
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

The Relationship between Psychological Vulnerability, Aging Attitudes and Life Meaning in Elderly Patients with Comorbidities
1 Department of Geriatrics, Renmin Hospital of Wuhan University, Wuhan, 430060, China
2 Department of General Practice, Renmin Hospital of Wuhan University, Wuhan, 430060, China
3 Department of Nursing, Renmin Hospital of Wuhan University, Wuhan, 430060, China
4 Department of Academic Research, Renmin Hospital of Wuhan University, Wuhan, 430060, China
5 Department of Nephrology, Renmin Hospital of Wuhan University, Wuhan, 430060, China
* Corresponding Author: Lili Zhang. Email:
# These authors contributed equally to this work
International Journal of Mental Health Promotion 2024, 26(11), 897-904. https://doi.org/10.32604/ijmhp.2024.056223
Received 17 July 2024; Accepted 25 September 2024; Issue published 28 November 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: With the rapid aging of China’s population and the increasing prevalence of comorbidities in the elderly, psychological crises have become more common. This study aims to investigate the present status of psychological vulnerability, aging attitudes, and life meaning in elderly patients with comorbidities. Methods: A total of 685 elderly inpatients and outpatients at Renmin Hospital of Wuhan University between July and December 2022 were selected using the simple random sampling method. Social demographic data were collected, and the Attitudes to aging Questionnaire (AAQ), the Chinese Life Meaning Questionnaire (C-MLQ), and the Psychological Vulnerability Scale (C-PVS) were used for the analysis. A total of 685 questionnaires were received, and 602 valid questionnaires were collected, with an effective rate of 87.88%. Data analysis was performed using SPSS V25.0 and AMOS V24.0. Results: The total scores of psychological vulnerability, aging attitudes, and life meaning were 69.4 ± 12.8, 80.2 ± 13.5 and 39.2 ± 8.3, respectively. The psychological vulnerability was significantly negatively correlated with life meaning and aging attitudes (r = −0.351, −0.264; p < 0.01). There was a significant positive correlation between aging attitudes and life meaning (r = 0.515; p < 0.01). Life meaning played a partial mediating role between psychological vulnerability and aging attitudes (β = 3.070, p < 0.05). Conclusion: This study found that the psychological vulnerability in elderly patients with comorbidities was at the lower level, which was related to the elderly patients’ aging attitudes and their current status of life meaning. The level of psychological vulnerability in elderly patients with senile-related comorbidities needs to be further improved. Medical workers should pay attention to the psychological vulnerability of elderly patients and improve the identification of psychological crises of such patients.Keywords
Nomenclature
| Term 1 | Interpretation 1 |
| Term 2 | Interpretation 2 |
| e.g., | |
| | Porosity |
| s | Skin factor |
Statistics from the Seventh National Census in China show that there are 264.02 million people over 60 years old, accounting for 18.7% of the total population (the Central Committee of the Communist Party of China, 2021). According to the outline of the ‘Healthy China 2030’ plan, the early detection of and timely intervention in psychological problems in key population groups should be strengthened, and the ability to identify and intervene in psychological crises in emergencies should be improved [1]. With the deepening of aging, the phenomenon of comorbidity in the elderly is becoming increasingly common. On the one hand, patients are more likely to experience psychological crises such as depression, worthlessness and loneliness. On the other hand, their ability to resist various crises has also declined [2]. According to statistics, 44.3–200 out of every 100,000 elderly people in China die by suicide, which is a relatively high level globally [3]. The potential cause of this problem is that the elderly with comorbidities have frequent mental health problems and high susceptibility to psychological crises [4–8].
The psychological vulnerability of elderly patients with comorbidities has become an urgent social problem. Such patients tend to develop relatively negative aging attitudes due to the long course of the disease, repeated illness, continuous drug treatment and other factors. Psychological crises in these patients can be described in terms of psychological vulnerability, which refers to the degree to which a person can withstand a crisis. Sinclair described individuals with cognitive patterns that make them more susceptible to stress, where psychological vulnerability is defined as a belief that reflects dependence on achievement or external sources of affirmation for the individual’s sense of self-worth [5].
Eriksson’s theory of psychosocial development suggests that there is a significant event in every stage of human life [9]. The important event in old age is reflection and the acceptance of life. The crisis to be dealt with at this stage is self-improvement and despair. In this process, the elderly can re-examine and reconcile their relationship with the past and reflect on the value and significance of life [10,11]. The meaning of life is an essential part of positive psychology [12], and studies have shown that a strong sense of life meaning can promote positive emotional experiences and enhance one’s ability to resist crises [13]. Similarly, aging attitudes act as a psychological tendency and a protective mechanism for mental health, helping to maintain physical and mental stability. Therefore, both aging attitudes and a sense of life meaning play critical roles in reducing negative emotions and improving the mental health of elderly patients with comorbidities.
Prior research suggests that positive aging attitudes can foster a greater sense of life meaning by helping individuals to reframe aging as a period of continued growth and contribution rather than decline [14]. This, in turn, can mitigate psychological vulnerability by enhancing psychological resilience and reducing the risk of adverse mental health outcomes. While it is plausible that life meaning could influence aging attitudes, the literature indicates that attitudes are more likely to serve as a precursor to life meaning rather than the reverse [15]. As other scholars have found, “Attitude is the central issue that predicts, explains and continuously influences behavior and determines emotion, thought and behavioral style” [16,17]. Attitudes tend to form earlier and are more stable, influencing how individuals interpret life events, including their search for meaning.
Therefore, we propose the following research framework: aging attitudes affect life meaning and, consequently, psychological vulnerability. Reviewing the existing literature, it is clear that there are many studies on the relationship between any two of these constructs, but there is a lack of comprehensive and in-depth discussion that encompasses all three. The interaction mechanism between the three has not yet been demonstrated, and there is a lack of discussion on the special group of elderly patients with comorbidities.
Based on this, we conducted a cross-sectional survey on the psychological vulnerability, aging attitudes, and life meaning of elderly patients with chronic diseases. This study aims to provide a reference for identifying and reducing the psychological vulnerability of elderly patients with comorbidities by analysing the internal relationship between psychological vulnerability and aging attitudes and life meaning. This study assumes that aging attitudes have a direct impact on psychological vulnerability, with these attitudes also having an indirect impact on psychological vulnerability through the sense of life meaning. The purpose of this study is to verify the above hypothesis and provide a basis for the clinical implementation of targeted crisis intervention and formulation of aging policies.
This cross-sectional study was conducted in 2022. A total of 685 elderly inpatients and outpatients at Renmin Hospital of Wuhan University between July and December 2022 were selected using the simple random sampling method. We first conducted a preliminary test in 6 wards of the geriatrics department and surveyed a total of 103 patients. The maximum number of items of the Attitudes to Aging Questionnaire (AAQ) in the research instrument was 24, with 103 cases in the pre-test, and the standard deviation (σ) of the data in this group was 5.28. The attendant formula (n = [uα/2σ/δ]2) was calculated according to the sample size of a cross-sectional survey [18] (deviation σ = 0.475, α = 0.05, uα/2 = 1.96), with the calculated sample size (n) equal to 475. Considering that 20% of the questionnaire may be lost to follow-up, the initial sample size of this study was 570 cases. Convenience sampling was then used to select participants for this study, focusing on both inpatients and outpatients. Data collection was conducted by clinical teachers and undergraduate internship students, who rotated across various departments to gather a wide range of responses. Inpatients were surveyed in the afternoon following their treatments, ensuring that they were in a suitable state to respond, whereas outpatient surveys were conducted based on the participants’ individual rest times. The Chinese version of the Psychological Vulnerability Scale (C-PVS) developed by Guo et al. [19–21], the AAQ, the Chinese Meaning in Life Questionnaire (C-MLQ) and a sociodemographic questionnaire were used for the analysis. A total of 685 questionnaires were sent out, and 602 questionnaires were collected, with an effective recovery rate of 87.88%. The inclusion criteria included patients (1) aged ≥60 years old; (2) with no mental illness or other disease affecting intelligence and expression; (3) and who were able to communicate with people normally. The exclusion criterion was patients with cognitive dysfunction and behavioural disorders. Informed consent was signed by the selected participants and their families.
Due to the large workload of this questionnaire, a questionnaire research team was formed. The team members included the general director of clinical teaching and teaching team leaders of internal medicine and the general director of clinical teaching and teaching team leaders of geriatrics. The questionnaire research team recruited clinical teachers and undergraduate internship students as investigators. To ensure that the collection and entry of the questionnaires were completed under homogeneous quality, the questionnaire research team members were responsible for training the investigators.
Questionnaire recovery and quality control
The inclusion and exclusion criteria were strictly implemented to ensure that the patients’ data were true and credible, with the patients’ general data collected and checked to ensure that it matched the patients’ identity information. Five trained staff were selected to conduct a pre-survey of patients who met the inclusion requirements. The questionnaire was adjusted according to the survey results and patient feedback. The survey time was controlled at approximately 30 min. Before the investigation, the general information questionnaire and the filling methods and requirements of the scale were explained in detail to the respondents. After signing the informed consent form, the respondents were asked to complete the questionnaire independently according to the actual situation. Those who could not complete it by themselves due to disease-related reasons were assisted and recorded by the investigator on an individual basis. Following data recovery, the members of the research group reviewed and checked whether there were any omissions; if there were, they were subsequently supplemented. At the same time, the research group used periodic and summary reports to regularly provide feedback on common or specific problems found in the research process, and they promptly analysed and resolved any related issues. A double-entry data and review process was conducted to ensure the accuracy of the data.
The members of the investigation group explained the completion rules, precautions and unified guidance, and they dealt with on-the-spot recovery and inspection.
In this research, four questionnaires were used: a sociodemographic questionnaire, the AAQ, the C-MLQ, and the C-PVS. The sociodemographic questionnaire was designed by the research group, and the other scales were authorized for use. A cross-sectional survey was conducted with questionnaires. A unified guide was used to explain the purpose of the research survey and obtain informed consent. 685 questionnaires were received, and 602 valid questionnaires were collected, with an effective recovery rate of 87.88%.
Sociodemographic questionnaire
The sociodemographic variables assessed included gender, age, degree of education, marital status, living condition, payment of medical expenses, income, exercise situation, medical treatment situation, chronic diseases, oral medication and self-report health condition.
Attitudes to aging questionnaire
The AAQ was used to evaluate people’s attitudes to aging [22,23]. The questionnaire was compiled by the Chinese scholars Huang et al. in 2010 and included three dimensions: psychosocial loss, physiological change, and psychological gain. The internal consistency coefficients of the 3 dimensions were 0.746, 0.785, and 0.716, respectively. The participants were asked to respond to 24 statements, such as ‘As people get older, they are better able to deal with life’s problems’ and ‘Old age is an advantage’. The scale covered 24 items and used a 5-point Likert scale, with options of 1 (totally wrong), 2 (somewhat wrong), 3 (does not matter), 4 (somewhat right), and 5 (totally accurate). The score for the AAQ ranged from 24 to 120. A higher score indicated more positive aging attitudes. It is the most commonly used measurement tool for studying the aging attitudes of the elderly in China, which accords with the domestic culture.
Chinese life meaning questionnaire
Based on Steger’s Sense of Meaning in Life Scale [24], and combined with Chinese clinical practice, Chinese scholars Lu et al. adapted the scale into a localised life meaning measurement scale in 2010 following cultural adjustments [25]. The C-MLQ included two dimensions: having a sense of life meaning and seeking a sense of life meaning. The participants were asked to respond to nine statements, such as ‘I understand the meaning of my life’ and ‘I am always trying to find the purpose of my life’. The scale covered 9 items using a 7-point Likert scale, with options of 1 (strongly disagree), 2 (somewhat disagree), 3 (slightly disagree), 4 (not sure), 5 (slightly agree), 6 (somewhat agree) and 7 (strongly agree). The score for the C-MLQ ranged from 9 to 63; a higher score indicated a better sense of life meaning. This scale had good reliability and validity. Its Cronbach’s coefficient was 0.71, and the Cronbach’s coefficient of the two dimensions were 0.81 and 0.72, respectively.
Chinese meaning in psychological vulnerability scale
The C-PVS, compiled by Guo et al. [19–21], was specifically created and validated for use in Chinese populations, and it assessed psychological vulnerability by focusing on emotions and cognitions that may predispose individuals to psychological distress. The C-PVS was a culturally tailored tool designed to capture the unique aspects of psychological vulnerability within the Chinese context. The scale was divided into four dimensions: challenge, coping, support and resilience. The scale covered 22 items using a 5-point Likert scale, with options of 1 (strongly disagree), 2 (somewhat disagree), 3 (not sure), 4 (somewhat agree) and 5 (strongly agree). The score for C-PVS ranged from 22 to 110, and a higher total score indicated greater psychological vulnerability. The internal consistency reliability of the total questionnaire was 0.92, and the retest reliability was 0.85. It took approximately 5–10 min to complete the entire questionnaire. The questionnaire is suitable for individuals ranging from students to the elderly and has good universality. All scales used in the study have been authorised for use by the original authors.
This study was approved by the Ethics Committee of Renmin Hospital of Wuhan University (Ethical number: IRB2022019). Before the questionnaire survey, the purpose, significance and specific process of the study were explained to the patients. All personal information involved in the questionnaire was confidential and was only for scientific research sharing. All participants were informed that they had the right to withdraw from the study at any time.
Analyses were performed using SPSS V25.0 (IBM, Armonk, NY, USA) and AMOS V24.0 (IBM, Armonk, NY, USA) software. Pearson’s correlation analysis and linear regression analysis were used to examine the relationship between psychological vulnerability, aging attitudes, and life meaning. A p-value of < 0.05 was considered statistically significant. The structural equation analysis model was established using Amos V24.0 software. Error variables were included in the model to account for unobserved factors influencing the relationships between psychological vulnerability, aging attitudes, and life meaning. These variables helped capture the complexity of the data.
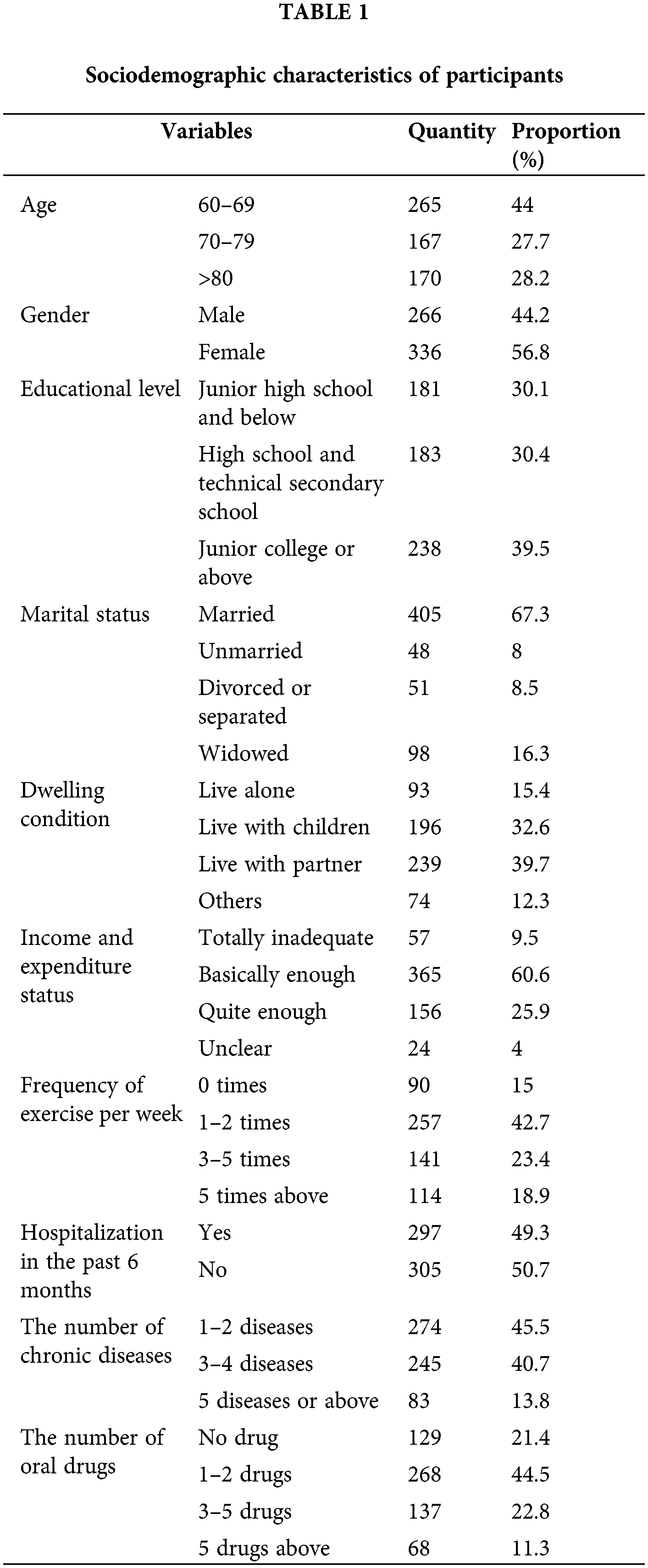
Sociodemographic characteristics
In this study, we collected elderly patients’ data, including age, gender, education level, marital status, dwelling condition, income condition, exercise frequency, hospitalisation status, chronic diseases and oral drug status. Details of the sociodemographic characteristics are shown in Table 1. We analysed the data from 602 respondents, of whom 336 (56.8%) were women and 266 (44.2%) were men, with an average age of 73.15 ± 11.15 years (range: 60–91 years).
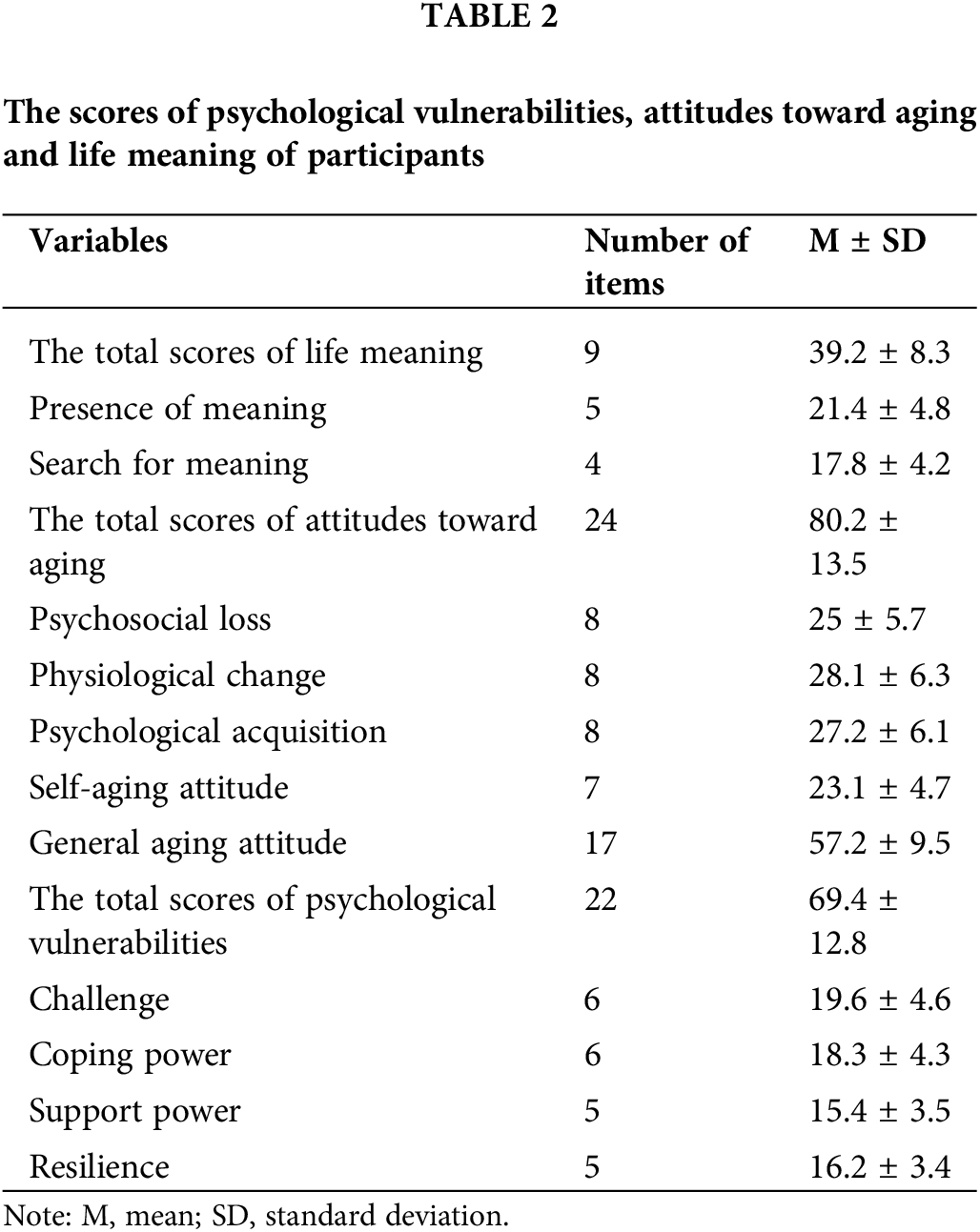
The status quo of psychological vulnerability, aging attitudes and life meaning
The total score of psychological vulnerability was 69.4 ± 12.8, the total score of aging attitudes was 80.2 ± 13.5 and the total score of life meaning was 39.2 ± 8.3. The scores of each dimension are shown in detail in Table 2.
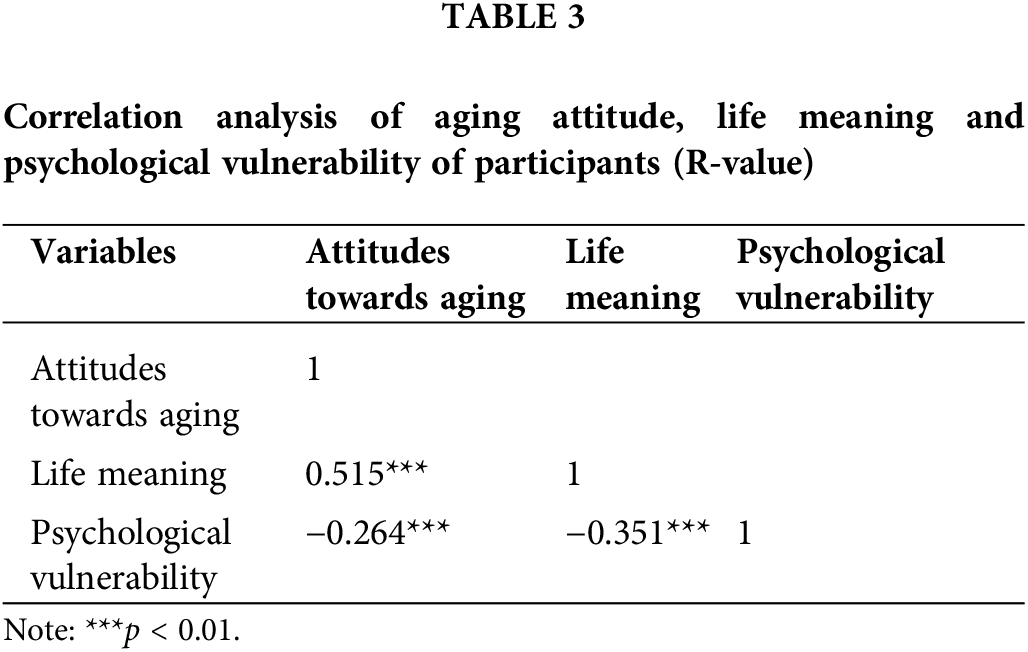
Correlation analysis of psychological vulnerability with aging attitudes and life meaning
Pearson’s correlation analysis showed that the psychological vulnerability in elderly patients with comorbidities was negatively correlated with life meaning (r = −0.351; p < 0.01), psychological vulnerability was negatively correlated with aging attitudes (r = −0.264; p < 0.01) and aging attitudes were positively correlated with life meaning (r = 0.515; p < 0.01) (Table 3).
Partial mediating effect of life meaning between psychological vulnerability and aging attitudes in elderly patients with comorbidities
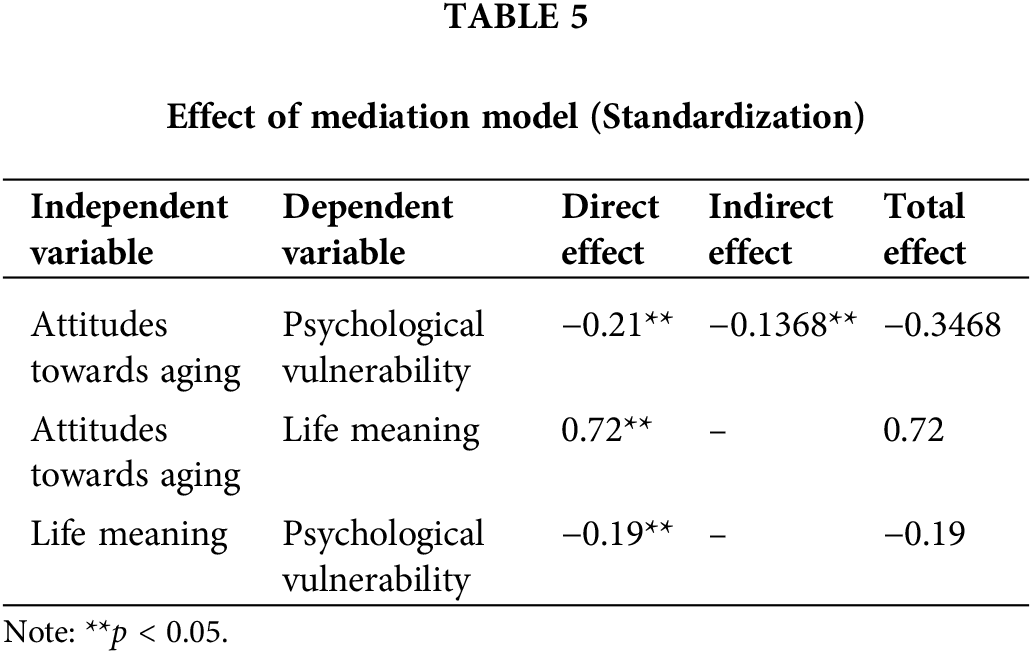
Based on correlation analysis, a hypothetical model with crisis vulnerability as the dependent variable (Y), aging attitudes as the independent variable (X), and life meaning as the mediating variable (M) was established, as shown in Fig. 1. The structural equation model was constructed using Amos V24.0 software, and the model was tested and modified. Model fitting results showed that all fitting indexes were within the reference range, indicating that the model was ideal, as shown in Table 4. The model suggested that a sense of life meaning played a mediating role in the relationship between aging attitudes and psychological crisis vulnerability (β = 3.070, p < 0.01). When the indirect effect was greater than the direct effect, it indicated that the intermediary variable had an influence; attention must be paid to the intermediary effect variable. In this study, the indirect effect was greater than the direct effect, and the ratio of the intermediary effect to the total effect was −0.1368/−0.3468 = 39.44%. Therefore, it is necessary to attach importance to the sense of life meaning as the intermediary variable. The interaction between the variables is shown in Table 5.
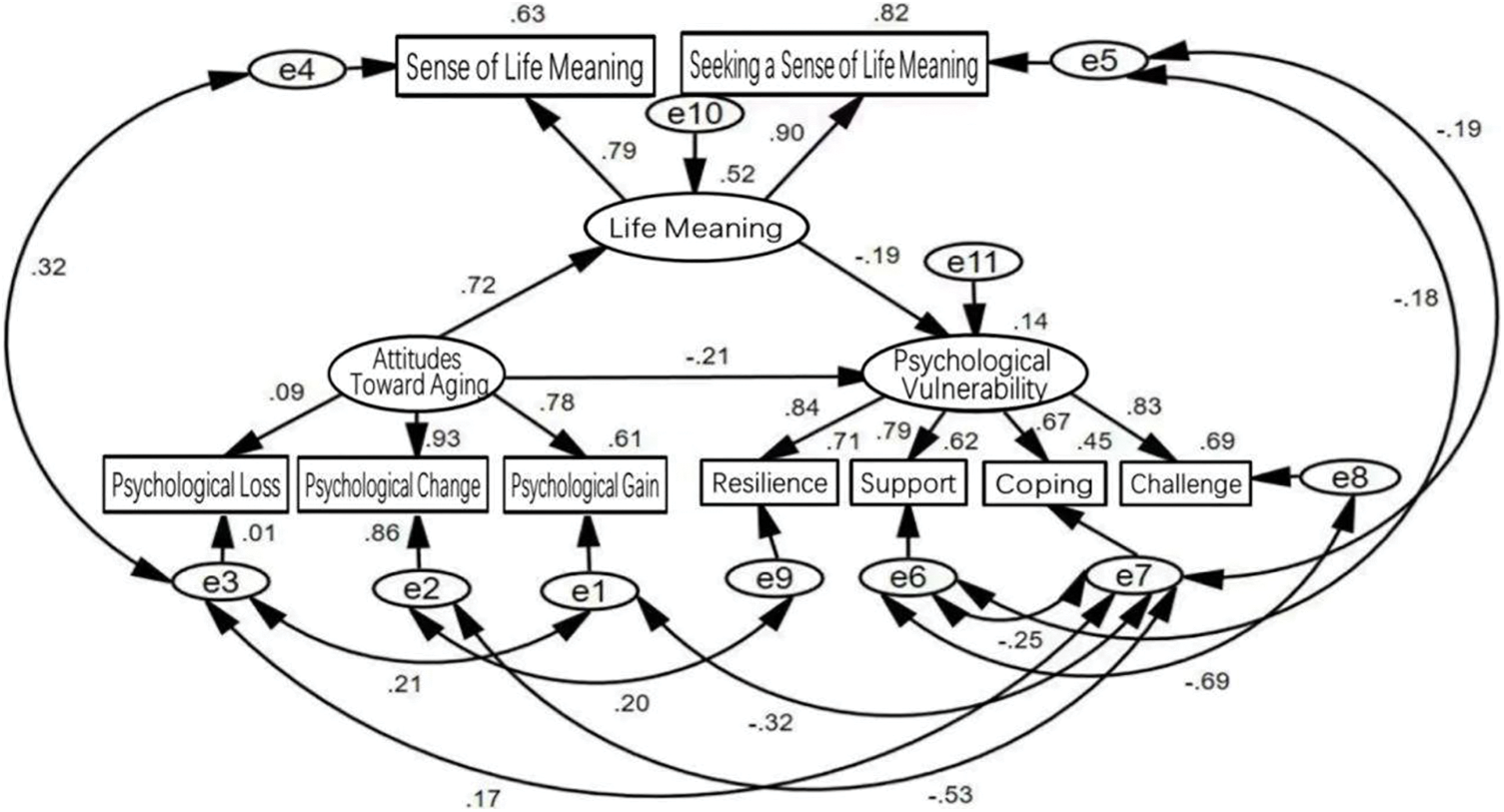
Figure 1: The mediating effect model of life meaning on attitudes towards aging and psychological vulnerability

Status of the psychological vulnerability of elderly patients with comorbidities
In this study, the psychological vulnerability of elderly patients with comorbidities was 69.4 ± 12.8, a score that could be considered relatively low when compared with the scale’s maximum score of 110, which suggested that their psychological vulnerability was at the lower level. These findings suggest that elderly individuals with comorbidities have a limited ability to cope with psychological crises, which is consistent with findings by Silveira et al. [26]. Their psychological vulnerability requires further attention, as it is a key predictor of crises, which become more frequent with age [27,28]. Assessing this vulnerability can help in early intervention, providing necessary psychological support and defences. It is worth noting that elderly people with comorbidities are more prone to psychological crises. Given their physical and mental challenges, along with limited income and social support, targeted psychological care is essential to help these individuals manage crises and improve their quality of life in old age.
Correlation between psychological vulnerability, aging attitudes and life meaning
This study found that psychological vulnerability in elderly patients is linked to their aging attitudes and sense of life meaning, acting as psychological protective mechanisms. In addition, vulnerability to a mental crisis is the behavioral projection of mental health status, which belongs to the category of mental mapping [29]. Therefore, aging attitudes and a sense of the meaning of life are important parts of the assessment of patients’ mental health. Abell et al. [30,31] found that positive experiences enhanced the ability of elderly patients with cancer to cope with crises, whereas Silveira et al. [32] identified resilience as a key factor in reducing psychological vulnerability. Therefore, healthcare providers must monitor emotional changes in elderly patients and promote positive aging attitudes through media, community initiatives, and activities that foster a sense of achievement. Policymakers should also work to create an aging-friendly society that values the contributions of the elderly.
The mediating effect of life meaning on psychological vulnerability and aging attitudes
This study indicates that life meaning has a partial mediating effect on psychological vulnerability and aging attitudes (β = 0.182, p < 0.01), with the mediating effect accounting for 56.12% of the total effect. This indicates that aging attitudes not only directly predict the psychological vulnerability of the elderly with comorbidities but also indirectly affect the psychological crisis vulnerability of such individuals through the sense of life meaning. The sense of life meaning is the degree to which an individual understands and is aware of the meaning of their own life. The degree of purpose, mission and primary goal refers to the individual’s understanding and pursuit of purpose and goals in life. A good sense of life’s meaning helps the elderly to appreciate life more and have confidence in living and themselves [33]. A positive life attitude is an important psychological protection mechanism, helping the elderly to be more able to face crises. Based on this, attention must be paid to the mediating effect of a sense of life meaning on aging attitudes and psychological vulnerability, providing a new way to conduct relevant interventions for psychological vulnerability [34].
The urgent need to strengthen the assessment of the psychological vulnerability of the elderly and to pay attention to the awareness of early warning and prevention
Psychological crisis assessment and intervention often focus on adolescents; however, negative life events significantly impact elderly patients, correlating strongly with chronic diseases (correlation coefficient: 0.592). Negative life events are a form of stressor, that directly affects the comprehensive health level of the elderly through social function, mental health, and disease outcome, and early assessment and warning have a certain buffer effect in this regard [35]. The C-PSV scale, devised by Guo Jing, and validated in community settings, requires further study for effective early warning and intervention [21]. It is recommended to establish a coordinated assessment and intervention system, set up specialized teams, and develop an information resource database for early crisis detection, focusing on high-risk elderly individuals, families, and communities.
This study has several limitations. First, the sample was limited to elderly patients from Renmin Hospital of Wuhan University, which may affect the generalisability of the findings to other regions and healthcare settings. Second, the cross-sectional design prevented the observation of changes over time, limiting the analysis of long-term trends. Additionally, reliance on patient self-reporting introduces the risk of subjectivity and recall bias, particularly regarding the measurement of psychological vulnerability through the C-PVS, which may reflect perceived rather than actual vulnerability. While validated in the Chinese context, the C-PVS’s applicability in global research remains uncertain due to cultural differences. Further research is needed to explore the complex relationships between psychological vulnerability, aging attitudes and life meaning, as well as their long-term impact on mental health. Finally, while our model fits the data well, further refinement could reduce the dependence on error terms.
The above factors may have certain limitations and deviations in the interpretation and promotion of the research results.
Improving these factors can reduce vulnerability, as positive experiences enhance crisis resilience. Further comparisons of the elderly with different levels of psychological vulnerability could reveal that individuals with higher psychological vulnerability tend to have more negative aging attitudes and life meaning. Therefore, for the elderly with high psychological vulnerability, it is necessary to pay attention to their aging attitudes and their perception of life and to strengthen psychological support and intervention to improve their resistance to psychological crisis and their quality of life. The early identification and intervention of psychological vulnerability and attention to mental health are essential to promote the comprehensive health of elderly patients.
This study indicates that the psychological vulnerability of elderly patients with comorbidities is at a low to medium level and is related to the sense of life meaning and aging attitudes. Aging attitudes are the elderly’s experiences of being older, including both positive and negative experiences. The negative experience of aging refers to the negative feelings of physical, psychological, and social loss caused by aging. Positive experiences are the positive feelings and experiences associated with old age, such as good health, consistent exercise, wisdom, and growth. Positive aging attitudes help older people understand aging correctly, face it more positively, and adopt a healthier lifestyle. Elderly people with comorbidities suffer from a variety of chronic diseases, and their fragility regarding psychological crises is often higher, which requires greater attention from medical staff. Therefore, paying attention to the mental crisis fragility and aging attitudes of the elderly with comorbidities will be the focus of future research to improve their quality of life and guide them to establish positive aging attitudes.
Acknowledgement: The authors sincerely thank Jing Guo and other teachers for authorizing the questionnaire, which made the research possible. Many thanks to Renmin Hospital of Wuhan University for its strong support of this research. The authors also sincerely appreciate the hard work of every team member and the active cooperation of all the patients involved in the study.
Funding Statement: 2023 Hubei Provincial Key Laboratory Open Project-Nursing Special Project: 2023KFH017; Current Status Survey and Interventional Research on Alexithymia in Elderly Cancer Patients (Chaired by Lili Zhang); Wuhan University Clinical Nursing Special Research Cultivation Fund Project: LCHL202307; Constructing a Long-Term Care Model Based on Narrative Transport Model to Identify and Reduce the Vulnerability of Psychological Crises in Elderly Patients with Comorbidities (Chaired by Lili Zhang); 2022 Hubei Provincial Key Laboratory Open Project-Nursing Special Project: 2022KFH030; Empirical Study on the Construction and Application of a Frailty Risk Warning Model for Hospitalized Elderly Patients (Chaired by Jiaojiao Wu).
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: Dou Fu, Jiaojiao Wu, Lili Zhang; data collection: Dou Fu, Jiaojiao Wu, Lili Zhang, Xu Xu, Hui Cheng, Xiaojie Ma, Doudou Lin; analysis and interpretation of results: Lili Zhang, Xiangying Xie, Xinmei Wang, Xiangying Shen, Shanshan Liu, Xu Xu; draft manuscript preparation: Dou Fu and Jiaojiao Wu. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data will be provided upon request to the corresponding author.
Ethics Approval: This study was approved by the Ethics Committee of Renmin Hospital of Wuhan University (Ethical number: IRB2022019). All participants signed the informed consent in this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Tan X, Zhang Y, Shao H. Healthy China 2030, a breakthrough for improving health. Glob Health Promot. 2019;26(4):96–9. doi:10.1177/1757975917743533. [Google Scholar] [PubMed] [CrossRef]
2. Guo X, Zhao B, Chen T, Hao B, Yang T, Xu H. Multimorbidity in the elderly in China based on the China Health and Retirement Longitudinal Study. PLoS One. 2021;16(8):e0255908. doi:10.1371/journal.pone.0255908. [Google Scholar] [PubMed] [CrossRef]
3. Chen YT, Gao XT, Chen ZL, Huang SH. Meaning in life and mental health of the elderly based on the dual-factor model: mediating effects of attitudes toward aging. Stud Psych Behav. 2022;20(1):88–95. doi:10.12139/j.1672-0628.2022.01.013. [Google Scholar] [CrossRef]
4. Eplov LF, Petersen J, Jørgensen T, Johansen C, Birket-Smith M, Lyngberg AC, et al. The mental vulnerability questionnaire: a psychometric evaluation. Scand J Psychol. 2010;51(6):548–54. doi:10.1111/j.1467-9450.2010.00834.x. [Google Scholar] [PubMed] [CrossRef]
5. Sinclair VG, Wallston KA. The development and validation of the Psychological Vulnerability Scale. Cognit Ther Res. 1999;23(2):119–29. doi:10.1023/A:1018770926615. [Google Scholar] [CrossRef]
6. Chen L, Guo W, Perez C. The effect of aging attitudes on the quality of life of older adults in China. Res Aging. 2021;43(2):96–106. doi:10.1177/0164027520948192. [Google Scholar] [PubMed] [CrossRef]
7. Demirci I, Ekşi H, Ekşi F, Kaya Ç. Character strengths and psychological vulnerability: the mediating role of resilience. Curr Psychol. 2021;40(11):5626–36. doi:10.1007/s12144-019-00533-1. [Google Scholar] [CrossRef]
8. Ho IS, Azcoaga-Lorenzo A, Akbari A, Black C, Davies J, Hodgins P, et al. Examining variation in the measurement of multimorbidity in research: a systematic review of 566 studies. Lancet Public Health. 2021;6(8):e587–97. doi:10.1016/S2468-2667(21)00107-9. [Google Scholar] [PubMed] [CrossRef]
9. Sacco RG. Re-envisaging the eight developmental stages of erik erikson: the fibonacci life-chart method (FLCM). J Educ Dev Psychol. 2013;3(1):140–6. doi:10.5539/jedp.v3n1p140. [Google Scholar] [CrossRef]
10. Erikson EH. Identity and the life cycle. USA: International Universities Press; 1959. [Google Scholar]
11. Butler RN. The life review: an interpretation of reminiscence in the aged. Psychiatry. 1963;26(1):65–76. doi:10.1080/00332747.1963.11023339. [Google Scholar] [PubMed] [CrossRef]
12. Park N, Peterson C, Szvarca D, Vander Molen RJ, Kim ES, Collon K. Positive psychology and physical health: research and applications. Am J Lifestyle Med. 2014;10(3):200–6. doi:10.1177/1559827614550277. [Google Scholar] [PubMed] [CrossRef]
13. Xu X, Xu Y, Zhao J, Ye P, Yu M, Lai Y, et al. Good personality and subjective well-being: presence of meaning in life and perceived social support as mediators. Int J Environ Res Public Health. 2022;19(21):14028. doi:10.3390/ijerph192114028. [Google Scholar] [PubMed] [CrossRef]
14. Sargent-Cox KA, Anstey KJ, Luszcz MA. The relationship between change in self-perceptions of aging and physical functioning in older adults. Psychol Aging. 2012;27(3):750–60. doi:10.1037/a0027578. [Google Scholar] [PubMed] [CrossRef]
15. Shiah YJ, Chang F, Chiang SK, Lin IM, Tam WCC. Religion and health: anxiety, religiosity, meaning of life and mental health. J Relig Health. 2015;54(1):35–45. doi:10.1007/s10943-013-9781-3. [Google Scholar] [PubMed] [CrossRef]
16. Kim YJ, Kang I, Lee CS. A study on attitudes toward older adults: comparative analysis of young, midlife, and older adults. J Famil Better Life. 2004;22(1):65–75. [Google Scholar]
17. Suh S, Choi H, Lee C, Cha M, Jo I. Association between knowledge and attitude about aging and life satisfaction among older Koreans. Asian Nurs Res. 2012;6(3):96–10. doi:10.1016/j.anr.2012.07.002. [Google Scholar] [PubMed] [CrossRef]
18. Serdar CC, Cihan M, Yücel D, Serdar MA. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochemia Medica. 2021;31(1):010502. doi:10.11613/BM.2021.010502. [Google Scholar] [PubMed] [CrossRef]
19. Guo J, Wang Y, Ji LL, Jia LP, Lu GH. Development and validation of psychological crisis vulnerability scale. Stud Psych Behav. 2018;16(6):847–53. doi:10.3969/j.issn.1672-0628.2018.06.017. [Google Scholar] [CrossRef]
20. Guo J, Ji LL, Jia LP, Yu LR, Lu GH. Mediation of psychological vulnerability in the association between stressful life events and psychological crisis among college students. Chin J School Health. 2019;40(1):104–6 (In Chinese). doi:10.16835/j.cnki.1000-9817.2019.01.028. [Google Scholar] [CrossRef]
21. Guo J, Wang Y, Song YP, Wang MM, Teng S, Lu GH. Preliminary revision and psychometric evaluation of Mental Vulnerability Questionnaire-Chinese Version in community adults. Chin J Public Health. 2019;35(2):129–33 (In Chinese). doi:10.11847/zgggws1119908. [Google Scholar] [CrossRef]
22. Laidlaw K, Kishita N, Shenkin SD, Power MJ. Development of a short form of the Attitudes to aging Questionnaire (AAQ). Int J Geriatr Psychiat. 2018;33(1):113–21. doi:10.1002/gps.4687. [Google Scholar] [PubMed] [CrossRef]
23. Huang YF, Wang DH, Liu YG. Application of attitudes to aging questionnaire (AAQ) among chinese aged adults. Chin J Clin Psych. 2010;18(4):447–50 (In Chinese). [Google Scholar]
24. Steger MF, Frazier P, Oishi S, Kaler M. The meaning in life questionnaire: assessing the presence of and search for meaning in life. J Couns Psychol. 2006;53(1):80. doi:10.1037/0022-0167.53.1.80. [Google Scholar] [CrossRef]
25. Lu SS, Gan YQ. Reliability and vaildity of the Chinese version of the meaning in life questionaire. Chin Ment Health J. 2010;24(6):478–82 (In Chinese). doi:10.3969/j.issn.1000-6729.2010.06.021. [Google Scholar] [CrossRef]
26. Silveira S, Hecht M, Adli M, Voelkle MC, Singer T. Exploring the structure and interrelations of time-stable psychological resilience, psychological vulnerability, and social cohesion. Front Psychiat. 2022;13:804763. doi:10.3389/fpsyt.2022.804763. [Google Scholar] [PubMed] [CrossRef]
27. Yu X, Liu S. Stressful life events and chinese older people depression: moderating role of social support. Front Public Health. 2021;9:768723. doi:10.3389/fpubh.2021.768723. [Google Scholar] [PubMed] [CrossRef]
28. Turana Y, Tengkawan J, Chia YC, Shin J, Chen CH, Park S, et al. Mental health problems and hypertension in the elderly: review from the HOPE Asia Network. J Clin Hypertens. 2021;23(3):504–12. doi:10.1111/jch.14121. [Google Scholar] [PubMed] [CrossRef]
29. Lajoie C, Poleksic J, Bracken-Roche D, MacDonald ME, Racine E. The concept of vulnerability in mental health research: a mixed methods study on researcher perspectives. J Empir Res Hum Res Ethics. 2020;15(3):128–42. doi:10.1177/1556264620902657. [Google Scholar] [PubMed] [CrossRef]
30. Abell AM. Physical health, attitudes toward menopause and aging, meaning in life, and their relationship to psychological distress in midlife women. Fielding Graduate University: USA; 2016. [Google Scholar]
31. Thielsch MT, Röseler S, Kirsch J, Lamers C, Hertel G. Managing pandemics-demands, resources, and effective behaviors within crisis management teams. Appl Psychol. 2021;70(1):150–87. doi:10.1111/apps.12303. [Google Scholar] [PubMed] [CrossRef]
32. Silveira S, Hecht M, Matthaeus H, Adli M, Voelkle MC, Singer T. Coping with the COVID-19 pandemic: perceived changes in psychological vulnerability, resilience and social cohesion before, during and after lockdown. Int J Environ Res Public Health. 2022;19(6):3290. doi:10.3390/ijerph19063290. [Google Scholar] [PubMed] [CrossRef]
33. Sallnow L, Smith R, Ahmedzai SH, Bhadelia A, Chamberlain C, Cong Y, et al. Report of the lancet commission on the value of death: bringing death back into life. Lancet. 2022;399(10327):837–84. doi:10.1016/S0140-6736(21)02314-X. [Google Scholar] [PubMed] [CrossRef]
34. Satici SA, Uysal R. Psychological vulnerability and subjective happiness: the mediating role of hopelessness. Stress Health. 2017;33(2):111–8. doi:10.1002/smi.2685. [Google Scholar] [PubMed] [CrossRef]
35. Phyo AZZ, Gonzalez-Chica DA, Stocks NP, Woods RL, Fisher J, Tran T, et al. Impact of economic factors, social health and stressful life events on physical health-related quality of life trajectories in older Australians. Qual Life Res. 2022 May;31(5):1321–33. doi:10.1007/s11136-021-03021-x. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools