
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Instruments Assessing Problematic Use of the Internet and Their Associations with Psychological Distress among Ghanaian University Students
1 Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, 701, Taiwan
2 Department of Special Education and Counselling, The Education University of Hong Kong, Tai Po, New Territories, Hong Kong, China
3 Department of Behavioural Sciences, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, AK-4944, Ghana
4 International Gaming Research Unit, Psychology Department, Nottingham Trent University, Nottingham, NG1 4FQ, UK
5 Department of Nursing, School of Health and Welfare, Jönköping University, Jönköping, SE-551 11, Sweden
6 Biostatistics Consulting Center, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, 701, Taiwan
7 Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, 701, Taiwan
8 Department of Occupational Therapy, College of Medicine, National Cheng Kung University, Tainan, 701, Taiwan
* Corresponding Authors: Emma Sethina Adjaottor. Email: ; Chung-Ying Lin. Email:
# Yu-Ting Huang and Daniel Kwasi Ahorsu contributed equally to this work
International Journal of Mental Health Promotion 2024, 26(11), 875-885. https://doi.org/10.32604/ijmhp.2024.057049
Received 06 August 2024; Accepted 30 September 2024; Issue published 28 November 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: The present study evaluated the psychometric properties of Problematic Internet Use (PIU) instruments and their correlation with psychological distress and time spent on Internet activities among university students in Ghana. Methods: In the present cross-sectional survey design study, 520 participants (35.96% female) were recruited with a mean age of 19.55 years (SD = 1.94) from several university departments (i.e., Behavioral Sciences, Materials Engineering, Nursing and Midwifery, and Biochemistry and Biotechnology) of Kwame Nkrumah University of Science and Technology (KNUST) between 19 July and 04 August, 2023. Participants completed a survey that included the following measures: the Gaming Disorder Test (GDT), Gaming Disorder Scale for Adolescents (GADIS-A), Internet Gaming Disorder Scale-Short Form (IGDS9-SF), Bergen Social Media Addiction Scale (BSMAS), Smartphone Application Based Addiction Scale (SABAS), Nomophobia Questionnaire (NMP-Q), and the external criterion measure: Depression Anxiety Stress Scale-21 (DASS-21). Confirmatory factor analysis (CFA) was carried out to evaluate the structure of the instruments. Cronbach’s α, McDonald’s ω, and composite reliability were used to evaluate internal consistency. Pearson correlation was used to examine the associations between the scores of instruments assessing PIU, time spent on Internet activities, and the level of psychological distress. Results: Model fits confirmed the (i) unidimensional structure of the GDT, BSMAS, SABAS, IGDS9-SF, (ii) two-factor structure of the GADIS-A, and (iii) four-factor structure of the NMP-Q. Additionally, the study found that different types of PIU were significantly associated with psychological distress and time spent on related Internet activities. Conclusion: The six instruments validated in the present study demonstrated very good to excellent psychometric properties when applied to university students in Ghana. The significant associations between Internet-related disorders, time spent on Internet-related activities, and psychological distress highlight the importance of addressing issues of PIU among this population.Keywords
The increase in Internet accessibility has transformed communication, education, work, and entertainment, including in Ghana (where the present study was carried out). Ghana is classified by the World Bank as a low- to middle-income country, and has experienced rapid technological advancement. Internet use has become progressively active in recent years after the Ghanaian government launched the Information and Communication Technology for Accelerated Development (ICT4AD) Policy in 2003. The ICT4AD led to the expansion of the information and communication technology (ICT) infrastructure and services, which enhanced Internet accessibility [1]. In addition, the use of ICTs in education and social connection has significantly increased in Ghana due to the closure of schools caused by COVID-19 [2]. Compared to the period before the COVID-19 pandemic in 2018, the number of Internet users has significantly increased by approximately 137.97%, rising from 12.64 million to 30.08 million at the start of 2024 [3]. Meanwhile, the number of social media users increased by approximately 23% from 6 million to 7.4 million [4]. However, the widespread prevalence of Internet use has provided some challenges. In some cases, the increased accessibility and reliance on the Internet have resulted in problematic Internet use (PIU), such as the problematic playing of videogames [5].
The definition of PIU indicates overuse, impaired control, and having the urge to use the Internet. In its most extreme form, it is also considered an addictive behavior. PIU presents in various forms. Internet gaming disorder (IGD) proposed in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and gaming disorder (GD) included in the eleventh revision of the International Classification of Diseases (ICD-11) is one such form, characterized by impaired control over gaming behaviors, leading to functional impairment that impacts personal lives [6,7]. Problematic social media use is another form of PIU, characterized by individuals having an urge and being overly engaged with social media platforms such as Facebook, Instagram, and Twitter (now X). This often leads to reduced real-life social interactions and reduced productivity, which negatively impacts education and/or occupation [8]. Smartphones provide high accessibility to the Internet, which makes problematic smartphone use an issue when it becomes challenging to withdraw from using the smartphone, fostering continuous and excessive online engagement that leads to significant impairment in various aspects of daily life [9]. The attachment to smartphones has also led to the emergence of nomophobia (the fear of being without a mobile phone) which triggers anxiety and discomfort when individuals are unable to access their smartphone [10]. These PIU behaviors share similar features and use patterns (e.g., frequency/duration of use) but are distinct (e.g., gaming, social networking, and media streaming). The negative consequences (NCs) underscore the need for targeting distinctive Internet use behaviors when assessing PIU.
PIU has emerged as a significant public health concern, including psychological distress [11,12]. Psychological distress includes symptoms such as depression, anxiety, and stress. Numerous studies, including those conducted among Ghanaians, have established a strong association between PIU and psychological distress. People with high levels of PIU often report higher levels of depression and anxiety [5,12–14]. This makes the issue of PIU important because the Ghanaian government may not have sufficient resources to deal with the health problems (especially mental health problems) caused by PIU.
The Gaming Disorder Test (GDT), Gaming Disorder Scale for Adolescents Test (GADIS-A), and Internet Gaming Disorder Scale-Short Form (IGDS9-SF) are instruments for evaluating specific PIU related to gaming behaviors. The Bergen Social Media Addiction Scale (BSMAS) is an instrument for assessing another specific PIU (i.e., problematic social media use). The Smartphone Application Based Addiction Scale (SABAS) is an instrument that evaluates generalized PIU associated with diverse Internet activities conducted on smartphones. The Nomophobia Questionnaire (NMP-Q) is an instrument for assessing the fear of being without a mobile phone. All these instruments have been validated with good psychometric properties in Western [15–19] and Asian [20–23] countries. However, to the best of the authors’ best knowledge, no previous research has thoroughly examined the psychometric properties of these instruments in Ghana. More specifically, existing studies often rely on instruments developed and validated in contexts other than African countries, which may not fully capture the unique living conditions and Internet use patterns among low- and middle-income countries. Moreover, there is a lack of validated instruments based on the state-of-art diagnostic criteria documented in the DMS-5 or ICD-11, and for examining specific forms of PIU among Ghanaians [24].
Despite the growing recognition of PIU as a significant health concern, there remains a noticeable research gap in the Ghanaian context. Most existing studies rely on instruments developed and validated outside of Africa. Additionally, there is a lack of validated instruments based on the latest diagnostic criteria for assessing specific sub-types of PIU (e.g., GD, social media addiction, and smartphone addiction) among Ghanaians. Therefore, the present study evaluated the psychometric properties of these various PIU instruments and examined their correlation with psychological distress and time spent on related Internet activities among university students in Ghana. The primary hypotheses were that the instruments would demonstrate good psychometric properties, and be consistent with results from previous studies. Additionally, it is hypothesized that the scores of PIU-related instruments would be associated with psychological distress and related Internet activities. It was expected that the study’s findings would confirm the reliability and validity of widely used PIU-related instruments that enable researchers and clinicians in Ghana to accurately assess and identify PIU behaviors and provide insights into the mental health implications of PIU.
A cross-sectional survey design was used for the present study.
The participants were mainly recruited from several departments (i.e., Behavioral Sciences, Materials Engineering, Nursing and Midwifery, and Biochemistry and Biotechnology) of Kwame Nkrumah University of Science and Technology (KNUST) between 19 July and 04 August, 2023. The inclusion criteria were (i) being aged between 18 and 24 years, (ii) being a Ghanaian student at university, (iii) possessing a smartphone or having used one before, and (iv) having experience in using the Internet. The study obtained ethical approval from Kwame Nkrumah University of Science and Technology (CHRPE/AP/612/23). The research team sought permission from various lecturers to recruit their students for the study. The potential participants were then informed of the study details and provided with a ‘paper-and-pencil’ survey if they wanted to participate. They were first given the consent form to sign and then the surveys were distributed to all the participants who consented with the help of three research assistants. They were also informed of their rights including confidentiality, anonymity, and the right to withdraw anytime without repercussion. Ample time was given to the participants to respond to the questionnaire. All the survey questions were in the English language and included questions about participants’ demographic characteristics (i.e., age and gender) and assessment on Internet use, smartphone applications, gaming, social media, smartphone use, and psychological distress. Measures on these variables were carefully selected based on their cross-cultural psychometric indices and potential fit in the Ghanaian culture. Therefore, the participants were directed to read the instructions for each measure before responding to it. Also, they were given enough time and free space (for confidentiality) to ensure that they responded truthfully without biases. They could also seek clarity if they did not understand any of the items. All the surveys were collected on the same day by the research team. After all the surveys were collected, participants were given the opportunity to ask questions about the study and then thanked for their help.
The Gaming Disorder Test (GDT)
The GDT is a self-report instrument designed to assess GD symptoms over a 12-month period based on the diagnostic criteria as defined in the ICD-11 [15]. It consists of four items, including the ability to control gaming behavior, priority given to gaming, continuation of gaming, and experience of significant problem. All four items are scored using a 5-point Likert scale (1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = very often), with a higher score indicating more severe symptoms. A previous study reported very good internal consistency for the GDT (α = 0.84) [15].
Gaming Disorder Scale for Adolescents (GADIS-A)
The GADIS-A is a self-report instrument designed to assess the risk of GD among adolescents [20]. It comprises the cognitive behavior symptoms (CBS) subscale (Items 1, 2, 4, and 5), the negative consequences (NC) subscale (Items 3, 6, 8, and 9), and four additional questions regarding the frequency of experiencing problems due to gaming (Items 10–13), reflecting the ICD-11 criteria for GD. The first nine of the 13 items are scored on a 5-point Likert scale (1 = strongly disagree; 2 = somewhat disagree; 3 = partially agree/partially disagree; 4 = somewhat agree; 5 = strongly agree) with a higher score indicating a greater likelihood of experiencing GD. A previous study reported excellent internal consistency for the GADIS-A (α = 0.91) [20].
Bergen Social Media Addiction Scale (BSMAS)
The BSMAS is a self-report six-item instrument designed to assess the risk of social media addiction based on the experience of social media use over a 12-month period [16,17]. All six items are scored using a 5-point Likert scale (1 = very rarely; 2 = rarely; 3 = sometimes; 4 = often; 5 = very often), with a higher score indicating a greater risk of experiencing social media addiction. Previous studies have reported very good internal consistency for the BSMAS (α = 0.91) [21–23].
Smartphone Application Based Addiction Scale (SABAS)
The SABAS is a self-report six-item instrument designed to assess the risk of developing addictions to smartphone applications [17,18]. All six items are scored using a 6-point Likert scale (1 = strongly disagree; 2 = disagree; 3 = slightly disagree; 4 = slightly agree; 5 = agree; 6 = strongly agree), with a higher score indicating a greater risk of experiencing addiction to smartphone applications. A previous study reported very good internal consistency for the SABAS (α= 0.81) [25].
Internet Gaming Disorder Scale-Short Form (IGDS9-SF)
The IGDS9-SF is a self-report instrument designed to assess IGD over a 12-month period based on the diagnostic criteria as defined in the DSM-5 [26]. All nine items are scored using a 5-point Likert scale (1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = very often), with a higher score indicating greater IGD severity. A previous review of many studies using the IGDS9-SF reported very good psychometric properties [27].
Nomophobia Questionnaire (NMP-Q)
The NMP-Q is a self-report instrument designed to assess the fear of being without a mobile phone [19]. It consists of four factors: not being able to communicate (Items 1–4), losing connectedness (Items 5–9), not being able to access information (Items 10–15), and giving up convenience (Items 16–20). All 20 items are scored using a 7-point Likert scale (from 1 = strongly disagree to 7 = strongly agree), with a higher score indicating a greater nomophobia. The original validation study reported excellent internal consistency for the NMP-Q (α = 0.95) [19].
Depression Anxiety Stress Scale-21 (DASS-21)
The DASS-21 is a self-report instrument designed to assess the level of psychological distress over the past week. It consists of three subscales: depression, anxiety, and stress [28]. All 21 items are scored using a 4-point Likert scale (from 0 = not applied to me at all to 3 = applied to me very much or most of the time), with a higher score indicating a greater psychological distress. Previous studies reported have reported good internal consistency for the DASS-21 [17,29,30].
Data cleaning was conducted, and descriptive statistics such as means, standard deviations, skewness, and kurtosis were used to ensure that the data distribution was appropriate for further analyses. Descriptive analyses were used to summarize the characteristics of the participants and the item properties of the instruments. Apart from the descriptive statistics, item properties of all instruments were examined through factor loadings and item-total correlation. Cronbach’s α, McDonald’s ω, and composite reliability were used to evaluate internal consistency, with a threshold of >0.70 indicating acceptable internal consistency.
Confirmatory factor analysis (CFA) was carried out to evaluate the structure of the instruments. More specifically, (i) the unidimensional structure of the GDT, BSMAS, SABAS, IGDS9-SF, (ii) two-factor structure of the GADIS-A, and (iii) four-factor structure of the NMP-Q. All CFAs were conducted using the diagonally weighted least square (DWLS) estimator. Various fit indices were used to indicate the goodness of model fits, including a nonsignificant χ2 test, comparative fit index (CFI) and Tucker-Lewis’s index (TLI) >0.9, standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA) <0.08, all of which supported the factor structure [31,32].
Pearson correlations were used to test the associations between the scores of Internet-related instruments (i.e., GDT, GADIS-A, BSMAS, SABAS, IGDS9-SF, and NMP-Q), time spent on Internet activities (i.e., online gaming, social media use, and online learning), and the level of psychological distress (i.e., the score of depression, anxiety, and stress subscales in the DASS-21). The level of statistical significance was set at p < 0.05. The strength of the correlations was interpreted using standard benchmarks: r = 0.10 to 0.29 for small, r = 0.30 to 0.49 for medium, and r ≥ 0.50 for large effects. CFA and Pearson correlation were conducted using JASP 0.18.3. IBM SPSS Statistics 22.0 was used for all other statistical analyses.
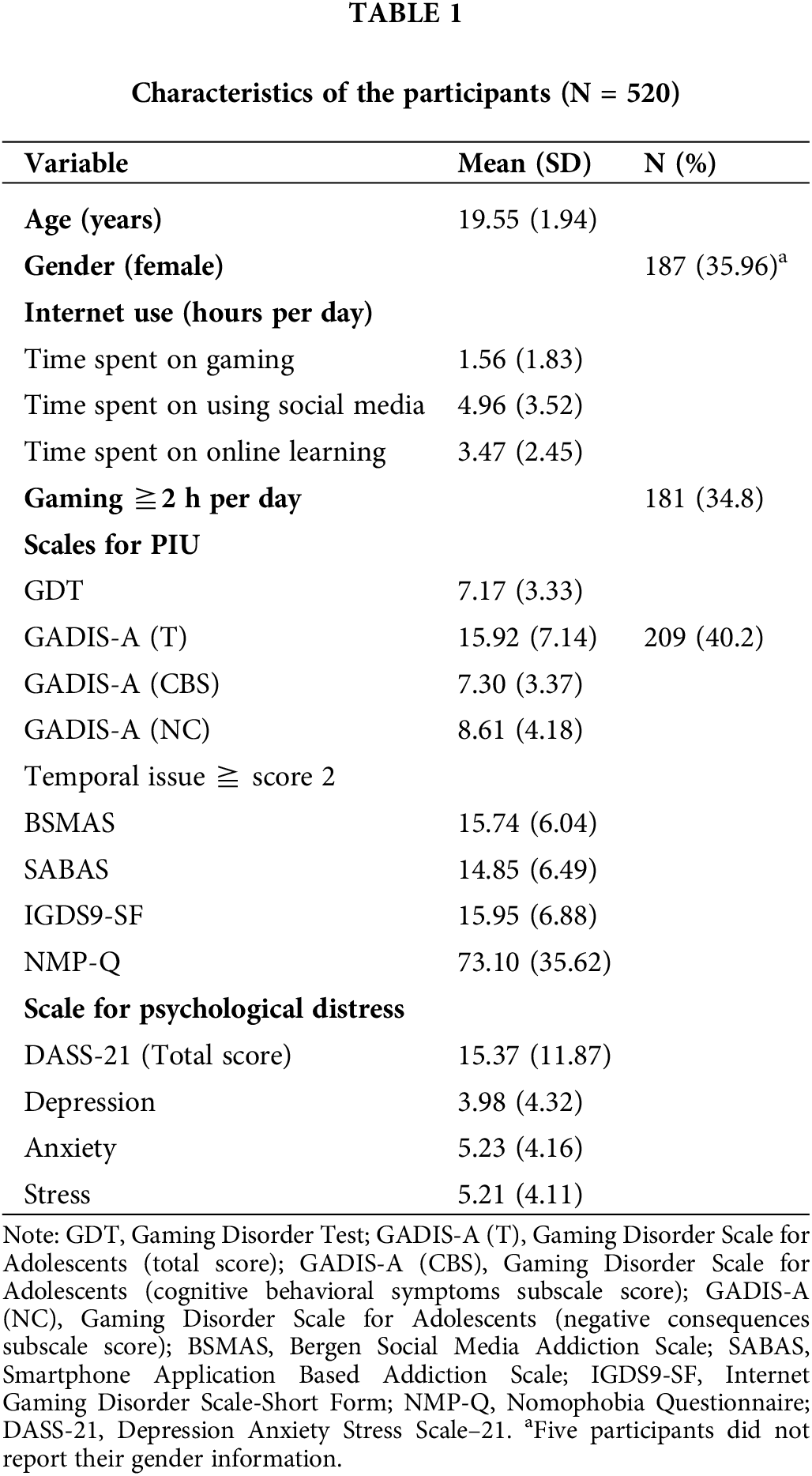
In the present study, there were 520 participants (35.96% female) with a mean age of 19.55 years (SD = 1.94). Participants reported an average of 1.56 h spent on gaming daily (SD = 1.83), 4.96 h on social media daily (SD = 3.52), and 3.47 h on online learning daily (SD = 2.45). The scores on the PIU scales were as follows: GDT (mean score = 7.17 out of 20; SD = 3.33), GADIS-A (mean score = 15.92 out of 36; SD = 7.14), BSMAS (mean score = 15.74 out of 30; SD = 6.04), SABAS (mean score = 14.85 out of 36; SD = 6.49), IGDS9-SF (mean score = 15.95 out of 45; SD = 6.88), and NMP-Q (mean score = 73.10 out of 140; SD = 35.62), and DASS-21 (mean score = 15.37 out of 63; SD = 11.87) (Table 1).
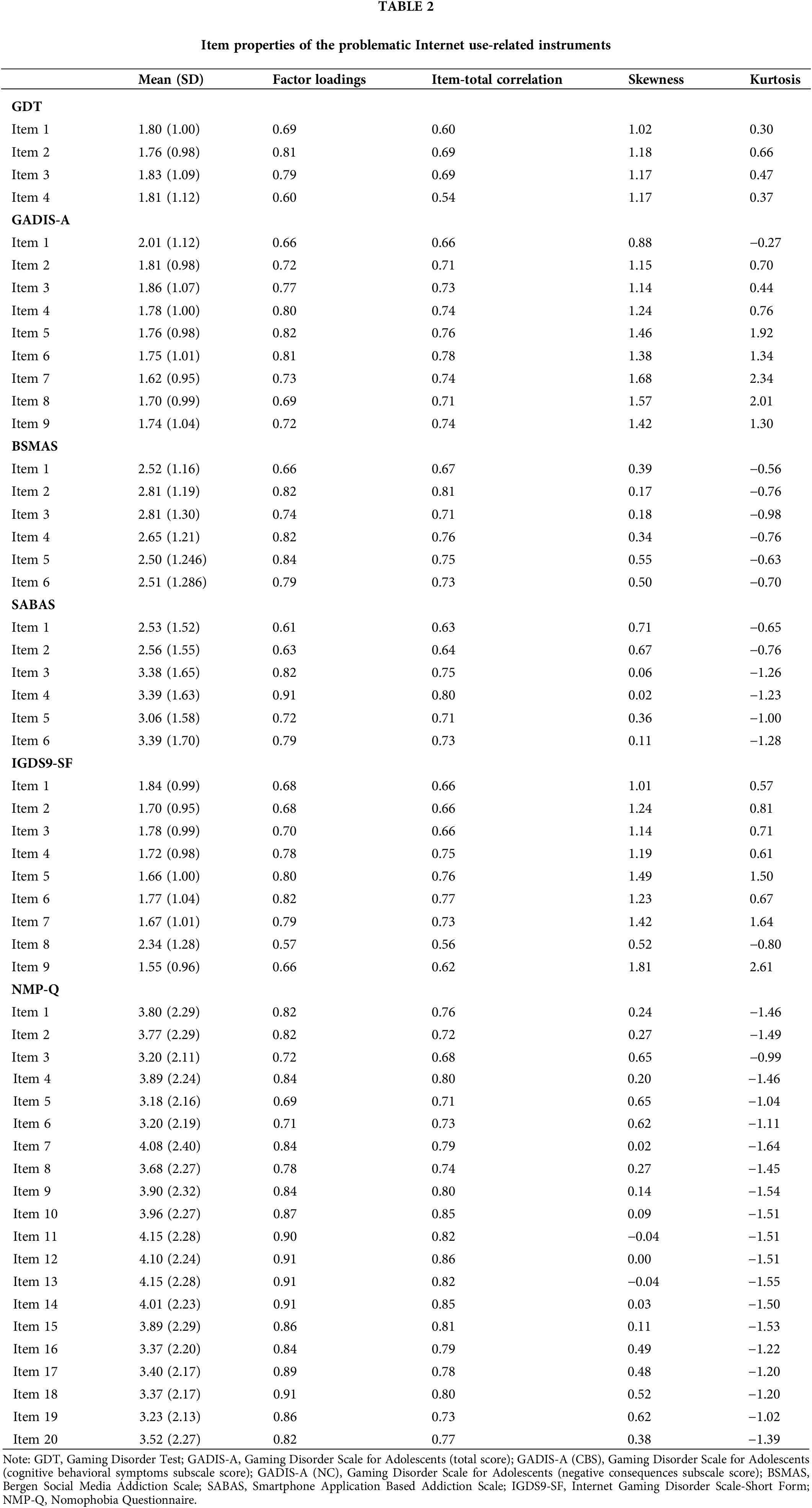
The descriptive statistics demonstrated near-normal distributions with acceptable values of skewness (ranging from: 0.60 to 0.69 for GDT, 0.66 to 0.8 for GADIS-A, 0.67 to 0.76 for BSMAS, 0.63 to 0.80 for SABAS, 0.52 to 1.81 for IGDS9-SF, −0.04 to 0.65 for NMP-Q) and kurtosis (ranging from: 0.30 to 0.66 for GDT, −0.27 to 2.34 for GADIS-A, −0.56 to −0.63 for BSMAS, −0.65 to −1.28 for SABAS, −0.80 to 2.61 for IGDS9-SF, −0.99 to −1.55 for NMP-Q). All values of factor loadings and item-total correlation were above 0.4 (Table 2).
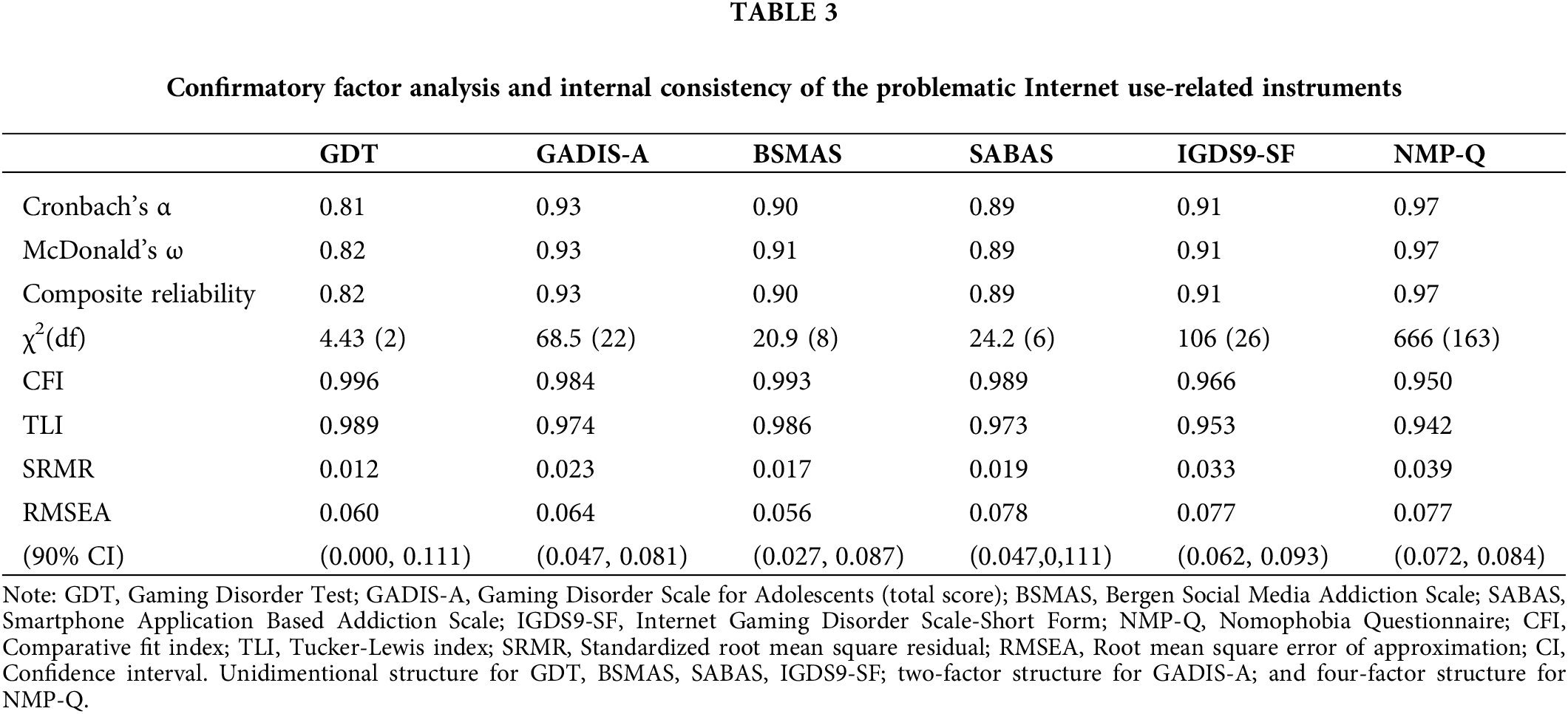
The internal consistency values ranged from 0.81 to 0.97 indicating very good to excellent reliability for all instruments. More specifically, Cronbach’s α = 0.81, McDonald’s ω = 0.81, and composite reliability = 0.81 for GDT; Cronbach’s α = 0.93, McDonald’s ω = 0.93, and composite reliability = 0.93 for GADIS-A; Cronbach’s α = 0.91, McDonald’s ω = 0.91, and composite reliability = 0.90 for BSMAS; Cronbach’s α = 0.89, McDonald’s ω = 0.89, and composite reliability = 0.89 for IGDSF-S9; and Cronbach’s α = 0.97, McDonald’s ω = 0.97, and composite reliability = 0.97 for NMP-Q. In the CFA fit indices supported the unidimensional structure of the GDT (CFI = 1.000, TLI = 0.999, SRMR = 0.016, RMSEA = 0.026), BSMAS (CFI = 1.000, TLI = 0.999, SRMR = 0.019, RMSEA = 0.030), SABAS (CFI = 0.998, TLI = 0.997, SRMR = 0.029, RMSEA = 0.068), and IGDS9-SF (CFI = 0.999, TLI = 0.998, SRMR = 0.035, RMSEA = 0.044). The CFA fit indices also supported the two-factor structure for GADIS-A (CFI = 0.998, TLI = 0.997, SRMR = 0.037, RMSEA = 0.067) and the four-factor structure for NMPQ (CFI = 0.998, TLI = 0.998, SRMR = 0.038, RMSEA = 0.069) (Table 3).
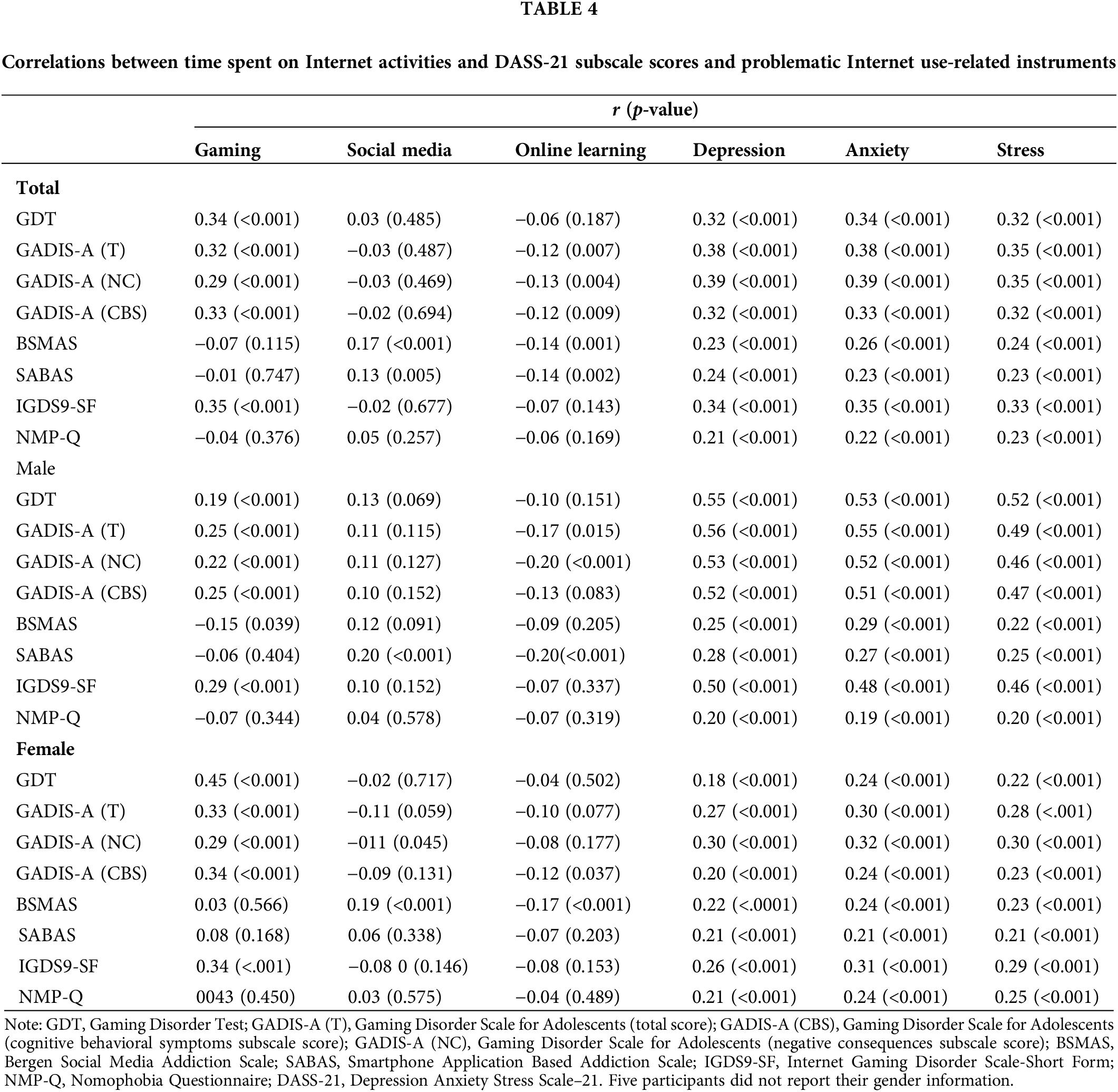
The scores on the problematic gaming-related instruments (i.e., GDT, GADIS-A, IGDS9-SF) showed a significant positive correlation with GD (r = 0.29–0.35; all p-values < 0.001). Time spent on social media was found to be positively related to the score on the social media addiction scale (BSMAS; r = 0.17; p < 0.001) and smartphone addiction scale (SABAS; r = 0.13; p < 0.001). Higher scores on the DASS-21 were associated with higher scores on the problematic Internet use-related instruments (r = 0.21–0.39; all p-values < 0.001), especially with gaming disorder (r = 0.32–0.35; all p-values < 0.001), indicating an association between problematic Internet use and psychological distress. With regards to the results of the correlations across gender, the scores of the problematic gaming-related instruments showed a significant positive correlation with gaming time among both males (r = 0.19–0.29; all p-values < 0.001) and females (r = 0.29–0.45; all p-values < 0.001). An additional negative correlation between score on the BSMAS and gaming time was found among males (r = −0.15; p < 0.005). Time spent on social media was found to be (i) positively related to score on the SABAS among males, and (ii) negative related to the GADIS-A NC subscale score (r = −0.11; p < 0.005) and positive related to BSMAS score (r = 0.19; p < 0.001) among females. Higher scores on the DASS-21 were associated with higher scores on the problematic Internet use-related instruments among both males (r = 0.19–0.56; all p-values < 0.001) and females (r = 0.18–0.32; all p-values < 0.001), with a more pronounced relationship to gaming disorder among males (r = 0.46–0.56; all p-values < 0.001) (Table 4).
The present study validated five instruments in English (i.e., GDT, GADIS-A, IGDS9-SF, BSMAS, and SABAS) among university students from Ghana assessing PIU (including specific forms of PIU and generalized PIU); one instrument (i.e., NMP-Q) assessed the consequences of PIU, and their associations with general psychological distress (assessed using DASS-21) among university students in Ghana. All instruments demonstrated very good reliability. Model fits confirmed the (i) unidimensional structure of the GDT, BSMAS, SABAS, IGDS9-SF; (ii) two-factor structure of the GADIS-A; and (iii) four-factor structure of the NMP-Q. Additionally, the study found that all forms of PIU, irrespective of being specific or generalized, were significantly associated with psychological distress.
The GDT demonstrated a unidimensional structure with very good internal consistency (α = 0.81). This is in line with previous validations in other languages and populations [15,30,33,34], suggesting that the GDT is a reliable instrument for assessing GD among Ghanaian university students. The GDT was designed based on the diagnostic criteria outlined in the ICD-11. Although there are only four items in the GDT, all items capture distinctive features of GD. Higher GDT scores were significantly associated with higher levels of depression, anxiety, and stress, supporting the association between GD and psychological distress reported in previous studies [5,12]. GD may directly lead to psychological distress or through sleeping problems (as mediators) [35]. Additionally, individuals may reduce participation in social activities because of gaming which can contribute to feelings of loneliness and depression [36]. Individuals may adopt gaming as a method to escape from negative situations in the real world, especially those with emotional regulation deficits [37]. However, problematic gaming behaviors may trigger more emotional difficulties (for example, conflicts with families or friends), further creating a vicious circle of GD and psychological distress [36].
The GADIS-A CFA supported the two-factor structure and it had excellent internal consistency (α = 0.93). These results are consistent with previous findings in both Western and Asian adolescent populations [20,30,34,38]. These results suggest that the GADIS-A is a valid and reliable instrument for assessing GD among university students in Ghana. The GADIS-A was designed based on the ICD-11 diagnostic criteria defined. Paschke et al. developed the GADIS-A with a two-factor structure to describe GD symptoms and consequences of problematic gaming [20], which better distinguish individuals based on the level of symptoms and impairment experienced. Similar to the GDT, the GADIS-A had significant associations with time spent gaming and psychological distress. This indicates that the GADIS-A, like the GDT, is another robust instrument for assessing GD.
The IGDS9-SF exhibited a robust unidimensional structure and excellent internal consistency (α = 0.91). These psychometric properties align with those found in other international validations synthesized in a recent systematic review [27] suggesting that the IGDS9-SF is a reliable and valid instrument for assessing GD. The IGDS9-SF was developed based on the DSM-5 diagnostic criteria with a broader range of symptoms and a greater emphasis on biological symptoms compared to the ICD-11 diagnostic criteria for GD [27]. Despite the heterogeneity in the definitions of GD and IGD, both the DSM-5 and ICD-11 recognize problematic gaming as a condition characterized by impaired control over gaming, prioritizing gaming over other activities, and persisting in gaming despite negative consequences. Both frameworks require significant functional impairment and specific duration of symptoms for diagnosis, demonstrating a shared understanding of the problematic gaming. The positive associations between IGDS9-SF scores and levels of depression, anxiety, and stress confirmed the external criteria with GDT and GADIS-A in terms of reflecting mental health deficits.
The BSMAS was designed based on the addiction component model [39] with further evidence supporting both one-factor and two-factor structures [40,41]. The present study’s findings supported the unidimensional structure of BSMAS. This finding is consistent with prior studies validating the BSMAS in different cultural contexts [21–23]. The results indicated that the BSMAS is a robust instrument for assessing the potential development of social media addiction among university students in Ghana. The positive correlations between BSMAS scores and psychological distress indicators highlight the detrimental effects of social media addiction being associated with poor mental health as reported in previous studies [14,42]. Similar to problematic gaming, social media addiction has been found to be associated with sleeping problems which can intensify the development of psychological distress [35]. Excessively engaging in social media use can lead to social isolation, because individuals may reduce real-life social participation, and negative social comparison generated from social media platforms may contribute to poor self-esteem [36]. These social challenges can contribute to feelings of depression and anxiety. Moreover, individuals may see social media platforms as places to escape from the real world and seek validation [36]. Those who depend more on social media validation experience higher levels of psychological distress when their validation needs are unmet [43].
The SABAS was also developed using the components model of addiction [39]. Although the literature has debated the factor structure of the model when conducting validations with BSMAS, there is no research testing a two-factor structure of the SABAS. Previous studies have all provided validation of the single-factor structure. The present study’s results demonstrated good internal consistency (α = 0.89) and supported the unidimensional structure. These psychometric properties align with previous studies conducted in various countries [24,44,45]. The results suggest that the SABAS is a robust instrument for assessing the risk of smartphone addiction among Ghanaian university students. Associations were found between SABAS scores and levels of depression, anxiety, and stress. Smartphone addiction is associated with psychological distress due to its impacts on individuals’ behavior, emotions, and social interactions. Excessive use of smartphones often leads to sleeping problems and disruption of daily routines which can increase stress and anxiety [46]. Similar to social media addiction, smartphone addiction can contribute to social isolation because interactions on social media through smartphones can replace face-to-face relationships, leading to loneliness and depression [47].
The NMP-Q showed a four-factor structure with excellent internal consistency (α = 0.97). These results are consistent with prior research validating the NMP-Q in different cultural settings [10,19]. Higher NMP-Q scores were significantly associated with increased psychological distress, supporting the association between nomophobia and poor mental health. Nomophobia is associated with psychological distress due to the high dependence on mobile phones. The fear of not having a smartphone, often derived from the fear of missing out on updates on social media, can cause significant psychological distress [48]. Additionally, the fear of missing out can make it difficult to concentrate on daily tasks and can exacerbate psychological distress by causing disturbances in individuals’ personal lives [12].
The present study further investigated the correlations between time spent on Internet activities and DASS-21 subscale scores as well as PIU-related instruments. The overall results align with previous studies showing that PIU is positively correlated with psychological distress among both males and females [49–51]. Moreover, the results indicated a stronger relationship with GD, which was found to be more pronounced among males, suggesting a stronger link between gaming disorder and psychological distress in males. These findings highlight that the psychological impact of PIU may differ between genders.
There are some limitations to the present study. First, the sample for the present study was predominantly composed of older adolescents from a single university in Ghana, which may limit the generalizability of the findings to other populations or age groups. Second, the study relied on self-report data, which is subject to social desirability and recall biases. Participants may have underreported or overreported their Internet use and psychological distress, potentially affecting the accuracy of the findings. Third, the study did not assess the test-retest reliability of the instruments, which is essential for determining the stability of the instruments over time. To address these aforementioned limitations, future research should include more diverse and representative samples to enhance the external validity of the results. Incorporating objective measures of Internet use could help reduce the bias od using self-report data. Future research should include longitudinal designs to evaluate the consistency of these instruments across different time points.
In conclusion, the six instruments validated among university students from Ghana in the present study demonstrated very good to excellent psychometric properties when applied to university students in Ghana. The significant associations between Internet-related disorders, time spent on Internet-related activities, and psychological distress highlight the importance of addressing issues of PIU among this population. Despite the limitations, the present study provides a valuable contribution to the understanding of Internet-related disorders in a Ghanaian context and underscores the need for continuous research and intervention efforts in this area.
Acknowledgement: We thank all the participants.
Funding Statement: This research was supported in part by Higher Education Sprout Project, Ministry of Education to the Headquarters of University Advancement at National Cheng Kung University (NCKU). This research was supported in part by (received funding from) the National Science and Technology Council, Taiwan (NSTC 112-2410-H-006-089-SS2).
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: Daniel Kwasi Ahorsu, Emma Sethina Adjaottor, Chung-Ying Lin; data collection: Daniel Kwasi Ahorsu, Emma Sethina Adjaottor, Frimpong-Manso Addo; analysis and interpretation of results: Yu-Ting Huang, Daniel Kwasi Ahorsu, Mark D. Griffiths, Amir H. Pakpour, Chung-Ying Lin; draft manuscript preparation: Yu-Ting Huang, Daniel Kwasi Ahorsu, Chung-Ying Lin; critically review and edit manuscript: Emma Sethina Adjaottor, Frimpong-Manso Addo, Mark D. Griffiths, Amir H. Pakpour, Chung-Ying Lin. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available on reasonable request from the corresponding author.
Ethics Approval: The study obtained ethical approval from Kwame Nkrumah University of Science and Technology (CHRPE/AP/612/23). Written informed consent was provided by all participants.
Conflicts of Interest: All the authors declare no conflicts of interest except MDG. MDG has received research funding from Norsk Tipping (the gambling operator owned by the Norwegian government). MDG has received funding for a number of research projects in the area of gambling education for young people, social responsibility in gambling and gambling treatment from Gamble Aware (formerly the Responsibility in Gambling Trust), a charitable body which funds its research program based on donations from the gambling industry. MDG undertakes consultancy for various gambling companies in the area of player protection and social responsibility in gambling.
References
1. Kubuga KK, Ayoung DA, Bekoe S. Ghana’s ICT4AD policy: between policy and reality. Digit Pol Regul Gov. 2021;23(2):132–53. [Google Scholar]
2. Sarpong SA, Dwomoh G, Boakye EK, Ofosua-Adjei I. Online teaching and learning under COVID-19 pandemic; perception of university students in Ghana. Eur J Interact Multimed Educ. 2021;3(1):e02203. doi:10.30935/ejimed/11438. [Google Scholar] [CrossRef]
3. Degenhard J. Ghana: internet users 2014-2029. Statista; 2024. Available from: https://www.statista.com/forecasts/1145600/internet-users-in-ghana. [Accessed 2024]. [Google Scholar]
4. Sasu DD. Ghana: active social media users 2024. Statista; 2024. Available from: https://www.statista.com/statistics/1171445/number-of-social-media-users-ghana. [Accessed 2024]. [Google Scholar]
5. Miezah D, Batchelora J, Megreya A, Richard Y, Moustafa A. Video/computer game addiction among university students in Ghana: prevalence, correlates and effects of some demographic factors. Psyc Clin Psychopharmacol. 2020;1. [Google Scholar]
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. USA: American Psychiatric Publishing; 2013. doi:10.1176/appi.books.9780890425596. [Google Scholar] [CrossRef]
7. World Health Organization. International classification of diseases, 11th revision (ICD-11). World Health Organization; 2019. Available from: https://icd.who.int [Accessed 2024]. [Google Scholar]
8. Sun Y, Zhang Y. A review of theories and models applied in studies of social media addiction and implications for future research. Addict Behav. 2021;114:106699. doi:10.1016/j.addbeh.2020.106699. [Google Scholar] [PubMed] [CrossRef]
9. Lin YH, Chiang CL, Lin PH, Chang LR, Ko CH, Lee YH, et al. Proposed diagnostic criteria for smartphone addiction. PLoS One. 2016;11(11):e0163010. doi:10.1371/journal.pone.0163010. [Google Scholar] [PubMed] [CrossRef]
10. Lin CY, Griffiths MD, Pakpour AH. Psychometric evaluation of Persian Nomophobia Questionnaire: differential item functioning and measurement invariance across gender. J Behav Addict. 2018;7(1):100–8. doi:10.1556/2006.7.2018.11. [Google Scholar] [PubMed] [CrossRef]
11. Durkee T, Carli V, Floderus B, Wasserman C, Sarchiapone M, Apter A, et al. Pathological internet use and risk-behaviors among European adolescents. Int J Environ Res Public Health. 2016;13(3):294. doi:10.3390/ijerph13030294. [Google Scholar] [PubMed] [CrossRef]
12. Ruckwongpatr K, Chirawat P, Ghavifekr S, Gan WY, Tung SEH, Nurmala I, et al. Problematic internet use (PIU) in youth: a brief literature review of selected topics. Curr Opin Behav Sci. 2022;46:101150. doi:10.1016/j.cobeha.2022.101150. [Google Scholar] [CrossRef]
13. Javed S, Kakul F. Internet gaming disorder: an interplay of cognitive psychopathology. Asian J Soc Health Behav. 2023;6(1):36. doi:10.4103/shb.shb_209_22. [Google Scholar] [CrossRef]
14. Alimoradi Z, Lin CY, Broström A, Bülow PH, Bajalan Z, Griffiths MD, et al. Internet addiction and sleep problems: a systematic review and meta-analysis. Sleep Med Rev. 2019;47(3):51–61. doi:10.1016/j.smrv.2019.06.004. [Google Scholar] [PubMed] [CrossRef]
15. Pontes HM, Schivinski B, Sindermann C, Li M, Becker B, Zhou M, et al. Measurement and conceptualization of gaming disorder according to the world health organization framework: the development of the gaming disorder test. Int J Ment Health Addict. 2019;19(2):508–28. doi:10.1007/s11469-019-00088-z. [Google Scholar] [CrossRef]
16. Andreassen CS, Billieux J, Griffiths MD, Kuss DJ, Demetrovics Z, Mazzoni E, et al. The relationship between addictive use of social media and video games and symptoms of psychiatric disorders: a large-scale cross-sectional study. Psychol Addict Behav. 2016;30(2):252–62. doi:10.1037/adb0000160. [Google Scholar] [PubMed] [CrossRef]
17. Oppong D, Adjaottor ES, Addo F-M, Nyaledzigbor W, Ofori-Amanfo AS, Chen H-P, et al. The mediating role of selfitis in the associations between self-esteem, problematic social media use, problematic smartphone use, body-self appearance, and psychological distress among young Ghanaian adults. Healthcare. 2022;10(12):2500. doi:10.3390/healthcare10122500. [Google Scholar] [PubMed] [CrossRef]
18. Csibi S, Demetrovics Z, Szabo A. Hungarian adaptation and psychometric characteristics of Brief Addiction to Smartphone Scale (BASS). Psychiatr Hung. 2016;31(1):71–7. [Google Scholar]
19. Yildirim C, Correia AP. Exploring the dimensions of nomophobia: development and validation of a self-reported questionnaire. Comput Human Behav. 2015;49:130–7. doi:10.1016/j.chb.2015.02.059. [Google Scholar] [CrossRef]
20. Paschke K, Austermann MI, Thomasius R. Assessing ICD-11 gaming disorder in adolescent gamers: development and validation of the Gaming Disorder Scale for Adolescents (GADIS-A). J Clin Med. 2020;9(4):993. doi:10.3390/jcm9040993. [Google Scholar] [PubMed] [CrossRef]
21. Abiddine FZE, Aljaberi MA, Alduais A, Lin C-Y, Vally Z, Griffiths MD, et al. The psychometric properties of the Arabic Bergen Social Media Addiction Scale. Int J Ment Health Addict. 2024;24(4):215. doi:10.1007/s11469-024-01297-x. [Google Scholar] [CrossRef]
22. Pramukti I, Nurmala I, Nadhiroh SR, Tung SEH, Gan WY, Siaw YL, et al. Problematic use of internet among Indonesia university students: psychometric evaluation of Bergen Social Media Addiction Scale and Internet Gaming Disorder Scale-Short Form. Psychiatr Investig. 2023;20(12):1103–11. doi:10.30773/pi.2022.0304. [Google Scholar] [PubMed] [CrossRef]
23. Ruckwongpatr K, Paratthakonkun C, Sangtongdee U, Pramukti I, Nurmala I, Angkasith K, et al. Validity, reliability, and measurement invariance of the Thai Smartphone Application-Based Addiction Scale and Bergen Social Media Addiction Scale. Int J Ment Health Promot. 2024;26(4):293–302. doi:10.32604/ijmhp.2024.047023. [Google Scholar] [CrossRef]
24. Gjoneska B, Potenza MN, Jones J, Sales CM, Hranov G, Demetrovics Z. Problematic use of the Internet in low- and middle-income countries before and during the COVID-19 pandemic: a scoping review. Curr Opin Behav Sci. 2022;48:101208. doi:10.1016/j.cobeha.2022.101208. [Google Scholar] [PubMed] [CrossRef]
25. Csibi S, Griffiths MD, Cook B, Demetrovics Z, Szabo A. The psychometric properties of the Smartphone Application-Based Addiction Scale (SABAS). Int J Ment Health Addict. 2018;16(2):393–403. doi:10.1007/s11469-017-9787-2. [Google Scholar] [PubMed] [CrossRef]
26. Pontes HM, Griffiths MD. Measuring DSM-5 internet gaming disorder: development and validation of a short psychometric scale. Comput Human Behav. 2015;45:137–43. doi:10.1016/j.chb.2014.12.006. [Google Scholar] [CrossRef]
27. Poon LYJ, Tsang HWH, Chan TYJ, Man SWT, Ng LY, Wong YLE, et al. Psychometric properties of the Internet Gaming Disorder Scale-Short-Form (IGDS9-SFsystematic review. J Med Internet Res. 2021;23(10):e26821. doi:10.2196/26821. [Google Scholar] [PubMed] [CrossRef]
28. Lovibond SH, Lovibond PF. Manual for the depression anxiety & stress scales. Psychology Foundation of Australia; 1995. vol. 56, p. 42. [Google Scholar]
29. Cao CH, Liao XL, Jiang XY, Li XD, Chen IH, Lin CY. Psychometric evaluation of the Depression, Anxiety, and Stress Scale-21 (DASS-21) among Chinese primary and middle school teachers. BMC Psychol. 2023;11(1):209. doi:10.1186/s40359-023-01242-y. [Google Scholar] [PubMed] [CrossRef]
30. Chen IH, Chen CY, Liao XL, Chen XM, Zheng X, Tsai YC, et al. Psychometric properties of the Depression, Anxiety, and Stress Scale (DASS-21) among different Chinese populations: a cross-sectional and longitudinal analysis. Acta Psychol. 2023;240(2–3):104042. doi:10.1016/j.actpsy.2023.104042. [Google Scholar] [PubMed] [CrossRef]
31. Lin CY, Broström A, Griffiths MD, Pakpour AH. Psychometric evaluation of the Persian eHealth Literacy Scale (eHEALS) among elder Iranians with heart failure. Eval Health Prof. 2020;43(4):222–9. doi:10.1177/0163278719827997. [Google Scholar] [PubMed] [CrossRef]
32. Nadhiroh S, Nurmala I, Pramukti I, Tivany S, Tyas L, Zari A, et al. Weight stigma in Indonesian young adults: validating the Indonesian versions of the Weight Self-Stigma Questionnaire and Perceived Weight Stigma Scale. Asian J Soc Health Behav. 2022;5(4):169–79. doi:10.4103/shb.shb_189_22. [Google Scholar] [CrossRef]
33. Maldonado-Murciano L, Pontes HM, Barrios M, Gómez-Benito J, Guilera G. Psychometric validation of the Spanish Gaming Disorder Test (GDTitem response theory and measurement invariance analysis. Int J Ment Health Addict. 2021;21(3):1–19. [Google Scholar]
34. Wu T-Y, Huang S-W, Chen J-S, Kamolthip R, Kukreti S, Strong C, et al. Translation and validation of the Gaming Disorder Test and Gaming Disorder Scale for Adolescents into Chinese for Taiwanese young adults. Compr Psychiatr. 2023;124:152396. doi:10.1016/j.comppsych.2023.152396. [Google Scholar] [PubMed] [CrossRef]
35. Wang Q, Mati K, Cai Y. The link between problematic internet use, problematic gaming, and psychological distress: does sleep quality matter? BMC Psychiatr. 2021;21(1):103. doi:10.1186/s12888-021-03105-5. [Google Scholar] [PubMed] [CrossRef]
36. Wong HY, Mo HY, Potenza MN, Chan MNM, Lau WM, Chui TK, et al. Relationships between severity of internet gaming disorder, severity of problematic social media use, sleep quality and psychological distress. Int J Environ Res Public Health. 2020;17(6):1879. doi:10.3390/ijerph17061879. [Google Scholar] [PubMed] [CrossRef]
37. Gisbert-Pérez J, Badenes-Ribera L, Martí-Vilar M. Emotional intelligence and gaming disorder symptomatology: a systematic review and meta-analysis. Adolesc Res Rev. 2024. doi:10.1007/s40894-024-00233-30. [Google Scholar] [CrossRef]
38. Başdaş Ö, Özbey H, Bayat M. Psychometric properties of the Turkish version of the Gaming Disorder Scale for Adolescents (GADIS-A). J Pediatr Nurs. 2024;77(2):e218–24. doi:10.1016/j.pedn.2024.04.032. [Google Scholar] [PubMed] [CrossRef]
39. Griffiths M. A ‘components’ model of addiction within a biopsychosocial framework. J Subst Use. 2005;10(4):191–7. doi:10.1080/14659890500114359. [Google Scholar] [CrossRef]
40. Amendola S. Discussing evidence on the components model of addiction. A commentary on Fournier et al. (2023). Addict Behav. 2023;145(3):107764. doi:10.1016/j.addbeh.2023.107764. [Google Scholar] [PubMed] [CrossRef]
41. Fournier L, Schimmenti A, Musetti A, Boursier V, Flayelle M, Cataldo I, et al. Further evidence for the bidimensionality of the components model of addiction: a reply to Amendola (2023). Addict Behav. 2024;150(2):107914. doi:10.1016/j.addbeh.2023.107914. [Google Scholar] [PubMed] [CrossRef]
42. Huang PC, Latner JD, O’Brien KS, Chang YL, Hung CH, Chen JS, et al. Associations between social media addiction, psychological distress, and food addiction among Taiwanese university students. J Eat Disord. 2023;11(1):43. doi:10.1186/s40337-023-00769-0. [Google Scholar] [PubMed] [CrossRef]
43. Tullett-Prado D, Doley JR, Zarate D, Gomez R, Stavropoulos V. Conceptualising social media addiction: a longitudinal network analysis of social media addiction symptoms and their relationships with psychological distress in a community sample of adults. BMC Psychiatr. 2023;23(1):509. doi:10.1186/s12888-023-04985-5. [Google Scholar] [PubMed] [CrossRef]
44. Leung H, Pakpour AH, Strong C, Lin YC, Tsai MC, Griffiths MD, et al. Measurement invariance across young adults from Hong Kong and Taiwan among three internet-related addiction scales: bergen Social Media Addiction Scale (BSMASSmartphone Application-Based Addiction Scale (SABASand Internet Gaming Disorder Scale-Short Form (IGDS-SF9) (Study Part A). Addict Behav. 2020;101:105969. [Google Scholar] [PubMed]
45. Nurmala I, Nadhiroh SR, Pramukti I, Tyas LW, Zari AP, Griffiths MD, et al. Reliability and validity study of the Indonesian Smartphone Application-Based Addiction Scale (SABAS) among college students. Heliyon. 2022;8(8):e10403. doi:10.1016/j.heliyon.2022.e10403. [Google Scholar] [PubMed] [CrossRef]
46. Alzhrani AM, Aboalshamat KT, Badawoud AM, Abdouh IM, Badri HM, Quronfulah BS, et al. The association between smartphone use and sleep quality, psychological distress, and loneliness among health care students and workers in Saudi Arabia. PLoS One. 2023;18(1):e0280681. doi:10.1371/journal.pone.0280681. [Google Scholar] [PubMed] [CrossRef]
47. Volungis AM, Kalpidou M, Popores C, Joyce M. Smartphone addiction and its relationship with indices of social-emotional distress and personality. Int J Ment Health Addict. 2019;18(5):1209–25. [Google Scholar]
48. Santl L, Brajkovic L, Kopilaš V. Relationship between nomophobia, various emotional difficulties, and distress factors among students. Eur J Investig Health Psychol Educ. 2022;12(7):716–30. [Google Scholar] [PubMed]
49. Mh K, Kashmir HS. Evaluation of internet addiction, impulsivity and psychological distress among university students. Int J Clin Ther Diagn. 2015;1(3):70–6. [Google Scholar]
50. Anand N, Jain PA, Prabhu S, Thomas C, Bhat A, Prathyusha PV, et al. Internet use patterns, internet addiction, and psychological distress among engineering university students: a study from India. Indian J Psychol Med. 2018;40(5):458–67. doi:10.4103/IJPSYM.IJPSYM_135_18. [Google Scholar] [PubMed] [CrossRef]
51. Mooi CS, Ali H, Theng CA, Salim HS. Psychological distress and internet addiction among medical students from a malaysian public university: a comparison between gender. Malays J Med Health Sci. 2019;1(15):3–8. [Google Scholar]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools