
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE
Research on the Effect of Dance Therapy on Improving Social Communication Ability of Children with Autism
1 Institute of Education, Xinyang University, Xinyang, 464000, China
2 Hengshui College Conservatory of Music, Hengshui, 053000, China
* Corresponding Author: Shan Wang. Email:
(This article belongs to the Special Issue: Mental Health and Social Development)
International Journal of Mental Health Promotion 2024, 26(5), 407-416. https://doi.org/10.32604/ijmhp.2023.030135
Received 23 March 2023; Accepted 07 June 2023; Issue published 30 May 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Research motivation: Through the 12 weeks dance therapy intervention for children with autism, the purpose is to explore the intervention model of dance therapy for children with autism and the changes in motor ability, social ability, and communication ability of children with autism after dance therapy intervention. The results of the research are expected to expand the intervention mode of dance therapy in my country and provide practical reference for rehabilitation intervention of children with autism. Research methods: 24 autistic boys aged 6 to 12 with mild to moderate symptoms were recruited and screened through the Internet as the subjects of this study. We randomly divided them into experimental group (N = 12) and control group (N = 12). All children with autism have an autism diagnosis certificate issued by Children’s Hospital or a tertiary hospital, excluding other mental diseases (such as epilepsy, major physical disability, mental illness, no history of drugs and other interventions, etc.). We used the paired sample t-test to compare the score difference between the dance treatment group and the control group before and after the two groups, and used the observation method to record the basic communication behavior and the number of active communication behaviors in the experimental group during the intervention process. All data analysis is used in SPSS 20.0. Research results: After 12 weeks of dance therapy intervention, there were statistically significant differences in the gross movement, balance, and coordination abilities of the children in the experimental group compared with those before the intervention (p < 0.01). There was no significant difference between the children in the control group (p > 0.05). After 12 weeks of dance therapy intervention, there were statistically significant differences in the scores of the social response scale for children with autism in the experimental group (p < 0.05). There was no significant change in the scores of each item of the SRS scale before and after intervention in the control group and the dance treatment group (p > 0.05).Keywords
Autism Spectrum Disorder (ASD) is a group of neurodevelopmental dysfunction disorders mainly characterized by restricted interests or repetitive behaviors and difficulties in social communication [1], and its related symptoms will accompany patients throughout their lives. At present, autism has been recognized as one of the most common developmental disorders in children. According to the latest data released by the Centers for Disease Control and Prevention in the United States in 2021, there is one in every 44 8-year-old children with autism, and the incidence rate for males is 4.2 times that of women [2]. As a country with a large population base, according to incomplete statistics, the number of autistic people in China has reached 10 million, of which the number of children has reached 2 million and the number is increasing by 200,000 every year [3]. In response to the increasing prevalence of autism, China has introduced a series of subsidy policies related to autism [4] and established a prescription library for the integration of sports and medicine to further develop health services for the whole society [5].
In response to autism, a global public health problem, researchers from all walks of life are actively exploring the recovery effects of different intervention methods on autistic people. Common intervention methods include applied behavior analysis, exercise intervention, structured teaching, and game therapy. The above-mentioned intervention methods are mainly aimed at improving the related defects of children with autism. Although there are relevant data to support their effectiveness [6–8], they ignore the advantages and abilities of children with autism in some aspects. For example, the attention advantage of objects [9], the tone perception advantage [10], etc. The physical and mental relationship and creativity emphasized by dance therapy can guide individuals to establish behavioral spontaneity and self-control, make full use of the advantages of autistic children, improve the individual’s sense of boundaries and communication skills, and thus establish behavioral choices and methods that are beneficial to a healthy life [11].
Dance Movement Therapy (DMT), also known as dance/movement therapy, promotes the development of individual social, communication, and basic motor skills through movement methods and non-verbal and creative strategies. Dance therapy is unique from traditional psychotherapy in that it emphasizes the interconnectedness of the emotional and physical bodies, as well as the ability of creativity to promote mental health. On the physical level, dance therapy helps people strengthen their coordination and improve their physical fitness. On the emotional level, dance therapy helps people become more joyful and confident, and gives people therapeutic methods and tools to express various emotions that cannot or cannot be expressed enough through language. Dance therapy can improve a person’s cognitive abilities, motivation and memory. Until now, dance therapy has been shown to have a positive effect on specific child mental health interventions or psychotherapy [12]. Especially with the implementation of the important national strategies of “Healthy China” and “Sports Power”, dance therapy, which is regarded as a “non-medical health intervention” method, has attracted more and more attention [13]. Based on the background of China’s relevant policy strategies and the growing rehabilitation needs of autism, this study explores the intervention effect of dance therapy on related symptoms of autistic children, in order to provide a necessary practical reference for autistic children to enter the society.
In western developed countries, the effectiveness of dance therapy intervention has been confirmed theoretically and empirically, but domestic theoretical research on DMT intervention is still relatively scarce. Based on drawing lessons from foreign theories, this study uses dance therapy to intervene in the movement ability, social and communication abilities of children with autism, in order to explore and enrich the DMT intervention theory in China. The application of dance therapy in autism rehabilitation treatment is conducive to creating a good classroom interactive environment, stimulating children’s enthusiasm and initiative in learning, and cultivating autistic children’s interest in learning. This paper uses dance therapy to intervene in the movement ability, social and communication skills of children with autism, and provides important references for families and children with autism.
Correlative research on movement disorders in children with autism
Children with autism generally have deficits in motor skills, and the early detection of motor dysfunction in autistic individuals is due to the failure of personal body regulation [14]. Symptoms of motor dysfunction appear in infancy, mainly including abnormal balance, abnormal coordination, gross and fine movements [15–17]. Autistic children have abnormal balance. Developmental disorders caused by hypotonia and excessive laxity of ligaments [18], which are mainly manifested in postural control, walking, etc. In terms of postural control, Lim et al. [19] found that autistic children have sensory integration deficits by comparing postural control among individuals with autism. Studies have shown that children with autism are prone to postural instability. Travers et al. [20] conducted a balance test on 21 autistic children. During the test, the autistic children swayed on an uneven slope and could not maintain a stable posture. Postural stability is determined by IQ in children with autism, and their walking is abnormal, the study found. In terms of walking, Gong et al. [21] tested the plantar pressure of 58 autistic children aged 4–6, and found that autistic children had abnormal gait characteristics such as left-right asymmetry and large stride changes when walking. Martin et al. [22] found abnormal gait in children with autism, including toe walking, stride length and duration, incoordination, and abnormal head and trunk positioning.
Children with autism have abnormal coordination skills. The coordination ability of autistic children is a milestone in the development of gross and fine motors, and it is more difficult for autistic children with coordination impairment to participate in motor activities than normal children. Dewey et al. [16] intervened 49 autistic children aged 5–18. Studies have found that when children with autism follow commands and perform gesture operations, they have wrong movements and directions, resulting in impaired coordination. Fournier et al. [15] found that autistic children have severe motor coordination deficits through the study of autistic children’s motor coordination, indicating that their symptoms are the main characteristics of autistic children. Dyck et al. [23] evaluated 29 children with autism aged 4–13 in terms of motor coordination, intelligence, and language. Children with autism show significant impairments in IQ and motor coordination on measures of ability. The study found that 86% of children with autism were associated with symptoms of social interaction, motor coordination and receptive language.
Abnormal development of gross motor abilities in children with autism. Gross motor deficits are present early on. Infants exhibit difficulty in crawling and walking, but as they grow older, autistic children have problems with basic motor control [24]. Green et al. [17] evaluated 101 autistic children with an average age of 10 years using the Children’s Motor Assessment Kit (M-ABC), and found that 79% of autistic children had obvious coordination impairments. Staples et al. [25] tested the motor development ability of 25 autistic children aged 9–12 with the second version of the Gross Motor Development Ability Test (TGMD-2), and found that the gross motor skills of autistic children were worse than expected, and children with autism also have delayed response defects. Mayer et al. [26] used the Early Learning Scale to test 87 infants aged 6–24 months. The study found that at 24 months of age, the ASD group performed worse than normal children in all domains, including gross motor, fine motor, and receptive language.
Research on social and communication barriers of children with autism
Autistic children have difficulty establishing and maintaining appropriate interpersonal relationships due to the core symptom of social impairment. Moreover, autism is a developmental disorder of the nervous system, and abnormal attention, social behavior, and social interaction of individual children will further affect their social skills. Chevallier et al. [27] found that children with autism showed obvious abnormal social behaviors such as lack of facial expressions and eye gaze when they were about 1 year old after birth. However, during the school-age period, children with autism show that it is difficult to establish and maintain stable partnerships with others, and they will not have intimate interactions with those around them. Even in the game session, children with autism rarely play group games with other children. In addition, compared with normal children, such groups lack attachment to family members. For example, children with autism showed less disturbed behaviors after being separated from their families, but they also rarely showed happy and excited behaviors when their families returned.
Social attention deficits are mainly manifested as abnormal eye contact, distraction or extreme concentration that cannot be effectively shifted, difficulty in shifting attention, difficulty in distribution of attention, and small span of attention. Freeman et al. [28] believed that children with autism had visual attention difficulties and abnormal visual communication activities during social activities, which resulted in children with autism being unable to properly obtain external information and hindering individuals from learning effective social cues. These affect the development of social interaction skills in children with autism [29]. In addition, the reduction of social joint attention plays an important role in explaining the occurrence and pathogenesis of autism. Social attention is the condition for individuals to carry out cognitive learning and shape behavior. Its normal development is conducive to individual imitation, interpersonal interaction, games, etc., but the delay or lack of development will seriously affect the social interaction of autistic children [30]. Therefore, the improvement of social attention of children with autism has positive significance for the development of their social ability.
Deficiency in self-awareness makes autistic individuals unable to accurately understand the relationship between their own body, mental activities, and the world around them, which is also an important reason for social impairment. Its main manifestation is selective damage, that is, the physical self-awareness is intact, while the psychological self-awareness is damaged. From a developmental point of view, normal children begin to be interested in themselves in the mirror at about 6–12 months of age, begin to have self-awareness at about 18–24 months, and begin to have delayed mirror self-awareness at about 3–5 years old Capabilities [31]. However, with the growth of age, a relatively advanced self-cognition ability is gradually formed. The self-awareness defect of autistic children cannot form a proper understanding of self-psychology and other people’s minds, and has a negative impact on the development of their normal social skills.
Communication deficit is one of the core symptoms of children with autism, mainly including lack of active communication, responding to others’ communication and participating in dialogue. It is characterized by inability to use verbal and non-verbal communication normally, lack of communication skills, lack of communication awareness of initiative and response, inability to communicate with others through normal eye contact and body communication, and strange tone of voice. From the perspective of the early development of emotional faces, normal children can have different differences between gaze and emotional faces when they are about 4 months old. At about 7 months, facial expressions can be distinguished and directional and habitual responses can be made to the same or different faces [32,33]. With the growth of age, the expression task can be completed proficiently at around 4 years old [34]. Children with autism lack emotional interaction and sharing, and cannot properly express their feelings and correctly use non-verbal behaviors to communicate and interact. The defect in the development of language function is the main pain point of communication problems in children with autism. Foreign studies have shown that more than half of children with autism have never developed a functional language during their growth [35], mainly manifested in the inability to use language as a tool for communication.
Compared with normal children, the language development rate of children with autism is significantly lower. Children with autism often ask others to meet their own needs through actions or postures, and it is difficult to use language to express. In addition, children with autism also have abnormalities in grammar, semantics and pragmatics. Some children with autism remain silent all their lives and do not use language to communicate. Although other children with autism have certain language skills, it is difficult for them to actively ask questions and obtain information like normal children. They are also unable to respond and interact in communicative situations. Children with autism have difficulty making eye contact with others, abnormal facial expressions, and non-verbal behaviors such as not understanding other people’s body language and gestures in communication activities. As a result, many autistics have problematic styles and skills in relating to others. In the absence of intervention, children with autism develop aggression, self-injury, emotional instability, and destructiveness as they age.
We recruited 25 autistic boys by sending questionnaires. His condition is mild, mild to moderate, and he has no other congenital diseases, severe respiratory diseases, no history of drug intervention, and no intervention training within half a year. Excluding one autistic child with data loss, the final effective subjects were 24 people, the average age of the participants was 8 years old, and the age range was 6–12 years old. There are 17 children who are only children, accounting for 70% of the total. 20 families are from the city, accounting for 83% of the total. There were 22 participants who were raised by their mothers, accounting for 91% of the total. The subjects were divided into two groups, an experimental group and a control group. All the subjects held a certificate of autism diagnosis issued by the hospital, the degree was mild or moderate, and they did not suffer from other diseases, and had not received intervention training within half a year. Parents signed the informed consent before the experiment.
We finely classify them and lay a theoretical foundation for the smooth progress of subsequent experimental research.
During the intervention phase, each child’s 80-min classroom communication behavior was observed and recorded, and with the consent of the parents, two cameras were used to record the whole process from different angles to obtain video data. Formulate the “Communication Behavior Record Form”, which mainly includes “observed person, number of observations, active eye contact, active body movements, active language behavior, inappropriate communication” and so on. After class, watch the subjects’ classroom video recordings and record the number of two video behaviors. Eye gaze is defined as eye behavior for more than two seconds, and one time is recorded; body movement is defined as communicating with others through physical means, and language is defined as speaking. Take the initiative to express ideas with others and remember 1 time. Record the number of active communication behaviors of the observed persons in the 2 videos, and record the change trend of communication behaviors. The researchers and team members used the same data collection procedure, and conducted consistency checks with the records of team members. The data was recorded only when the observation consistency percentage reached more than 90%, otherwise the third person watched again as the final value. The formula for the reliability test is: inter-observer agreement percentage = number of observed consistency ÷ (number of consistency + number of inconsistency) × 100%. The observation consistency percentages were all above 90%, indicating that the inter-observer consistency reliability was high.
The interview time for this study was from September 21, 2020 to January 10, 2023, and 25 parents of children with autism were interviewed. In the specific interview process, considering the convenience of the interview, two interview methods, online and offline, were mainly adopted. The offline interview was conducted at the Autism Sports Intervention Research Center, and the online interview was mainly conducted by telephone according to the free time of the interviewees. The interview time was 40–60 min, and the principle of informed consent was strictly followed, and the interviewees were asked to sign an informed consent form.
We have a solid understanding of the relevant background of each family, the personality and characteristics of children with autism, and their rehabilitation education. We recorded the needs of parents for rehabilitation intervention, and learned about the daily movement ability, social and communication behavior of children with autism, which provided a useful basis for the formulation of intervention plans and the selection of strategies for this study.
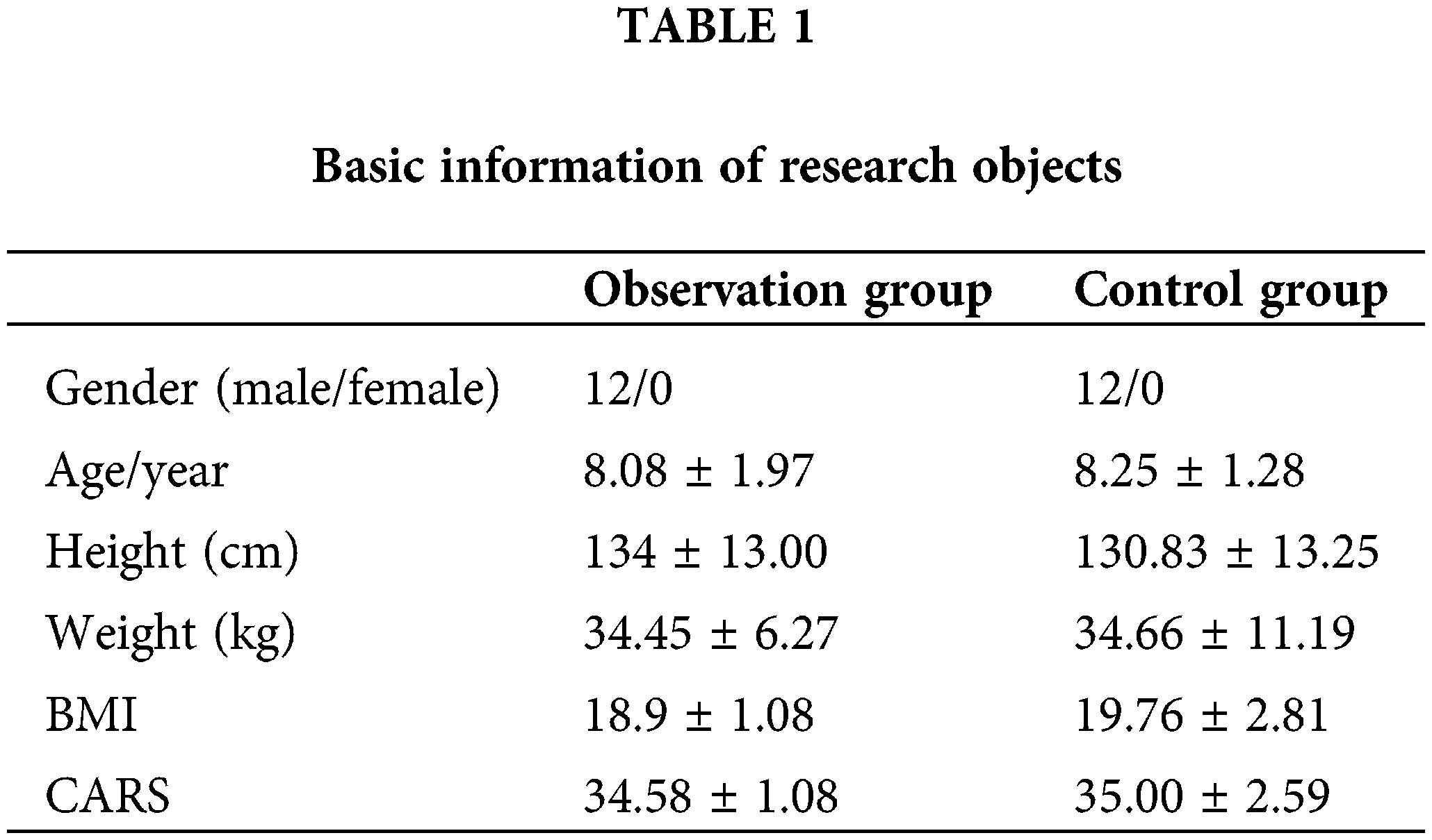
In this study, 24 autistic children in Nanjing were selected as the research partner, and their inclusion criteria were: (1) aged 6–12 years; (2) autism diagnosis certificate issued by a tertiary hospital; (3) 24 children Autistic subjects were randomly divided into experimental and control groups. None of the participating children had any training in dance. (4) The study was approved by Ethics Committee at the Xinyang University (IRB number: 20221005-APP-S). All participants signed the informed consent in this study (see Table 1).
The experimental tools used in this paper include CARS, TGMD-3 and SRS. Childhood Autism Rating Scale (CARS): It has good reliability and validity for identifying children with autism. It contains 15 items in total. The evaluation results include four levels: no autism, mild, moderate, and severe. The third edition of the Gross Motor Development Ability Test (TGMD-3) was compiled by Dr. Dale a Ulrich in the United States. It is an effective and reliable tool for assessing the development of gross motor skills in children aged 3–10 with normal development and children with special needs. It has a good reliability and validity. The scale is used to measure two types of basic motor skills: displacement skills (running, standing jump, hop, etc.) and object manipulation skills (catch the ball with both hands, kick the ball in situ, hit a fixed ball with both hands, pat the ball with one hand, etc.). These skills contain a total of 13 actions, and each item has 3–5 specific criteria, and one point is scored for each item. Each item is tested twice, and the total score is calculated by accumulating the scores of all items of displacement skills and object manipulation skills. The higher the score, the better the basic motor skills. The Social Responsiveness Scale (SRS) was used to assess the social impairment of autistic children aged 4–18. The internal consistency coefficient of the total scale is 0.95, the retest reliability is 0.96, and the reliability and validity are good. It is divided into 5 subscales of autism behavior, social motivation, social cognition, social perception and social communication, with a total of 65 items. Each item has 4 options to be filled in by parents or teachers. We then included the checked items on the scoring worksheet for scoring, with each item scoring on a scale of 0–3. A total score >60 points is diagnosed as autism, and the higher the score, the more serious the social impairment.
The specific experimental process in this paper is shown in Fig. 1. The experiment is divided into 3 stages. The first stage is the pre-test stage of the experiment. In this stage, the parents communicate with the parents and fill in the “Basic Information Registration Form for Children with Autism”, sign the informed consent form, and determine the research subjects. Various related scales were issued, and the pre-test evaluation was completed at the Autism Exercise Intervention Research Center of Nanjing Brain Hospital. The second stage is the dance therapy intervention stage. In this stage, children with autism in the experimental group receive dance therapy for 80 min three times a week. We use cameras to record the performance of children with autism during the intervention process. At the same time, we discuss with experts the problems that arise in the class during the intervention process, and communicate with parents after class to obtain suggestions, so as to make timely adjustments to the experiment. The third stage is the post-test stage of the experiment. In this stage, we distribute various related scales to parents and complete the post-evaluation in the Intervention Research Center. At the same time, watch the classroom video and record the changes in the daily communication behavior and active communication times of the children under test. Through interviews with parents and post-test evaluation results, we further analyzed whether there were any changes in the social, communication, and movement abilities of the subjects after the intervention, and provided follow-up supplements and demonstrations for the results of dance therapy research.
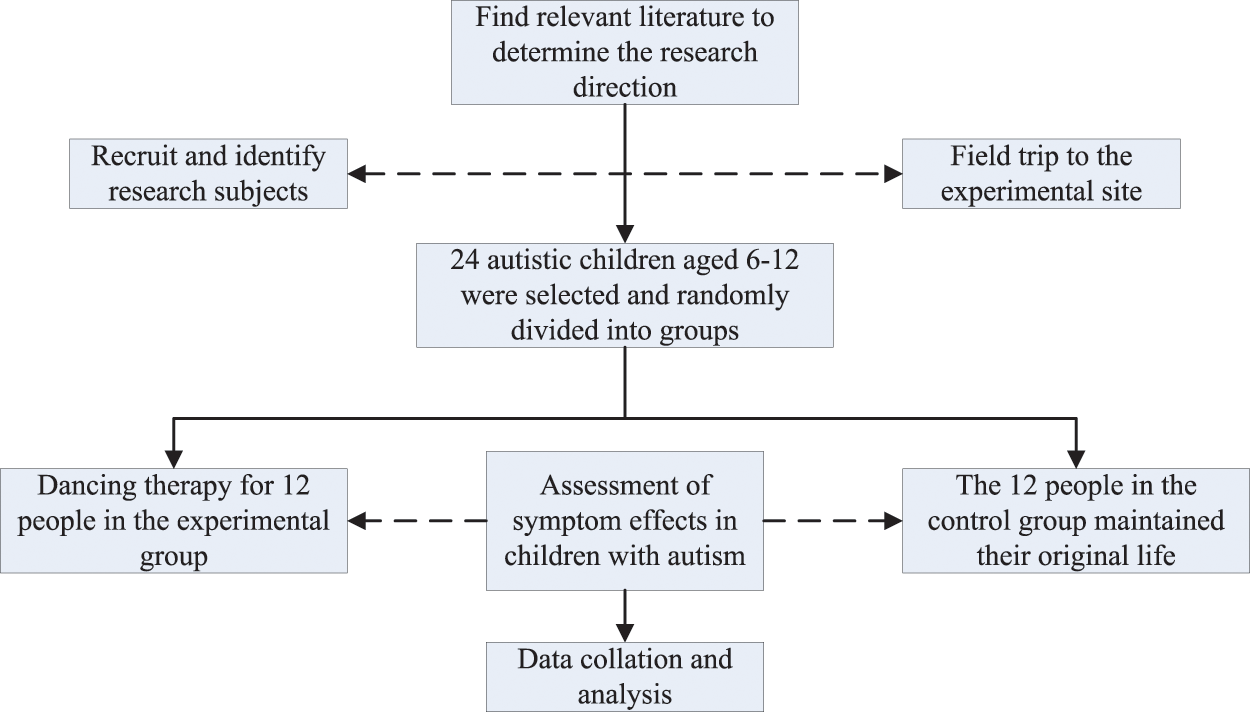
Figure 1: The flowchart of our experimental process.
We used SPSS 20.0 to analyze the data. After testing, all the data conformed to the normal distribution, expressed as mean ± standard deviation. The independent sample t-test was used for comparison between groups, the paired-sample t-test was used for comparison within a group, and Pearson’s two-sided correlation was used for correlation statistics. The significance level is p < 0.05.
Demographic and symptom differences of the children subjected
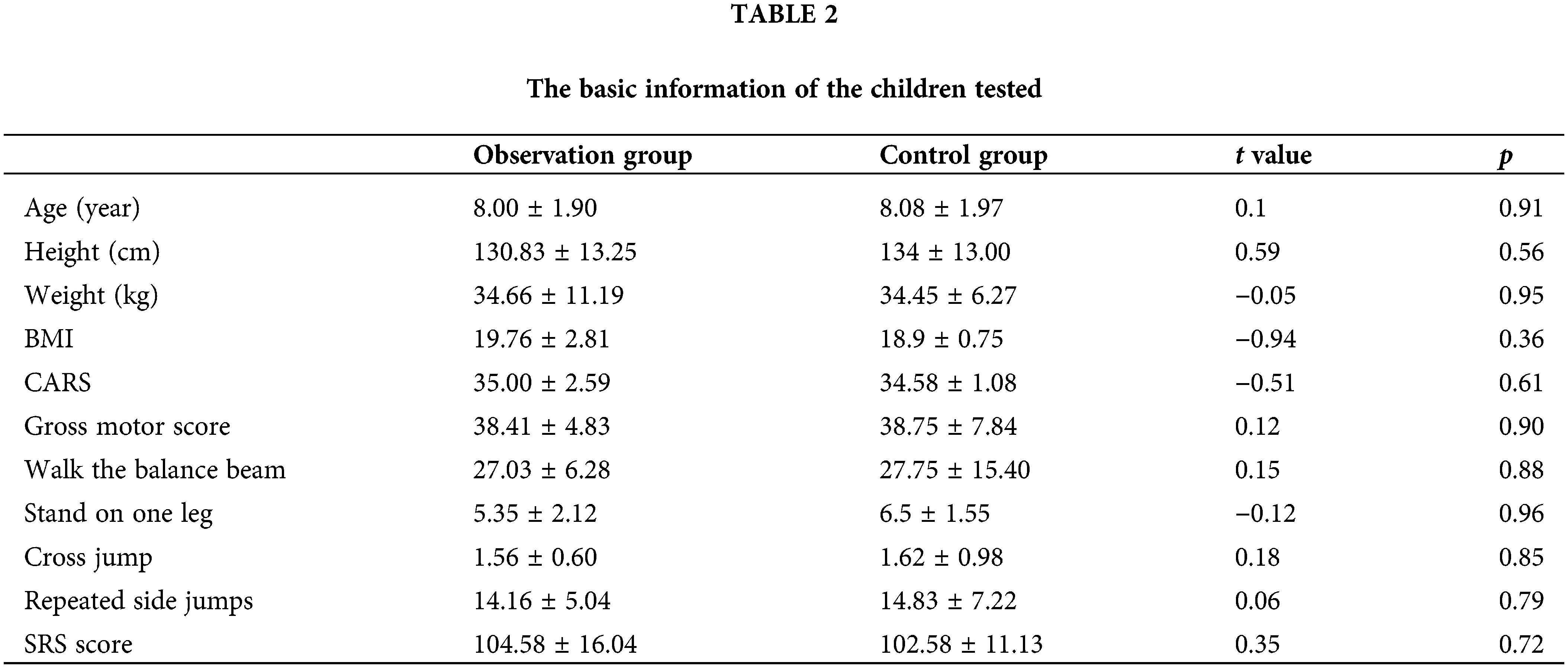
Depending on the level of development, the degree of symptoms can affect gross motor skills, balance, coordination, and social skills. As shown in Table 2, there was no statistical significance in the weight, age, height, gross movement, balance ability, coordination ability, and SRS score of children with autism in the two groups (p > 0.05).
Changes of the children’s displacement ability before and after the experiment
As shown in Table 3 and Fig. 2, there were statistically significant differences in the scores of displacement movement indicators such as running, horse trotting, single-leg hopping, running jump, standing jump, and side sliding step before and after the intervention in the experimental group (p < 0.01) was very significant. There was no statistically significant difference in the scores of displacement movement indicators such as running, horse trotting, single-leg hop, canter jump, standing jump, and side sliding step in the control group before and after the intervention (p > 0.05). There was no statistically significant difference in the scores of each item of the pre-test displacement movement between the two groups (p > 0.05), and the difference in the scores of each item of the post-test displacement movement between the two groups was statistically significant (p < 0.01), and the difference was very significant.
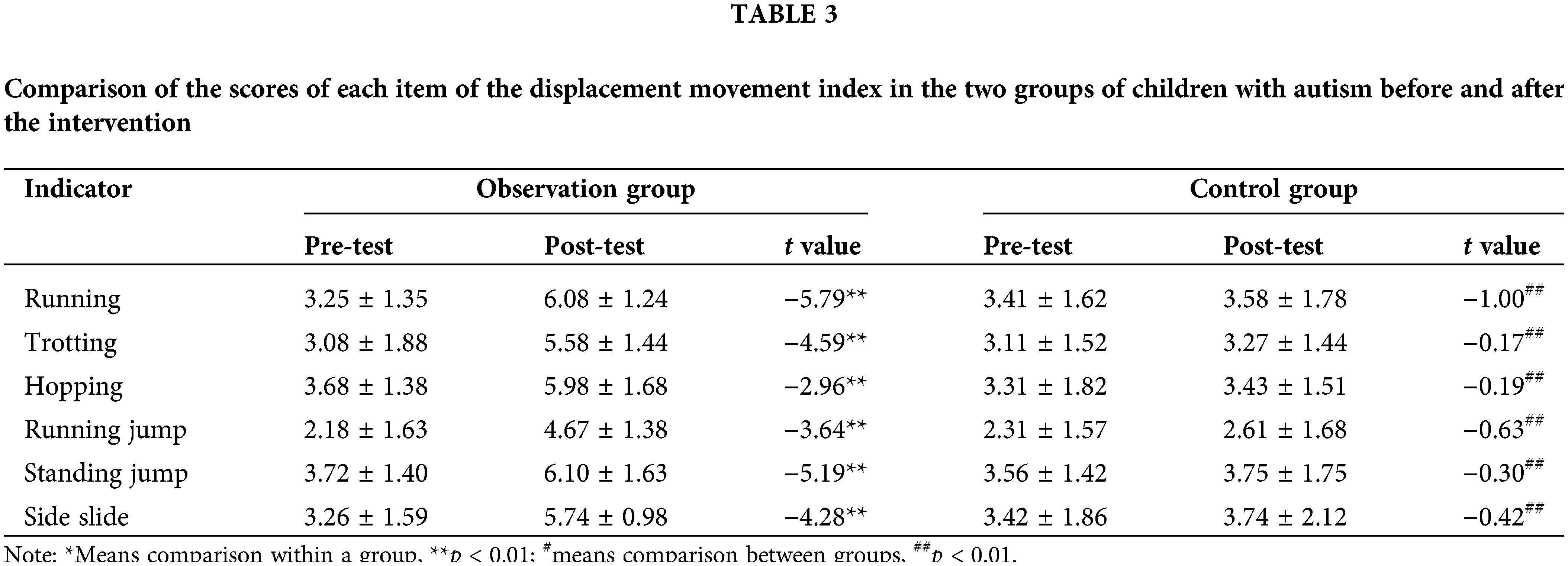
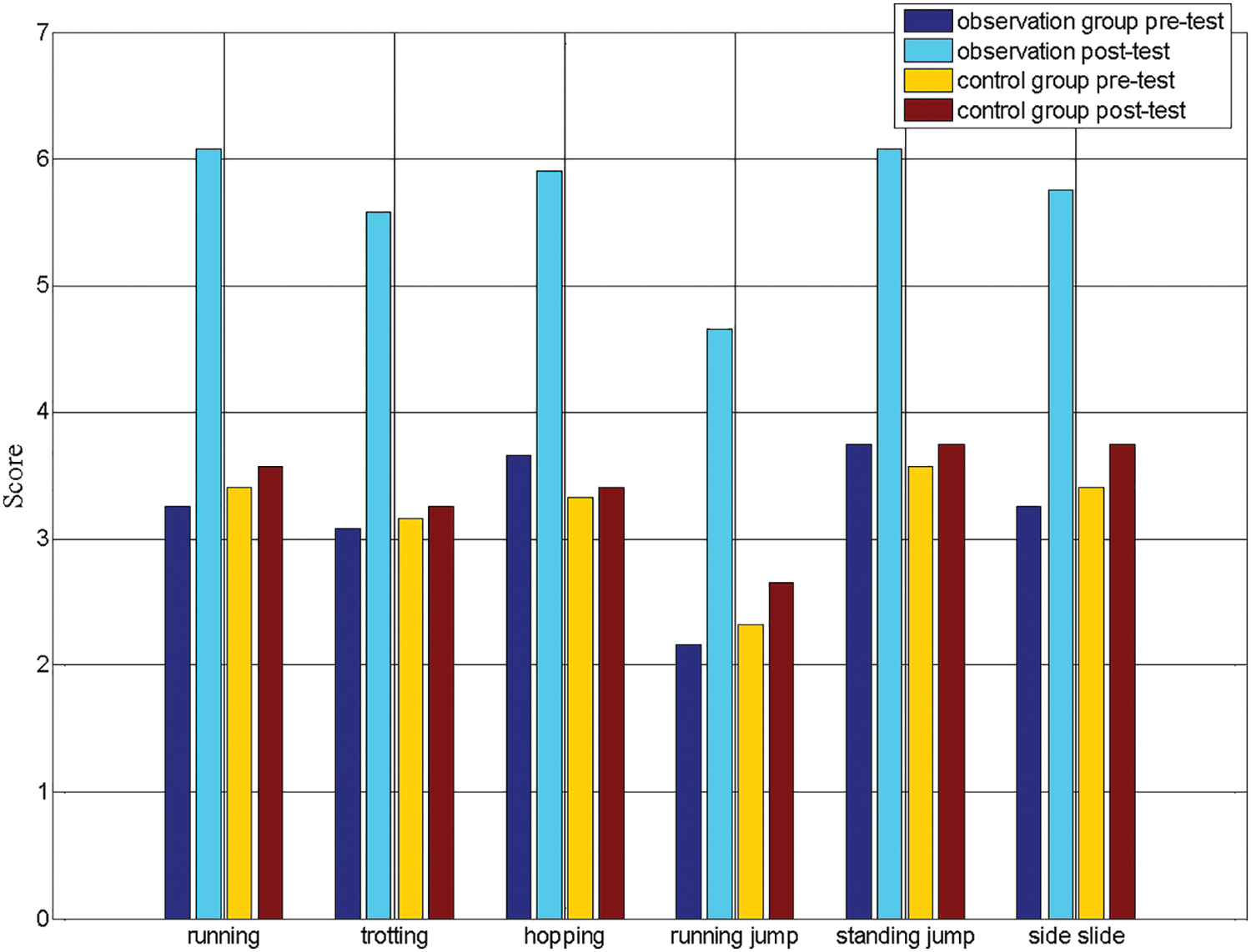
Figure 2: Changes in the scores of the displacement movements before and after the two groups of experiments.
As shown in Fig. 3, there were statistically significant differences in the scores of object manipulation indicators such as hitting the fixed ball, throwing the ball, hitting the ball with one hand, catching the ball with both hands, kicking the ball in place, throwing the ball with the overhand, and throwing the ball with the underhand before and after the intervention in the experimental group (p < 0.01), the difference is very significant. There was no statistically significant difference in the scores of the object manipulation ability before and after the intervention in the control group (p > 0.05). There was no statistically significant difference in the scores of each item of pre-test object manipulation between the two groups (p > 0.05), but there was statistically significant difference in the scores of each item of post-test object manipulation between the two groups (p < 0.01), and the difference was very significant.
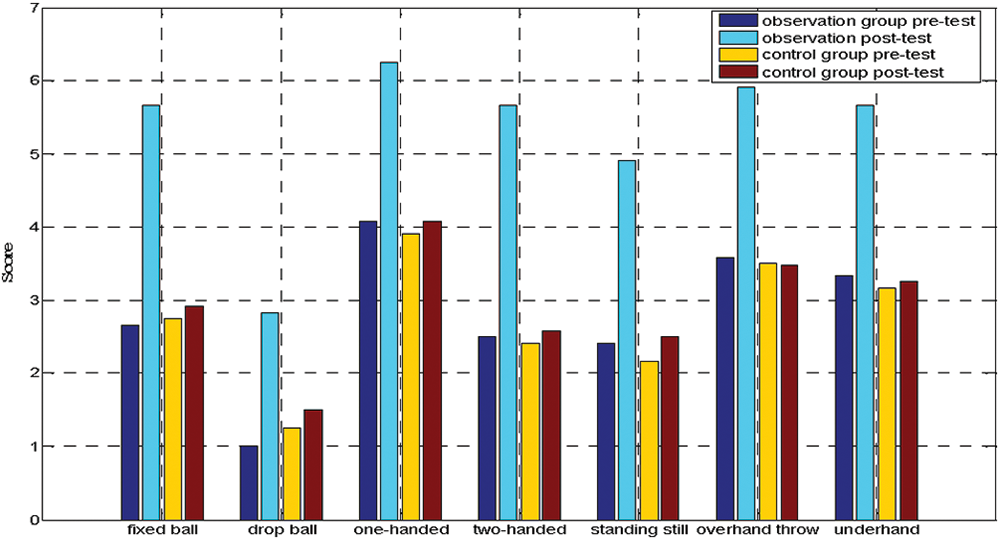
Figure 3: Changes in the scores of object manipulation items before and after the two groups of experiments.
Changes in the gross motor ability of the children before the experiment
As shown in Table 4 and Fig. 4, there were statistically significant differences in the total gross muscle score and the dimensions of displacement and object manipulation in the experimental group before and after the intervention (p < 0.01), and the difference was very significant. In the control group, there was no significant difference in the total score of gross muscle before and after the intervention, as well as the scores of displacement action and object manipulation action dimension (p > 0.05). There was no statistically significant difference in the scores of each item of gross motor in the pretest between the two groups (p > 0.05), but there was a statistically significant difference in the score of each item of gross motor in the posttest between the two groups (p < 0.01), and the difference was very significant.
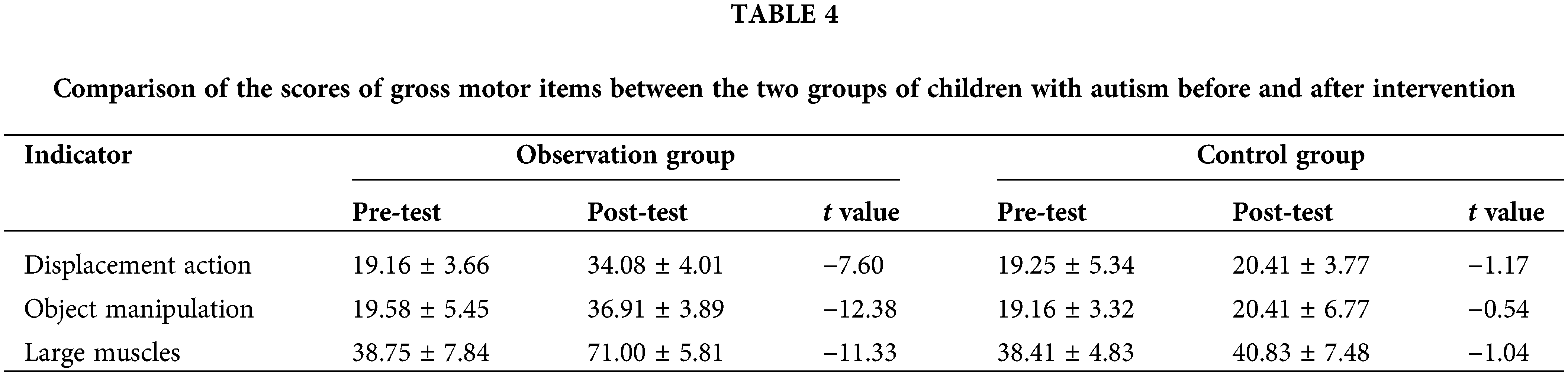
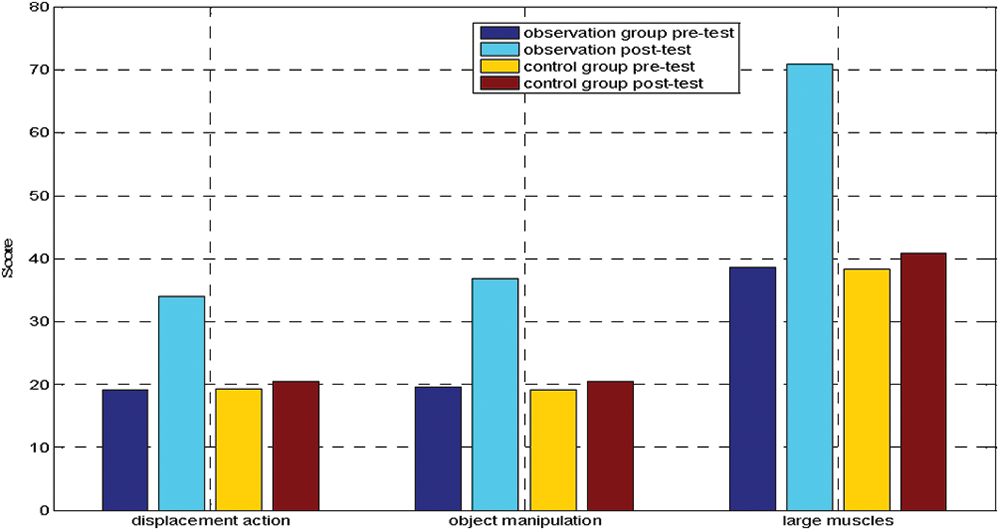
Figure 4: Changes of gross motor items before and after the two groups of experiments.
Good displacement movement development has a positive impact on physical fitness and the development of basic motor skills. The results of this study show that a 12 weeks dance therapy intervention can effectively improve the displacement movement ability of children with autism.
In this study, dance therapy was adopted, and the content of the intervention ranged from simple running and jumping to side-sliding steps, hops and other movement exercises, and the displacement movements were continuously developed, consolidated and strengthened. The results of the study show that dance therapy can promote the development of displacement movement ability of children with autism. Object manipulation skills refer to the ability to control the movement of objects in space. The results of this study show that a 12 weeks dance therapy intervention can effectively improve the object manipulation ability of children with autism.
Changes of the children’s balance ability before and after the experiment
As shown in Table 5 and Fig. 5, there were statistically significant differences (p < 0.01) in the scores of the balance ability indexes of walking on the balance beam and standing on one leg in the experimental group before and after the intervention, and the difference was very significant. There was no significant difference in the scores of two balance ability indexes of walking on the balance beam and standing on one leg in the control group before and after (p > 0.05). There was no statistically significant difference in the scores of each item of balance ability in the pretest between the two groups (p > 0.05), but there was statistically significant difference in the scores of each item in the posttest balance ability between the two groups (p < 0.01), and the difference was very significant.
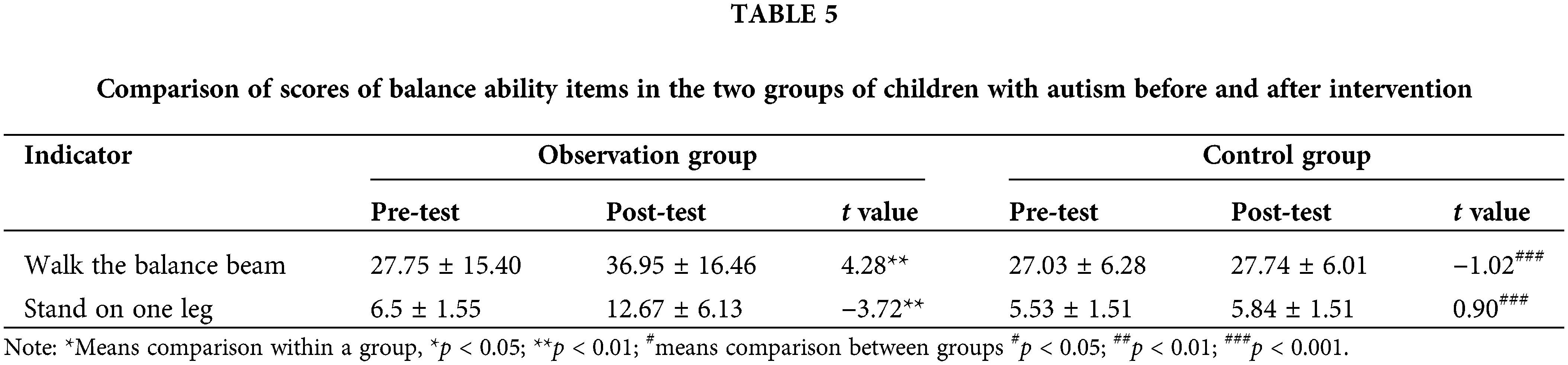
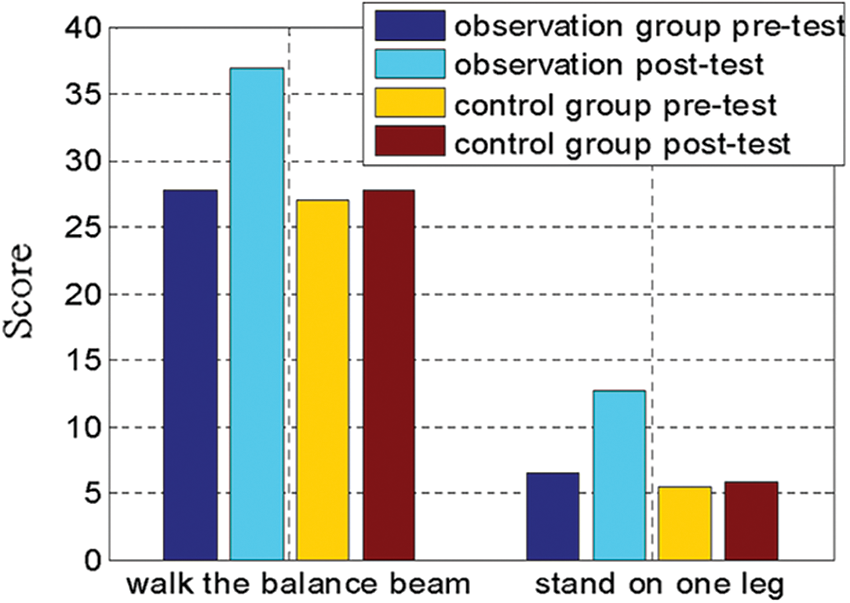
Figure 5: Balance and coordinate the changes of each item before and after the two groups of experiments.
Changes of the coordination ability of the children before and after the experiment
As shown in Table 6 and Fig. 6, there were statistically significant differences in the scores of the two coordination ability indexes of cross jumps and repeated side jumps before and after the intervention in the experimental group (p < 0.01), and the differences were very significant. In the control group, there was no statistical significance in the scores of cross jumps and repeated side jumps after intervention (p > 0.05). There was no statistically significant difference in the scores of the pre-test coordination items between the two groups (p > 0.05), and the differences in the scores of the post-test coordination items between the two groups were statistically significant (p < 0.01), and the difference was very significant.
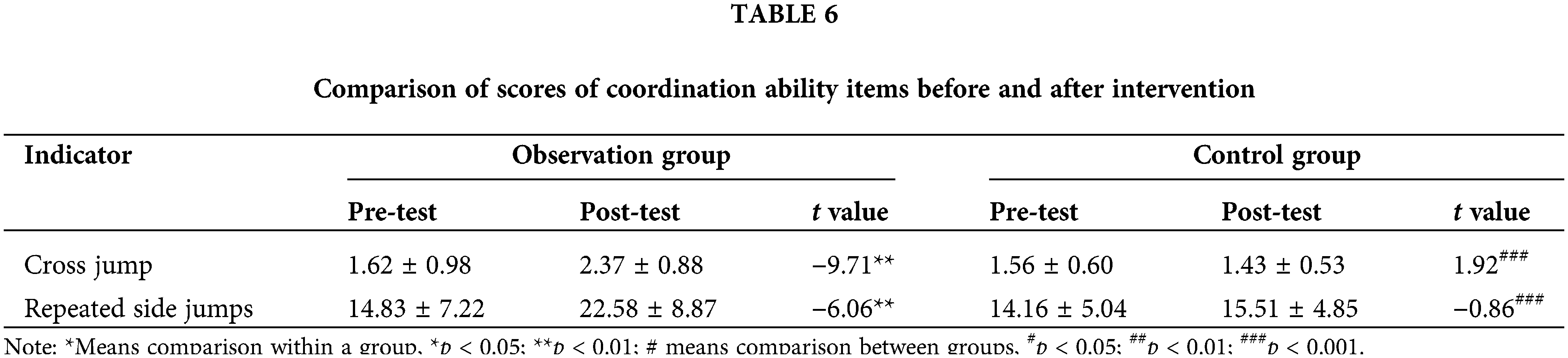
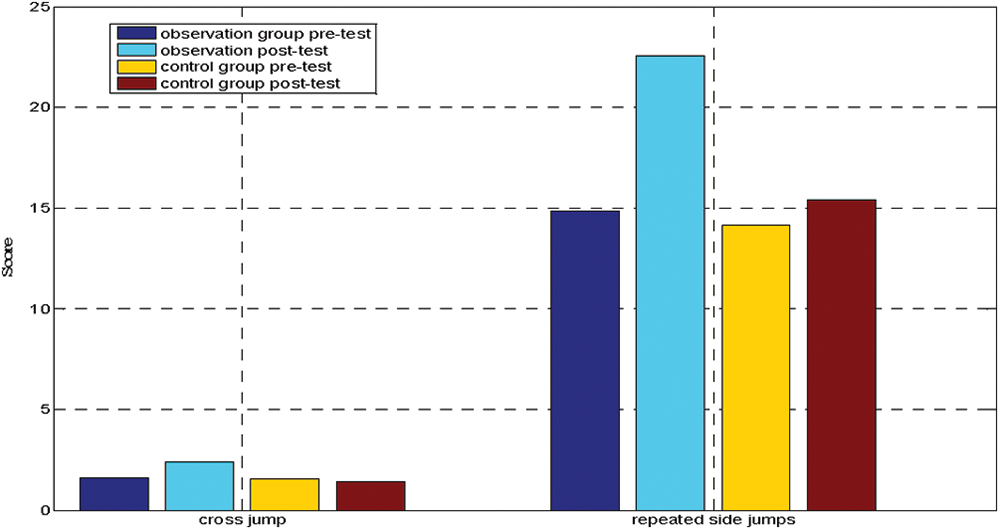
Figure 6: Coordinating the changes of each item before and after the two groups of experiments.
In early childhood development, movement coordination is closely related to nervous system development, and its development is crucial to the learning and development of body shape and physical fitness. Therefore, movement coordination disorders not only affect the development of physical fitness, but also hinder the development of children’s nervous system, thus Restrict children’s social, intellectual, emotional and other aspects of development. This study adopts the method of dance therapy, and incorporates imitation exercises into the intervention, such as imitating animals such as kittens, piglets, and puppies, and life movements to increase coordination ability. The results show that dance therapy intervention has a positive effect on the coordination ability of children with autism, especially the exercises related to displacement movements and object manipulation movements in motor ability, such as side sliding, horse trotting, overhand throwing, kicking and so on. After dance therapy intervention, it has a positive effect on the coordination ability of children with autism.
Changes in the social ability of the tested children before and after the experiment
As shown in Fig. 7, before the intervention, there was no significant difference in the total score of SRS and the scores of each dimension (social perception, social cognition, social communication, social motivation, behavior style) between the dancing treatment group and the control group (p > 0.05). After 12 weeks of intervention, there were significant differences in the total SRS score and scores of each dimension (social perception, social cognition, social communication, social motivation, and behavioral style) between the dancing treatment group and the control group (p < 0.01). This shows that the dance therapy group has improved in all dimensions of social response, and has a promoting effect on the social interaction ability of children with autism. According to the SRS score, the higher the degree of social impairment is. Comparing the pre-test and post-test in the dance therapy group, the post-test scores of social perception, social cognition, social communication, social motivation and behavior were significantly reduced. This shows that there are significant differences in all dimensions in the dance treatment group before and after the intervention (p < 0.01), while there is no statistically significant difference in the scores of the social response scale before and after the control group (p > 0.05).
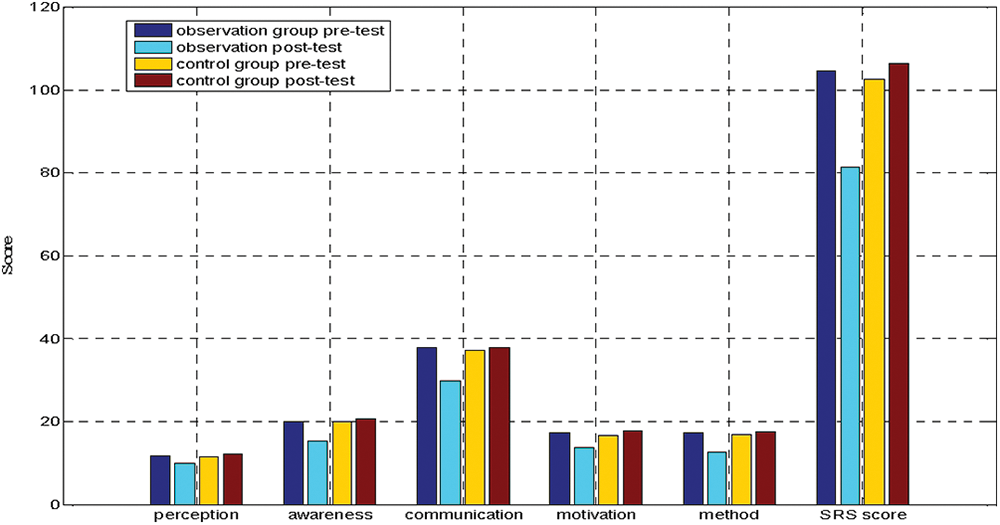
Figure 7: Changes of children’s SRS scores before and after the two groups of experiments.
People with autism have an advantage in dance and music, study finds. When selecting and designing intervention content, the strengths of the individual with autism can be used to develop areas of deficit. Therefore, DMT interventions use mirroring and group dynamics to provide a comfortable and acceptable environment for individuals with autism, thereby promoting physical fitness, motor development, and social skills in individuals with autism.
In this study, the dance therapy group established a kinesthetic empathy relationship with their peers during the intervention, increased physical and emotional experience, helped autistic children build trust with others, and promoted autistic children’s social communication skills. Therefore, in the DMT intervention environment, according to the advantages of individual movements of autistic children, an intervention plan based on body movement exercises was developed to make them full of emotional participation in physical communication activities, so as to achieve emotional regulation and provide social interaction with others. opportunities for interaction. Compared with single cognitive training, children with autism showed more enthusiasm and initiative in DMT intervention scenarios.
This study combs the theory of autistic children’s movement, social and communication abilities, combined with practical observation, expands the intervention mode of dance therapy in my country, and verifies the effect of dance therapy on the movement, social and communication abilities of children with autism through randomized controlled experiments. Improve the effect and provide a practical reference for dance intervention in the rehabilitation of children with autism. The main research conclusions of this paper are as follows: (1) 12 weeks of dance therapy intervention can improve the gross movement, balance and coordination ability of children with autism, and improve the movement ability of children with autism; (2) 12 weeks of dance therapy intervention can improve the Social perception, social cognition, social communication, social motivation, autistic behavior, improving the social dysfunction of children with autism. (3) The 12 weeks dance therapy intervention can promote the development of communication behaviors in children with autism. The frequency of eye gaze, body movements, and oral active communication has increased significantly, and communication skills have improved.
Acknowledgement: The authors thank research participants for their participation in this study.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: Study conception and design: Cuixiao Rui; data collection: Wang Shan; analysis and interpretation of results: Cuixiao Rui; draft manuscript preparation: Wang Shan. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data will be provided upon request to the corresponding author.
Ethics Approval: The study was approved by Ethics Committee at the Xinyang University (IRB number: 20221005-APP-S). All participants signed the informed consent in this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Pang YL, Lee CM, Wright M, Shen J, Shen B, Bo J. Challenges of case identification and diagnosis of autism spectrum disorders in China: a critical review of procedures, assessment, and diagnostic criteria. Res Autism Spect Dis. 2018;53:53–66. doi:10.1016/j.rasd.2018.06.003. [Google Scholar] [CrossRef]
2. Wingate M, Kirby RS, Pettygrove S, Cunniff C, Schulz E, Ghosh T, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years-autism and developmental disabilities monitoring network, 11 sites, United States, 2018. MMWR Surveill Summ. 2021;70(11):1–16. [Google Scholar]
3. Xu H, Wu Y. Lifestyle mobility in China: context, perspective and prospects. Mobilities. 2016;11(4):509–20. doi:10.1080/17450101.2016.1221027. [Google Scholar] [CrossRef]
4. Wang K, Wang X. Providing sports venues on mainland China: implications for promoting leisure-time physical activity and national fitness policies. Int J Env Res Pub He. 2020;17(14):1–11. doi:10.3390/ijerph17145136 [Google Scholar] [PubMed] [CrossRef]
5. Li XH, Song JC, Lin T, Dixon J, Zhang G, Ye H. Urbanization and health in China, thinking at the national, local and individual levels. Environ Health. 2016;15:113–23. doi:10.1186/s12940-016-0104-5. [Google Scholar] [CrossRef]
6. Petrus C, Adamson S, Block L, Einarson S, Sharifnejad M, Harris S. Effects of exercise interventions on stereotypic behaviours in children with autism spectrum disorder. Physioth Can. 2008;60(2):134–45. doi:10.3138/physio.60.2.134 [Google Scholar] [PubMed] [CrossRef]
7. Guo J, Li D. Effects of image-sandplay therapy on the mental health and subjective well-being of children with autism. Iran J Public Health. 2021;50(10):2046–54 [Google Scholar] [PubMed]
8. Dawson G, Bernier R. A quarter century of progress on the early detection and treatment of autism spectrum disorder. Dev Psychopathol. 2013;25(4):1455–72. doi:10.1017/S0954579413000710 [Google Scholar] [PubMed] [CrossRef]
9. Kikuchi Y, Senju A, Tojo Y, Osanai H, Hasegawa T. Faces do not capture special attention in children with autism spectrum disorder: a change blindness study. Child Dev. 2009;80(5):1421–33. doi:10.1111/j.1467-8624.2009.01342.x [Google Scholar] [PubMed] [CrossRef]
10. Deng Z, Wang H, Yu L. Supernormal abilities in individuals with autism: pitch perception advantage. J South China Normal Univ. 2011;1:95–9 (In Chinese). [Google Scholar]
11. Liu H, Yin Z, Wan X. Research progress and future prospect of dance movement therapy in China based on a Citespace visual analysis. Int J Phys Act Health. 2022;1(2):41–2. [Google Scholar]
12. Takahashi H, Matsushima K, Kato T. The effectiveness of dance/movement therapy interventions for autism spectrum disorder: a systematic review. Am J Dance Ther. 2019;41(1):55–74. doi:10.1007/s10465-019-09296-5. [Google Scholar] [CrossRef]
13. Landry H, Kingsbury M, Hamilton HA, Colman I. Psychological distress, non-medical use of prescription medications, and perceived unmet mental health care needs: a cross-sectional study of Ontario students. Soc Psychiatry Psychiatr Epidemiol 2023;58:1483–92 [Google Scholar] [PubMed]
14. Kanner L. Autistic disturbances of affective contact. Acta Paediatr. 1968;35(4):100–36. [Google Scholar]
15. Fournier K, Hass C, Naik S, Lodha N, Cauraugh J. Motor coordination in autism spectrum disorders: a synthesis and meta-analysis. J Autism Dev Disord. 2010;40:1227–40. doi:10.1007/s10803-010-0981-3 [Google Scholar] [PubMed] [CrossRef]
16. Dewey D, Cantell M, Crawford S. Motor and gestural performance in children with autism spectrum disorders, developmental coordination disorder, and/or attention deficit hyperactivity disorder. J Int Neuropsych Soc. 2007;13(2):246–56. doi:10.1017/S1355617707070270 [Google Scholar] [PubMed] [CrossRef]
17. Green D, Charman T, Pickles A, Chandler S, Simonoff E, Baird G. Impairment in movement skills of children with autistic spectrum disorders. Dev Med Child Neurol. 2009;51(4):311–6. doi:10.1111/j.1469-8749.2008.03242.x [Google Scholar] [PubMed] [CrossRef]
18. Klein M, Shinnar S, Rapin I. Abnormalities of joint mobility and gait in children with autism spectrum disorders. Brain Dev. 2014;36(2):91–6. doi:10.1016/j.braindev.2012.02.005 [Google Scholar] [PubMed] [CrossRef]
19. Lim Y, Partridge K, Girdler S, Morris S. Standing postural control in individuals with autism spectrum disorder: systematic review and meta-analysis. J Autism Dev Disord. 2017;47:2238–53. doi:10.1007/s10803-017-3144-y [Google Scholar] [PubMed] [CrossRef]
20. Travers B, Mason A, Gruben K, Dean D, McLaughlin K. Standing balance on unsteady surfaces in children on the autism spectrum: the effects of IQ. Res Autism Spect Dis. 2018;51:9–17. doi:10.1016/j.rasd.2018.03.008 [Google Scholar] [PubMed] [CrossRef]
21. Gong L, Liu Y, Yi L, Fang J, Yang Y, Wei K. Abnormal gait patterns in autism spectrum disorder and their correlations with social impairments. Autism Res. 2020;13(7):1215–26 [Google Scholar] [PubMed]
22. Martin S, Martin N, Vernazza A, Muller A, Rufo M, Massion J, et al. Goal directed locomotion and balance control in autistic children. J Autism Dev Disord. 2005;35:91–102. doi:10.1007/s10803-004-1037-3 [Google Scholar] [PubMed] [CrossRef]
23. Dyck M, Piek J, Hay D, Hallmayer J. The relationship between symptoms and abilities in autism. J Dev Phys Disabil. 2007;19:251–61. doi:10.1007/s10882-007-9055-7. [Google Scholar] [CrossRef]
24. Dyck M, Larson J, Apostu A, Mahone E, Denckla M, Mostofsky S. Dyspraxia in autism: association with motor, social, and communicative deficits. Dev Med Child Neurol. 2007;49(10):734–9. doi:10.1111/j.1469-8749.2007.00734.x [Google Scholar] [PubMed] [CrossRef]
25. Staples K, Reid G. Fundamental movement skills and autism spectrum disorders. J Autism Dev Disord. 2010;40:209–17. doi:10.1007/s10803-009-0854-9 [Google Scholar] [PubMed] [CrossRef]
26. Mayer R, Landa E. Development in infants with autism spectrum disorders: a prospective study. J Child Psychol Psyc. 2006;47(6):629–38. doi:10.1111/j.1469-7610.2006.01531.x [Google Scholar] [PubMed] [CrossRef]
27. Chevallier C, Kohls G, Troiani V, Brodkin E, Schultz R. The social motivation theory of autism. Trends Cogn Sci. 2012;16(4):231–9. doi:10.1016/j.tics.2012.02.007 [Google Scholar] [PubMed] [CrossRef]
28. Freeman S, Gulsrud A, Kasari C. Brief report: linking early joint attention and play abilities to later reports of friendships for children with ASD. J Autism Dev Disord. 2015;45:2259–66. doi:10.1007/s10803-015-2369-x [Google Scholar] [PubMed] [CrossRef]
29. Mundy P, Crowson M. Joint attention and early social communication: implications for research on intervention with autism. J Autism Dev Disord. 1997;27:653–76. doi:10.1023/A:1025802832021 [Google Scholar] [PubMed] [CrossRef]
30. Bird G, Press C, Richardson D. The role of alexithymia in reduced eye-fixation in autism spectrum conditions. J Autism Dev Disord. 2011;41:1556–64. doi:10.1007/s10803-011-1183-3 [Google Scholar] [PubMed] [CrossRef]
31. Povinelli D, Landau K, Perilloux H. Self-recognition in young children using delayed versus live feedback: evidence of a developmental asynchrony. Child Dev. 1996;67(4):1540–54. doi:10.2307/1131717. [Google Scholar] [CrossRef]
32. Andrews A. Emotions and social development: infants’ recognition of emotions in others. Pediatrics. 1998;102(5 Suppl E):109–18. [Google Scholar]
33. Mason W, Capitanio J. Basic emotions: a reconstruction. Emot Rev. 2012;4(3):238–44. doi:10.1177/1754073912439763 [Google Scholar] [PubMed] [CrossRef]
34. Widen S, Russell J. A closer look at preschoolers’ freely produced labels for facial expressions. Dev Psychol. 2003;39:114–28. doi:10.1037//0012-1649.39.1.114 [Google Scholar] [PubMed] [CrossRef]
35. Bryson S. Brief report: epidemiology of autism. J Autism Dev Disord. 1996;26(2):165–7. doi:10.1007/BF02172005 [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools