervention on improving the coping style of college students. China J Health Psychol. 2022;30(10):100–20 (In Chinese). doi:10.13342/j.cnki.cjhp.2022.10.023. [Google Scholar] [CrossRef]
81. He L, Shi Z. Intervention studies based on the strength model of self-control: a review. Chin Mental Health J. 2015;29(5):366–71 (In Chinese). doi:10.3969/j.issn.1000-6729.2015.05.012. [Google Scholar] [CrossRef]
82. Li Y. The state hope mentality of college students and intervention (Doctoral Dissertation). East China Normal University: China; 2017 (In Chinese). [Google Scholar]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools