
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

A Bifactor Analysis Approach to Construct Validity and Reliability of the Affective Exercise Experience Questionnaire among Chinese College Students
1
Body-Brain-Mind Laboratory, School of Psychology, Shenzhen University, Shenzhen, 518060, China
2
Department of Sport, Exercise & Health, University of Basel, Basel, Switzerland
3
Research Group Degenerative and Chronic Diseases, Movement, Faculty of Health Sciences Brandenburg, University of Potsdam,
Potsdam, Germany
4
Department of Psychological Sciences, Auburn University, Auburn, 36849, USA
5
School of Rehabilitation, Sport and Psychology, AECC University College, Bournemouth, BH5 2DF, UK
6
Center for Cognitive and Brain Health, Northeastern University, Boston, MA, 02115, USA
7
Beckman Institute, University of Illinois at Urbana-Champaign, Champaign, IL, 61820, USA
* Corresponding Author: Liye Zou. Email:
International Journal of Mental Health Promotion 2023, 25(9), 995-1008. https://doi.org/10.32604/ijmhp.2023.029804
Received 20 December 2022; Accepted 02 February 2023; Issue published 10 August 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Affective exercise experience as an emerging theoretical concept has great potential to provide a more nuanced understanding of individual factors that influence exercise behavior. However, concerning the Affective Exercise Experiences (AFFEXX) questionnaire, it has not been examined yet whether the structural score of the AFFEXX is a useful index to predict physical activity (refers to any bodily movement produced by skeletal muscles that requires energy expenditure). Furthermore, there is currently a gap in knowledge regarding the psychological mechanisms that can explain the relationship between affective exercise experiences and the level of physical activity (PA). In order to adress these gaps in the literature, we conducted two studies among Chinese collge students that aimed (i) to investigated whether the total score of the three AFFEXX-C constructs (antecedent appraisals, core affective exercise experiences, and attraction-antipathy towards exercise) is a relaible indicator that can be utilized in research and pratical settings and (ii) to evalute the specific psychological mechanisms that can explain the relationship between affective exercise experience and PA. In Study 1, we recruited 801 voluntary Chinese college students for bifactor and correlational analyses. In Study 2, 875 Chinese college students were enrolled to verify our findings from Study 1 and to explore the aforementioned mechanism. Results from the bifactor analyses supported our hypothesis that the total scores of the three AFFEXX-C constructs can be used among Chinese college students to establish a link with PA. Additionally, our results suggested that core affective exercise experiences and attraction-antipathy mediated the relationship between antecedent appraisals and the level of moderate-to-vigorous intensity PA. Therefore, measuring affective exercise experiences using the AFFEXX-C, specifically the total scores of each individual construct may be a useful approach to predict future PA levels.Keywords
There is solid evidence that regular engagement in physical activity (PA) is essential to maintain and promote physical and psychological health [1–3]. For instance, PA refers to any bodily movement produced by skeletal muscles that requires energy expenditure [4,5] and it consists of both structured (aerobic training and resistance training) and unstructured (walking the dog) PA, which can effectively enhance physical fitness [6] and metabolic health, with lack of PA being independently associated with morbidity and mortality [7–11]. Of note, many people do not regularly engage in PA [12–14]. In this regard, affective components towards PA may play an essential role in explaining why (or why not) individuals engage in PA [15,16]. For instance, numerous studies have shown that negative affective responses or affective valence (e.g., perceived fatigue) can influence future PA behavior [17–20]. Over time, these negative experiences can create an association that discourages the individual from engaging in PA, thus reducing regular or persistent exercise participation. Conversely, experiencing positive affect (e.g., pleasure, enjoyment, accomplishment) during physical exercise can promote future PA behavior [17,21].
In light of the growing interest in affective constructs toward physical exercise [16,22], it is fundamental to develop instruments that allow us to operationalize these theoretical constructs. Notably, previous research on the affective constructs has mostly focused on the immediate affective responses during or after a single bout of physical exercise, including measures of core affect [23] or enjoyment [24]. However, the previously mentioned measures only allow for a partial assessment of the influence of the affective component on PA, and thus a recent study proposed, developed, and evaluated an affective exercise experiences (AFFEXX) questionnaire [25], which assesses the individuals’ past exercise experiences. This scale is built on Affective-Reflective Theory (ART), which was proposed by Brand and Ekkekakis (2017) [16]. As a new dual-process theory, ART links reflective evaluation (referred to as reflection, rationality, and behavioral goals) and automatic affective evaluations (referred to as momentary, direct, and anticipated affect) in a single model, and further illustrates the role of these two factors on exercise motivation and exercise adherence. In particular, ART stresses that the automatic associations related to the object of evaluation or automatic affective valuation serve as the basis for reflective evaluation, controlled by individuals’ availability of self-control resources.
Based on ART theory, Ekkekakis and colleagues originally defined affective exercise experiences as a summary valanced concept, reflecting the history of associations between exercise in a person’s life and the attendant affective responses [25]. Furthermore, the AFFEXX questionnaire described a theoretical model which emphasizes the core constructs (i.e., core affective exercise experiences) and describes the relationships between it and the other two constructs (i.e., antecedent appraisals and attraction-antipathy). This model illustrated that the formation of exercise motivation is integrated by a three-order system: Antecedent-appraisals (contains 19 items within six lower-order factors), core affective exercise experiences (includes 12 items within three lower-order factors), and collectively shape attraction or antipathy toward physical exercise (consists of 5 items within a single factor) [25].
Recently, our group has developed a Chinese version of the affective exercise experiences questionnaire (AFFEXX-C) that has been validated and showed adequate reliability and validity among Chinese college students [26]. In the context of Chinese culture, the 30-item AFFEXX-C illustrated a slightly different three-layer model (specifically reflected in the decreased number of items and factors), which presented that the core affective exercise experiences (includes 9 items within three lower-order factors), which may be influenced by antecedent appraisals of exercise (contains 16 items within four lower-order factors), shape exercise motivation (shown in Fig. 1). Notably, a potential issue that makes a more widespread application of the AFFEXX-C difficult is that the AFFEXX-C was not originally developed so that total scores would be calculated and used for each of the three individual constructs (i.e., antecedent appraisals, core affective exercise experiences, and attraction-antipathy). Instead, scores are calculated for each of the lower-order factors within the three higher-order primary constructs of the AFFEXX-C (e.g., liking vs. disliking group exercise, interest vs. boredom, or pleasure vs. displeasure).
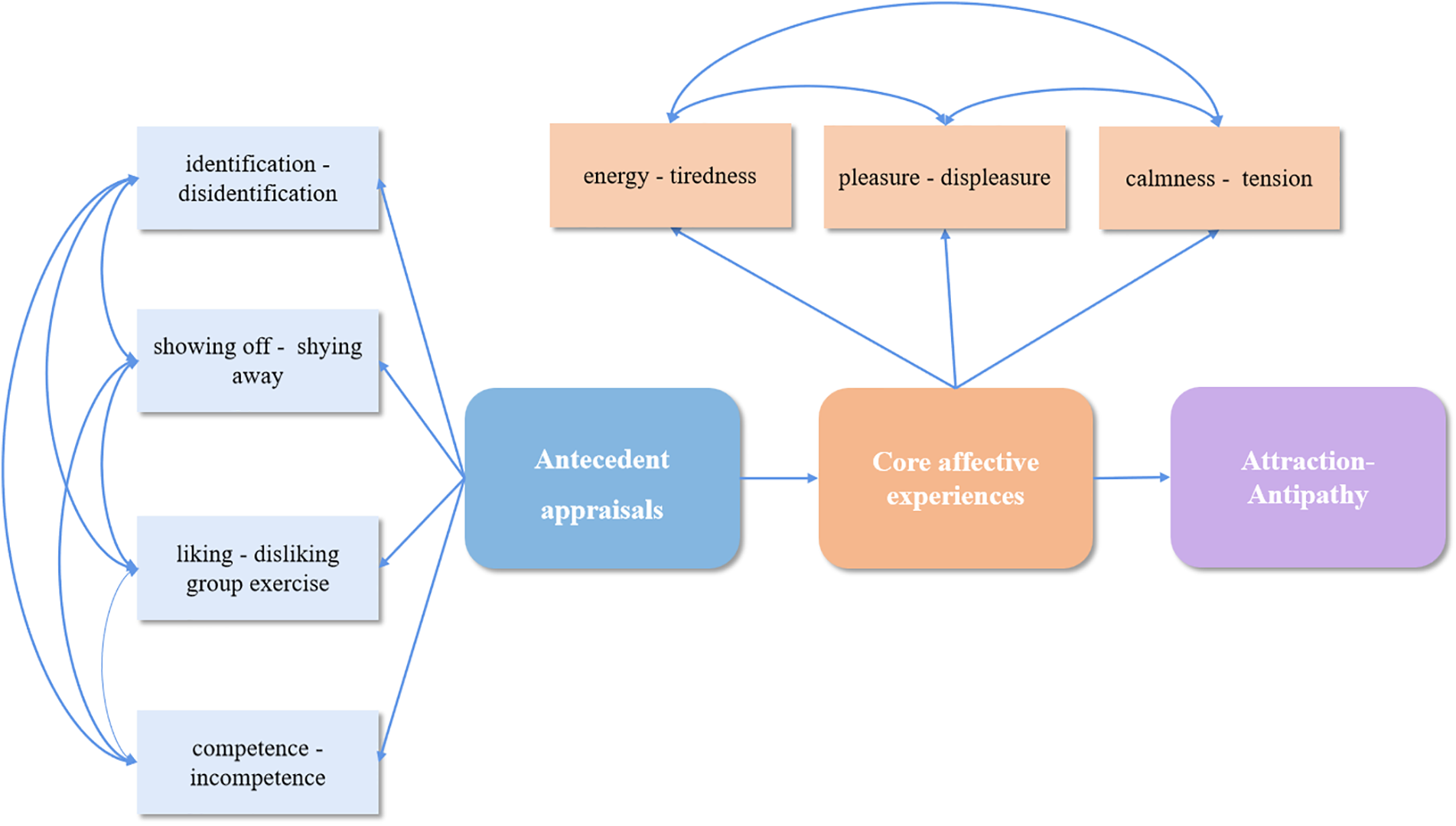
Figure 1: Illustration of the structural model of the AFFEXX-C (30 items).
Notes: The AFFEXX-C includes four factors of antecedent appraisals (i.e., identification vs. disidentification, showing off vs. shying away, liking vs. disliking group exercise, and competence vs. incompetence), three factors of core affective exercise experiences (i.e., pleasure vs. displeasure, energy vs. tiredness, and calmness vs. tension) and a single factor of attraction-antipathy towards exercise.
To tackle this problem, the current study employed a bifactor analysis approach, as this method emerging from the field of statistics has guided the interpretations of total scores from multifaceted inventories in the past decade, and has become popular in psychology and psychiatry research [27–30]. Two main reasons for using bifactor analysis are summarized below. First, a bifactor model allows researchers to verify the presence of a general factor. In bifactor analysis, the general factor is modeled independently from the individual group factors (i.e., specific sub-factors), and the unique contributions of both the group and general factors can be isolated, thus allowing for the simultaneous investigation of the overarching construct and the degree to which the lower order group factors are distinct from this general factor [31]. Second, compared to a general factor, the extent to which group factors appear redundant can support or oppose the use of total scores [32]. Accordingly, two (antecedent-appraisals and core affective exercise experiences) of the three constructs of the AFFEXX-C were respectively regarded as general factors, and their lower-order factors as group factors for bifactor analysis (two theoretical models of bifactor analyses of antecedent appraisals and core affective exercise experiences are presented in Figs. 2A and 2B, respectively). In contrast, the last of these three constructs, namely attraction-antipathy does not require bifactor analysis because it has no lower-order factors. Thus, this study aimed to determine whether the total scores of each individual construct are reliable and valid based on the results of bifactor analysis.
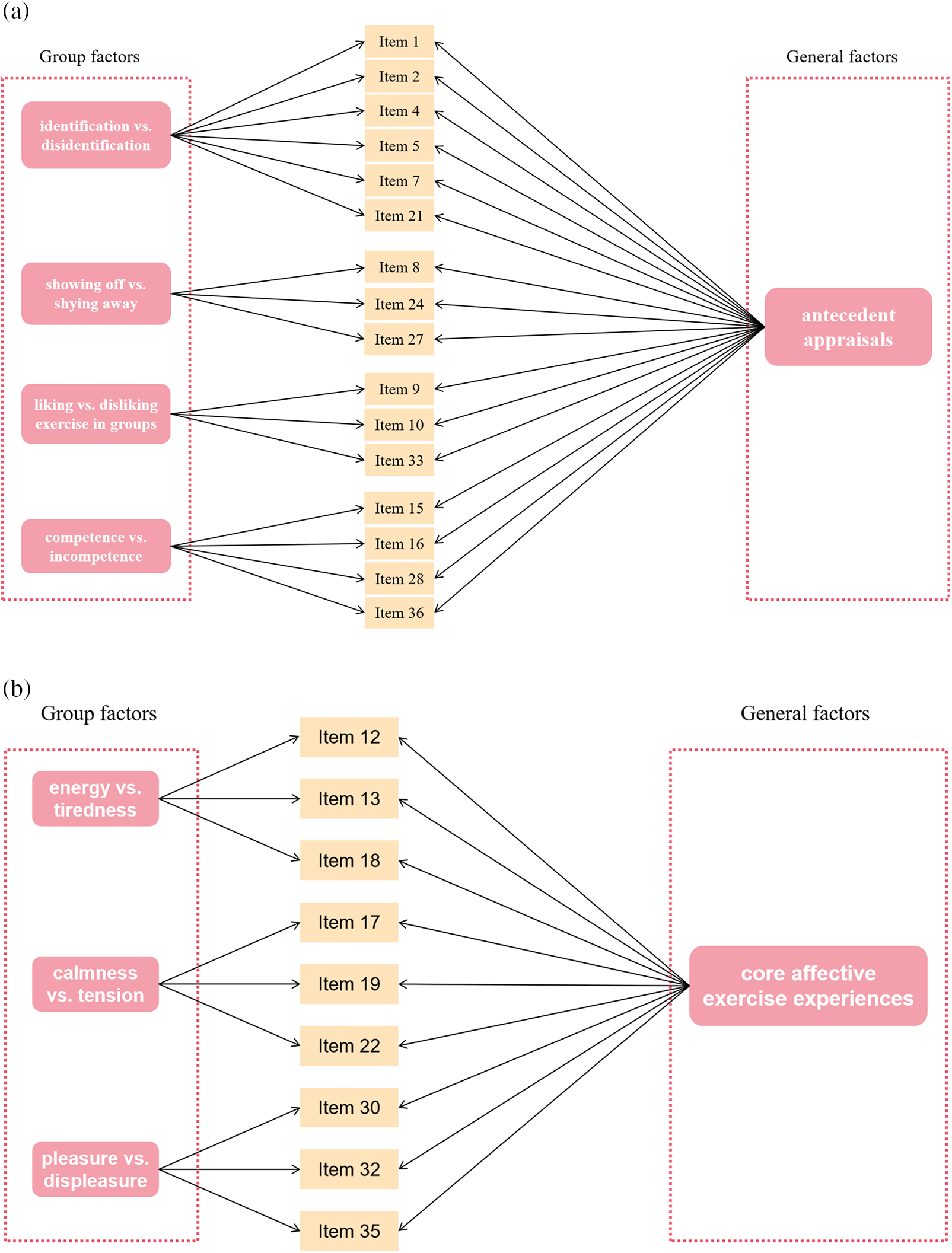
Figure 2: (A) Theoretical view for bifactor analysis of antecedent appraisals (16 items). (B) Theoretical view for bifactor analysis of core affective exercise experiences (9 items).
Despite the breakthrough development of an instrument that measures how past exercise experiences are associated with affective values associated with future exercise behaviors, there is a paucity of research on this topic. Although all of the factors of the AFFEXX-C were observed to be strongly correlated with PA level in previous research [25,26], the specific psychological mechanisms by which affective exercise experiences are connected with PA level still remains largely unclear. Based on existing literature [25], we hypothesize that (a) the total scores of each individual construct (i.e., antecedent appraisals, core affective exercise experiences, and attraction-antipathy) in this three-tiered framework would be positively related to PA level and (b) core affective experiences and attraction-antipathy would exert a mediating effect on antecedent appraisals and PA level. Thus, the second aim of this study was to elucidate the psychological mechanisms that can explain the significant relationship between affective exercise experiences and PA level.
In our two cross-sectional studies, healthy Chinese university students were recruited by word of mouth and by using WeChat. These students were asked to voluntarily complete an online questionnaire on the Questionnaire-Star platform. To confirm the stability of the results, data were collected in two different studies at different time points (Study 1 was conducted between June and July 2022, and Study 2 between November and December 2022). We excluded participants if they were (a) less than 18 years old or over 29 years old or (b) reported any psychiatric or neurological disorders, chronic diseases, or contraindications for PA. Additionally, the data of respondents that were indicative of inattentive responding (e.g., less than 3 min to complete this online questionnaire) or impractical response (e.g., time spent on exercise participation of > 16 h) [33,34] were also excluded (Study 1: n = 190, Study 2: n = 160) from the statistical analyses. According to these criteria, 801 participants were included for data analyses in Study 1 and 875 in Study 2. The research procedures of our studies were approved by the ethics committee of Shenzhen University (PN-202200026).
The Chinese version of the affective exercise experiences questionnaire (AFFEXX-C) was used to evaluate the affective exercise experiences of college students [26], which was originally developed by Ekkekakis and colleagues [25]. The AFFEXX-C consists of 30 items and 8 factors assessing three constructs, namely antecedent appraisals (four factors), core affective exercise experiences (three factors), and attraction-antipathy (single factor). Each item was scored on a 7-point Likert scale ranging from 1 (“if the statement on the left perfectly matches what you would say”) to 7 (“if the statement on the right perfectly matches what you would say”). Higher scores on each factor (average scores of subordinate items) indicate a more positive level of these three constructs (referred to better antecedent appraisals and core affective exercise experiences, and more attraction towards exercise). This instrument had sound psychometric properties among Chinese college students in a previous study from our research group, with all Cronbach’s α > 0.80 [26]. The Cronbach’s coefficients in the present studies varied between 0.84 and 0.93.
The level of habitual physical activity was assessed using the International Physical Activity Questionnaire-Short Form (IPAQ-SF), which consists of 7 items [34]. This scale reported good psychometric properties in the Chinese population [35]. Participants indicate their engagement in vigorous PA (VPA), moderate PA (MPA), and walking in the last seven days. The level of habitual PA was quantified by weighting each type of activity following the energy requirements defined in metabolic equivalents (METs) and expressed as MET-min per week (MET level * minutes of activity * events per week) [36]. The total level of PA is calculated based on the sum of the three intensity levels of PA. Additionally, the level of moderate-to-vigorous PA (MVPA, calculated by the sum of the VPA and MPA) was used as an indicator in the present study. The IPAQ-SF has good test-retest reliability in Chinese populations, with ICCs of 0.75 to 0.93 for the different PA parameters [35].
Statistical analyses were performed using IBM SPSS 27.0 (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp.) and MPlus 8 [37]. In Study 1, descriptive statistics were calculated (e.g., mean and standard deviations) and t-tests were conducted to explore sex-related differences. To examine whether the total scores of the three higher-order constructs of the AFFEXX-C can be used, we first calculated the average scores of the subordinate lower-order factors as the scores of the two constructs (excludes the single factor construct of attraction-antipathy). Secondly, four competing models for antecedent appraisals (presented in Fig. 3A) were tested in Study 1 using confirmatory factor analysis (CFA) following the guidelines outlined in [38]. Robust maximum likelihood (MLR) estimation was used to test all models. Specifically, the first model was a one-factor model in which all 16 items were loaded onto the same general factor (i.e., antecedent appraisals). The second model was a correlated four-factor model, with three items loading onto each factor. For the third model, lower-order factor correlations were removed from the lower-order four-factor model and these four factors were allowed to load onto a higher-order factor (i.e., antecedent appraisals). Of particular interest in the present study, the final model tested was a bifactor model, in which both a general factor and four lower-order factors were included—note all five factors are now first-order factors. The correlations between all factors were fixed to zero. Likewise, four competing models for core affective exercise experiences were also examined using CFA. The specific steps were similar to those mentioned above (shown in Fig. 3B). Additionally, the CFA of attraction-antipathy was also tested. To further test the validity of these bifactor models, standardized factor loadings for each item onto the general factor and the specific sub-factors were assessed. In Study 2, four competing models for antecedent appraisals and core affective exercise experiences were repeated to verify the results from Study 1.
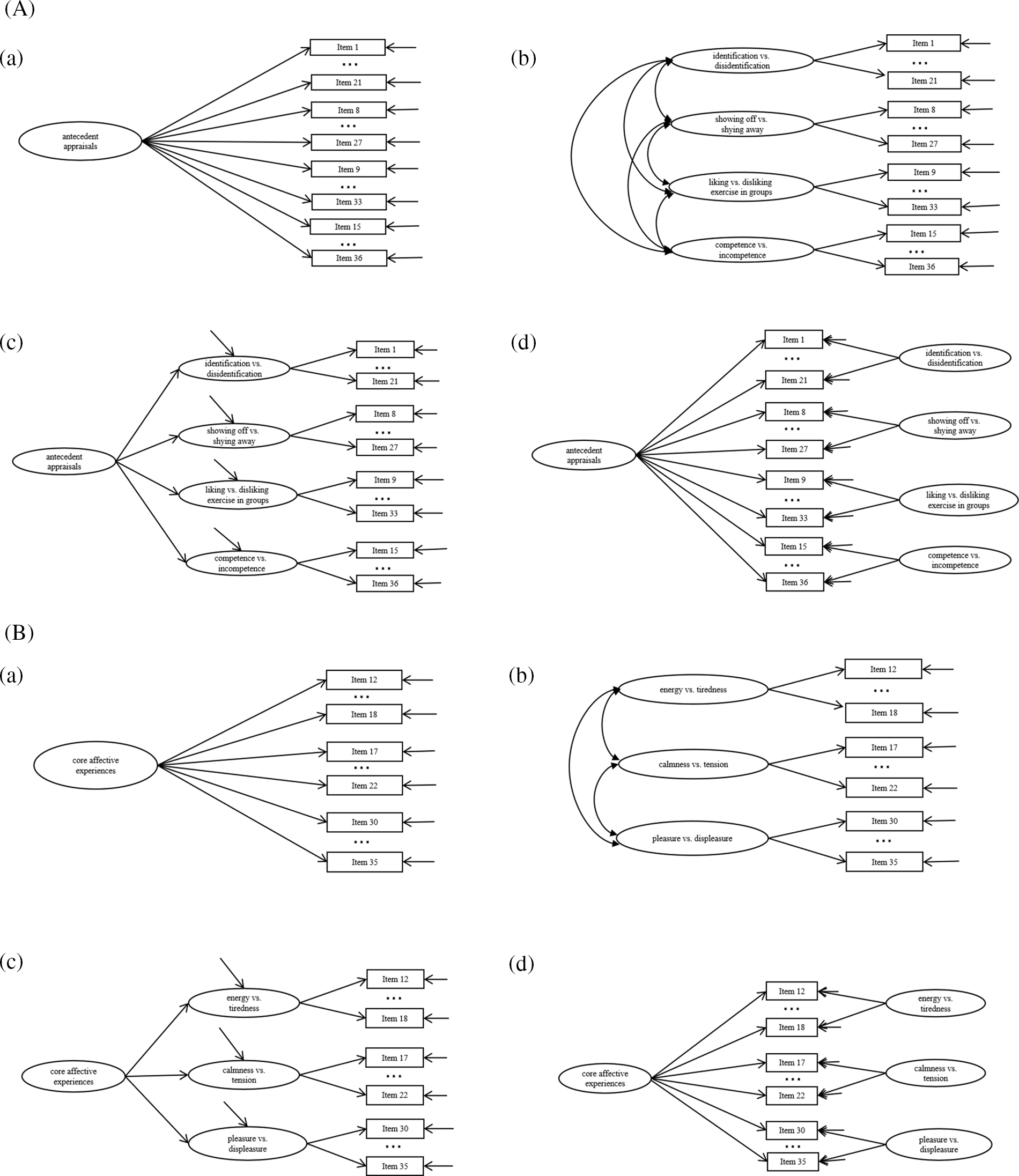
Figure 3: (A) Schematic representation of the four alternative models for antecedent appraisals. (B) Schematic representation of the four alternative models for core affective exercise experiences.
Note: For clarity, only first and final items are shown for each factor, with remaining items represented by ellipses. a. One-factor model. b. First-order model. c. Second-order model. d. Bifactor model.
The goodness of model fit was assessed by the following parameters: the Tucker-Lewis Index (TLI), Comparative Fit Index (CFI), Standardized Root Mean Square Residual (SRMR), and Root Mean Square Error of Approximation (RMSEA), with a 90% Confidence Interval (CI). According to the common criteria [39], adequate model fit is suggested by the following values for these indices: CFI and TLI close to 0.95 (ideally ≥ 0.95); SRMR and RMSEA close to 0.06 (ideally ≤ 0.06). The following statistical indices were tested to further evaluate the bifactor model [40,41]: the Omega (ω)/Omega S (ωS), Omega Hierarchical (ωH)/Omega HS (ωHS), and Explained Common Variance (ECV). Specifically, ω estimates the internal reliability of the multidimensional composite, while ωS for specific factors are only relevant to items loading on that factor. The general factor reliability statistic ωH reflects the amount of total variance attributed to variance on the general factor, whereas ωHS refers to the proportion of total variance attributable to specific factors after removing the variance explained by the general factor. These values range from 0 to 1, and >0.80 are high, with preferred values >0.90 [42,43]. Explained common variance (ECV) is calculated by dividing the variance explained by the general factor by the variance explained by both general and specific factors. Unidimensionality of a measure is suggested by ECV values >0.85 [44]. Based on the preceding analyses, correlation analyses between the three constructs and the levels of PA were examined. We rated the magnitude of the correlations by the following criteria: weak or small correlation: r = 0.10 to 0.29; moderate correlation: r = 0.30 to 0.49; high or large correlation: r ≥ 0.50 [45].
Additionally, a mediation model between the three AFFEXX-C constructs and MVPA level was carried out via PROCESS [46] in Study 2. Based on the existing framework [25,26], we regarded core affective experiences and attraction-antipathy as mediators between antecedent appraisals and MVPA level. These mediation hypotheses were tested following the method proposed by Hayes for the mediated analysis [47,48]. Specifically, there are four paths to the dependent variable (including one direct path and three indirect paths), and the standardized regression weights were respectively represented by path coefficients (i.e., letters a1, a2, d21, b1, b2, c, and c′). The mediating effect exists if the CIs of the path parameter do not include zero. As is standard practice, we set p < 0.05 as the statistical significance level in this study.
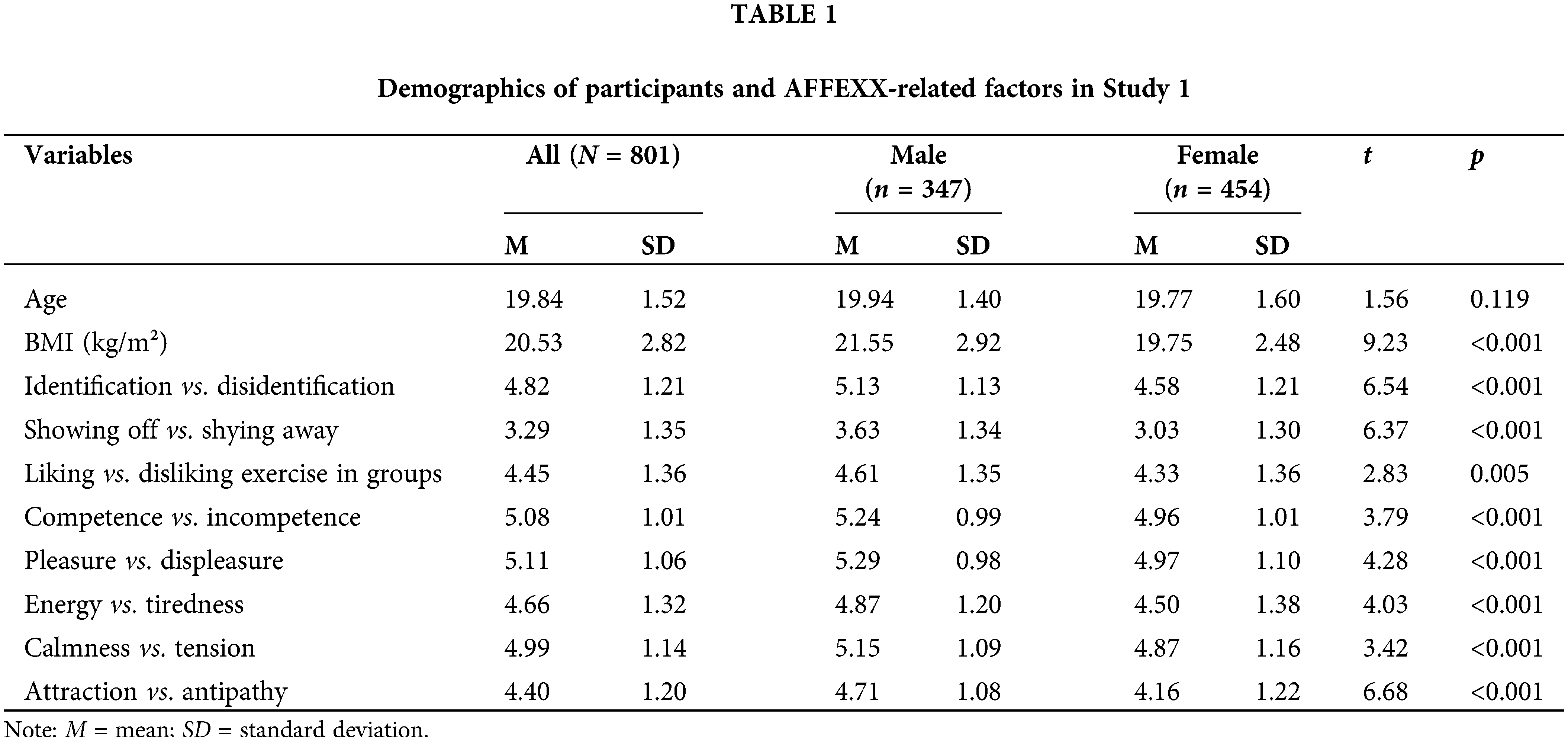
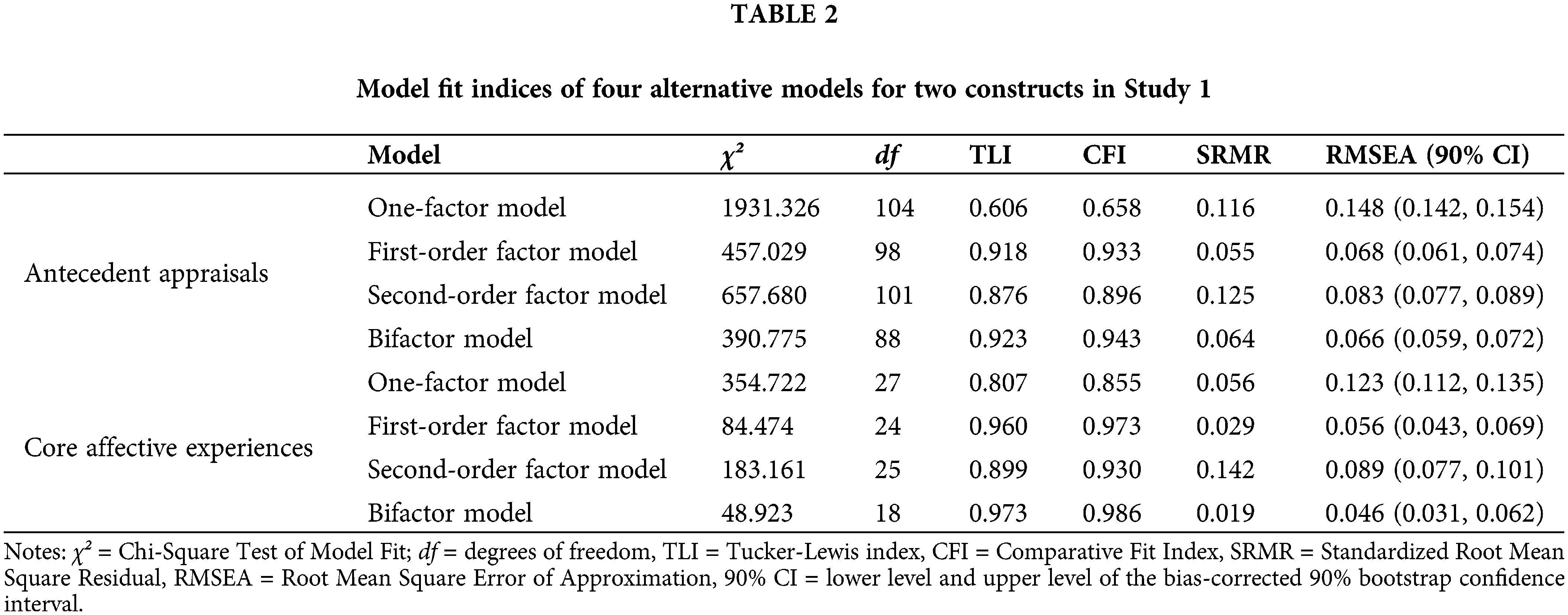
Sample demographics as well as gender differences in the factors of the AFFEXX-C, are shown in Table 1. Men reported higher scores on all factors of the AFFEXX-C, compared with women. Goodness-of-Fit statistics for the four tested models of each construct are presented in Table 2, respectively. For these two constructs, including antecedent appraisals and core affective exercise experiences, the first-order model and bifactor model provided adequate fit, in which a less stringent cut-off of 0.90 for the CFI and TLI was used [49]. The bifactor model had the best model-fit among respective four alternative models (antecedent appraisals: χ² (88) = 390.78, TLI = 0.92, CFI = 0.94, SRMR = 0.06, RMSEA = 0.07 [0.06, 0.07]; core affective experiences: χ² (18) = 48.92, TLI = 0.97, CFI = 0.99, SRMR = 0.02, RMSEA = 0.05 [0.03, 0.06]).
The reliability of the bifactor models is presented in Table 3. Results illustrated strong reliability for two general factors (ω = 0.95 for both antecedent appraisals and core affective experiences) and their specific sub-factors (ωS ranging from 0.85 to 0.91). For antecedent appraisals, reliability of two construct-specific factors identification-disidentification and competence-incompetence (ωHS = 0.00 and 0.27, respectively) was considerably lower than that for the other two specific factors (ωHS = 0.59 and 0.66, respectively). While the internal reliability of the three sub-factors for core affective exercise experiences were poor (ωHS ranging from 0.08 to 0.27), with extremely low reliable score variance explained by the construct-specific factors after controlling for the general factor. The ECV values for two general factors ranged from 0.61 to 0.79, with the values ranging from 0.03 to 0.15 for their specific factors. Standardized factor loadings and residual error of each item and their standard error for antecedent appraisals and core affective exercise experiences from bifactor models are shown in Figs. 4 and 5, respectively. Item loadings on core affective experiences were higher than the three specific factors, whereas lower item loadings on antecedent appraisals compared to the two sub-factors of the four were captured (except identification-disidentification and competence-incompetence).
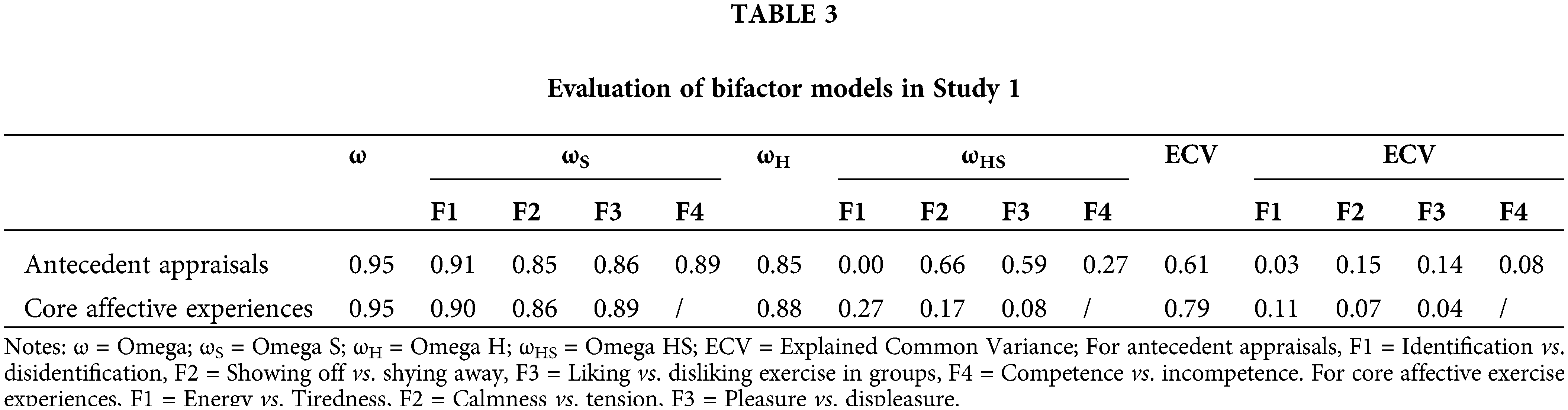
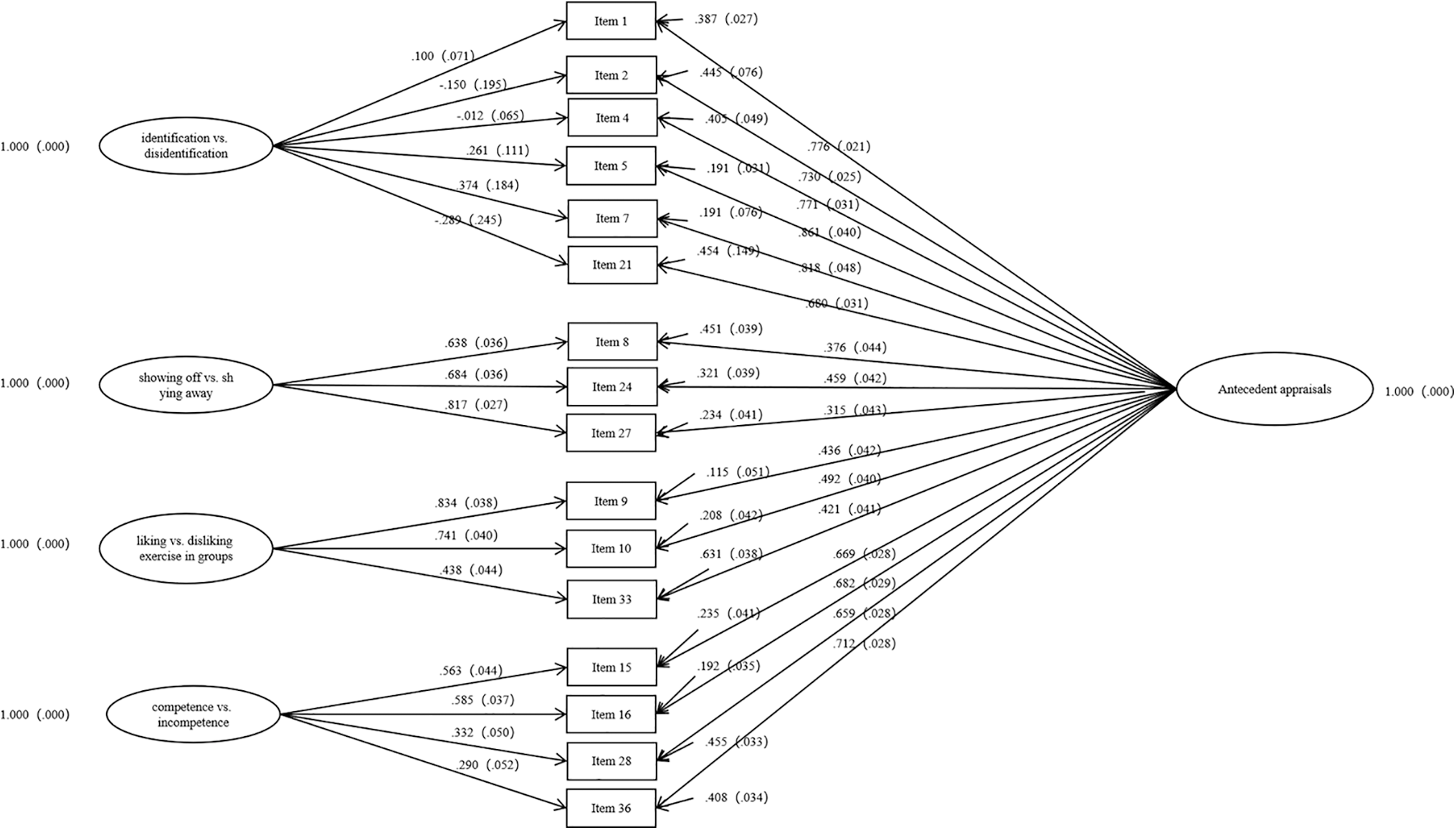
Figure 4: Factor loadings for bifactor model of antecedent appraisals.
Note: Standardized factor loadings and standard errors for each item onto the general factor and the specific sub-factors are shown. Small arrows represent residual error.
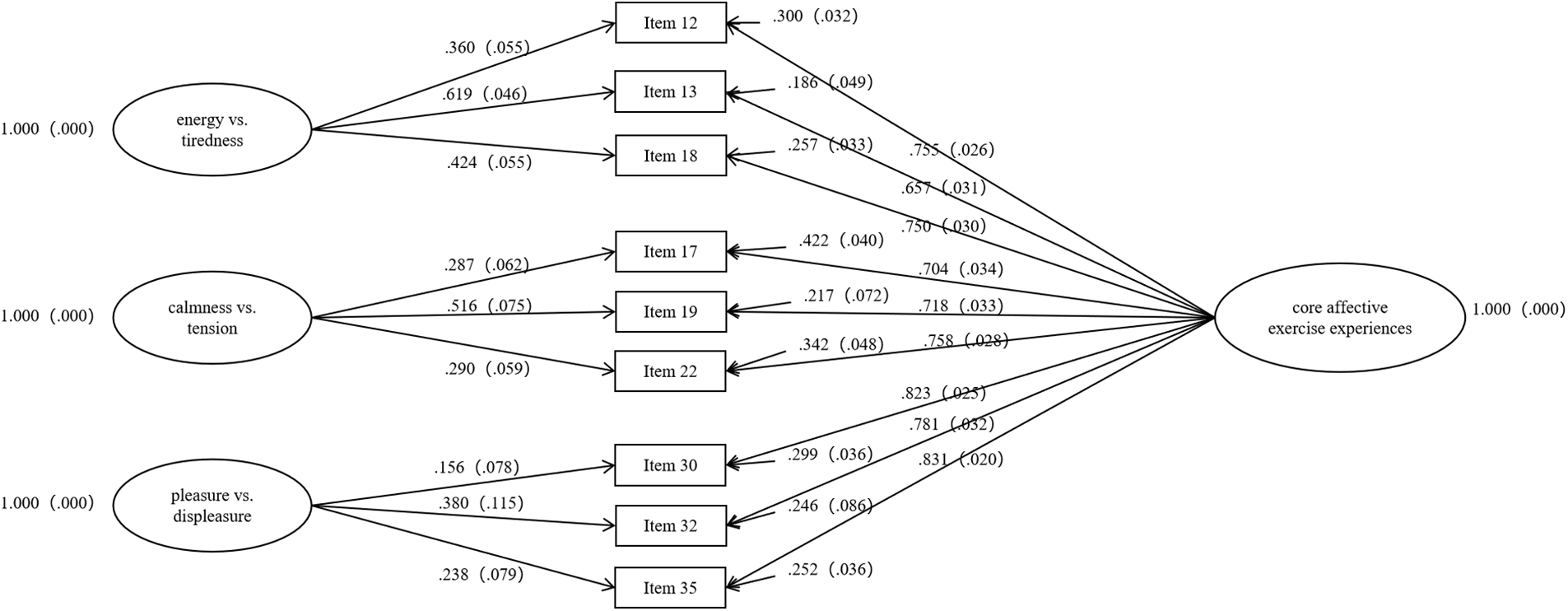
Figure 5: Factor loadings for bifactor model of core affective exercise experiences.
Note: Standardized factor loadings and standard errors for each item onto the general factor and the specific sub-factors are shown. Small arrows represent residual error.
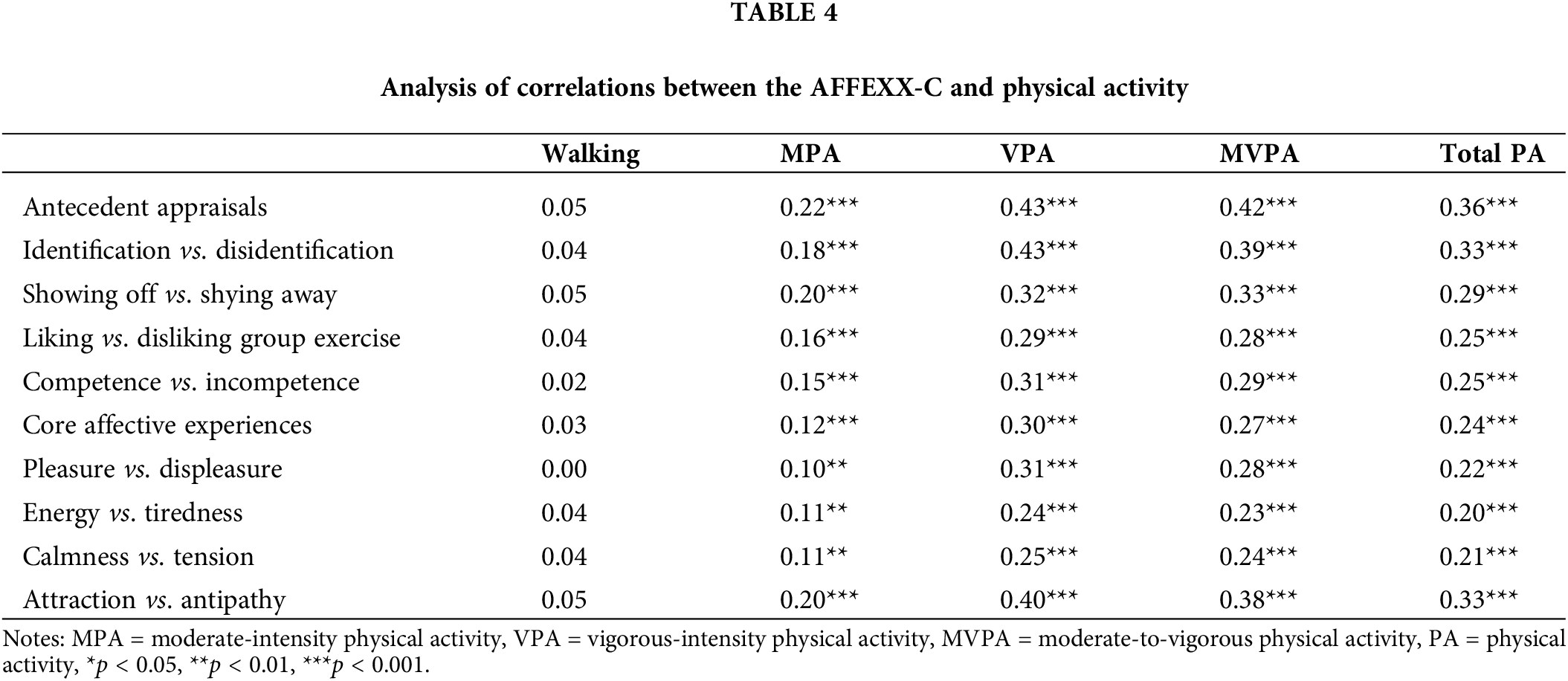
Correlation analyses between the total scores of these three constructs and the self-reported level of habitual PA are displayed in Table 4. All constructs (r = 0.12 to 0.43) and lower-order factors of the AFFEXX-C were significantly correlated with PA level (p < 0.01) in Pearson correlation analyses, except walking.
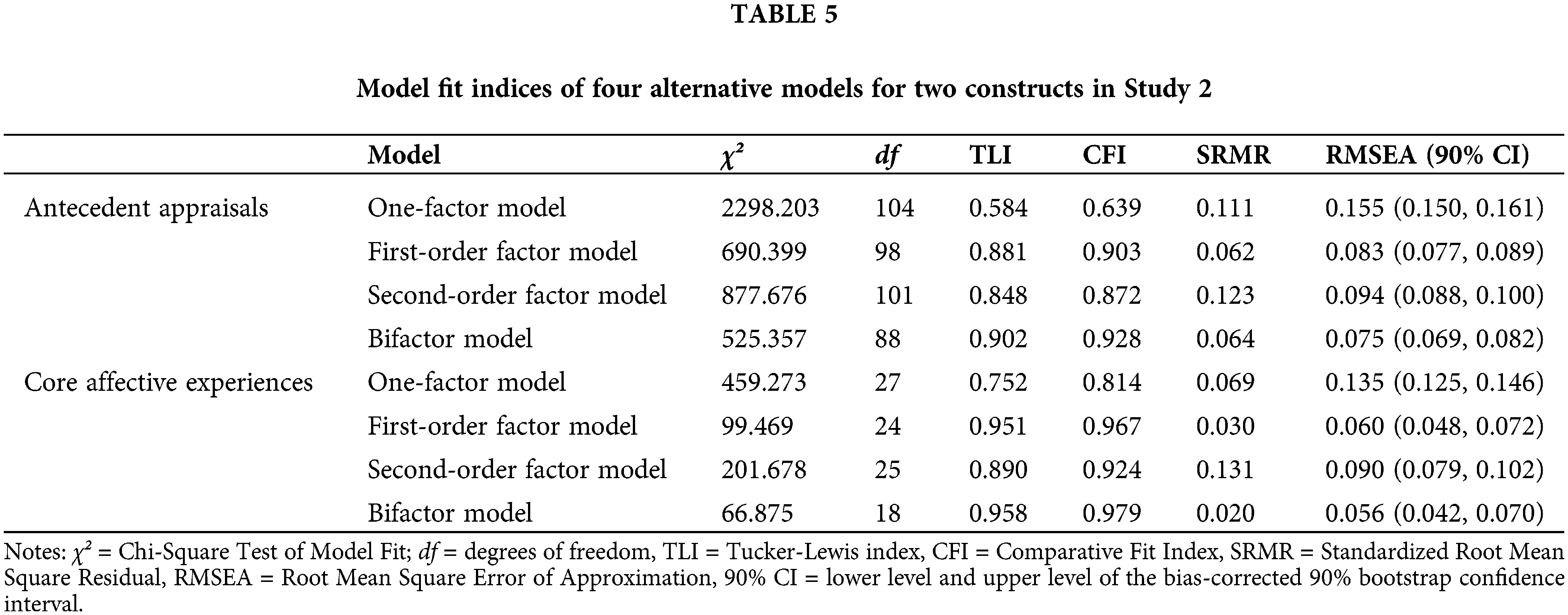
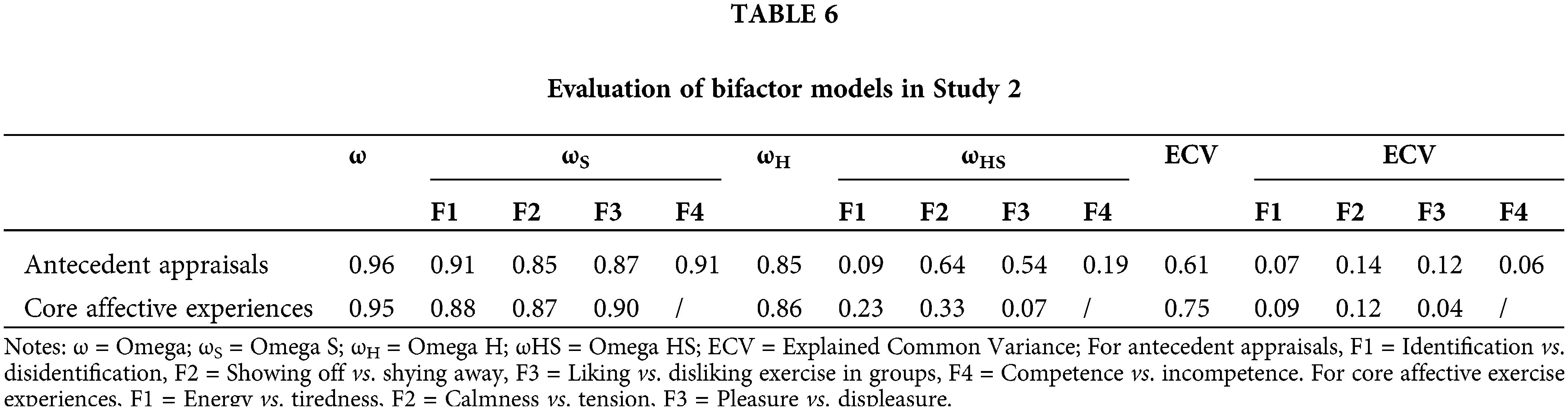
In Study 2, a sample of 875 participants (477 female, 398 male, age = 19.23 ± 1.94 years, Body Mass Index = 20.63 ± 2.77 kg/m2) was included in our statistical analyses. Model fit statistics for the four alternative models of each construct are presented in Table 5. Results indicated that bifactor models of these two general factors (i.e., antecedent appraisals and core affective exercise experiences) were adequate fits for the data and superior to the other models, concurring with the above Study 1. Model-based reliability is displayed in Table 6. Strong reliability was illustrated for the two constructs (ω = 0.96 and 0.95, respectively) and their specific sub-factors (ωS ranging from 0.85 to 0.91). Specifically, the internal reliability of identification-disidentification for antecedent appraisals (ωHS = 0.09) and pleasure-displeasure for core affective experiences (ωHS = 0.07) were considerably lower compared to the other corresponding specific factors. The ECV values of 0.61 and 0.75 for two general factors were close to the results of Study 1, with the values ranging from 0.04 to 0.14 for their sub-factors. Standardized factor loadings and residual error of each item and their standard error for antecedent appraisals and core affective exercise experiences from bifactor models in Study 2 were also tested (shown in Figs. S1 and S2 in supplementary materials).
Similar to Study 1, correlation analysis in Study 2 also showed that the constructs and related lower-order factors of the AFFEXX-C were significantly correlated to PA level, except walking (presented in Table 7). Specifically, the total scores of these three constructs were positively correlated to the level of VPA (r = 0.36, 0.28, and 0.38), MVPA (r = 0.32, 0.26, and 0.34), and total PA (r = 0.25, 0.23, and 0.28), respectively. As displayed in Table 8 and Fig. 6, the results of mediation analyses indicated that the 95% CI for the total, direct and indirect effects did not include zero, which means that the indirect and direct effects of antecedent appraisals on MVPA were statistically significant based on the regression analysis. Three indirect effects paths were as followed: antecedent appraisals → core affective experiences → MVPA; antecedent appraisals → attraction-antipathy → MVPA; antecedent appraisals → core affective experiences → attraction-antipathy → MVPA. The examination of the indirect effects showed that core affective exercise experiences and attraction-antipathy are mediators of the relationship between antecedent appraisals and MVPA.
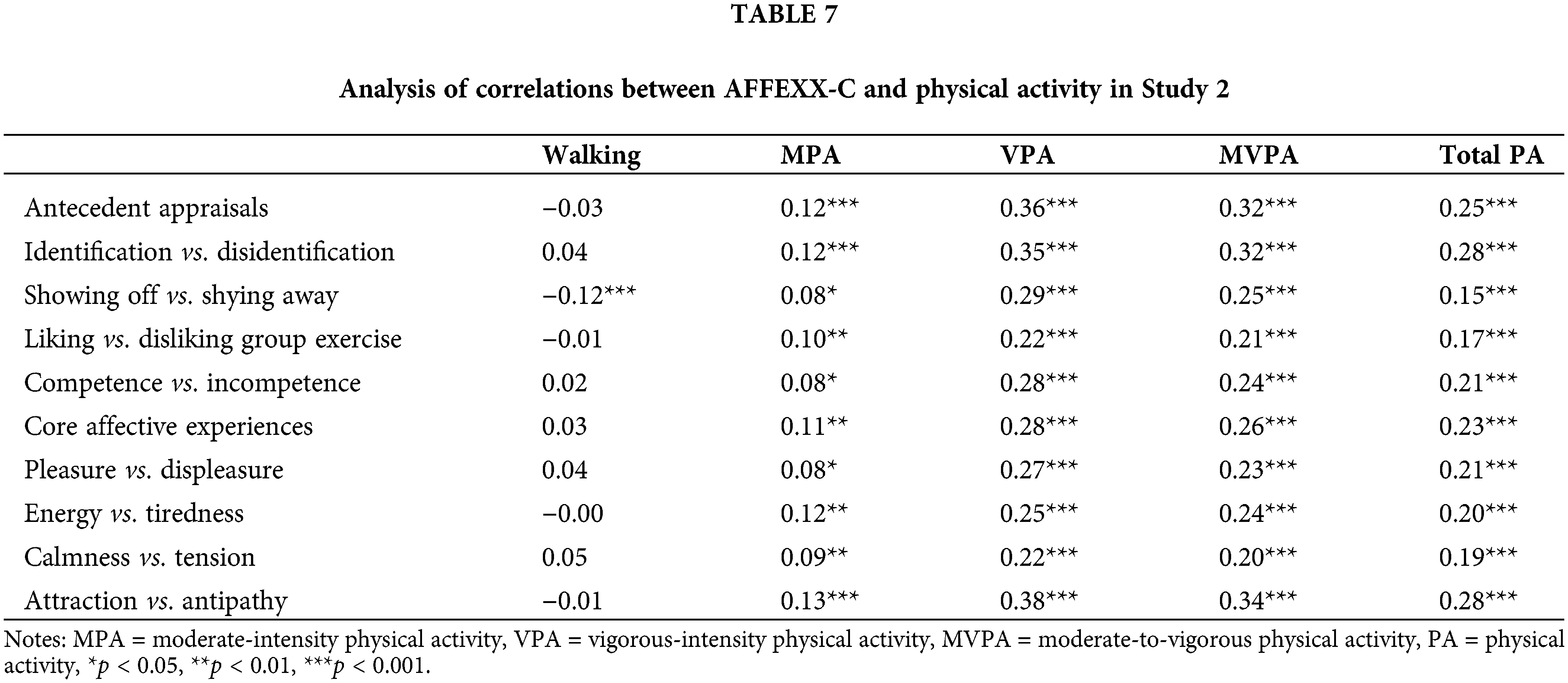
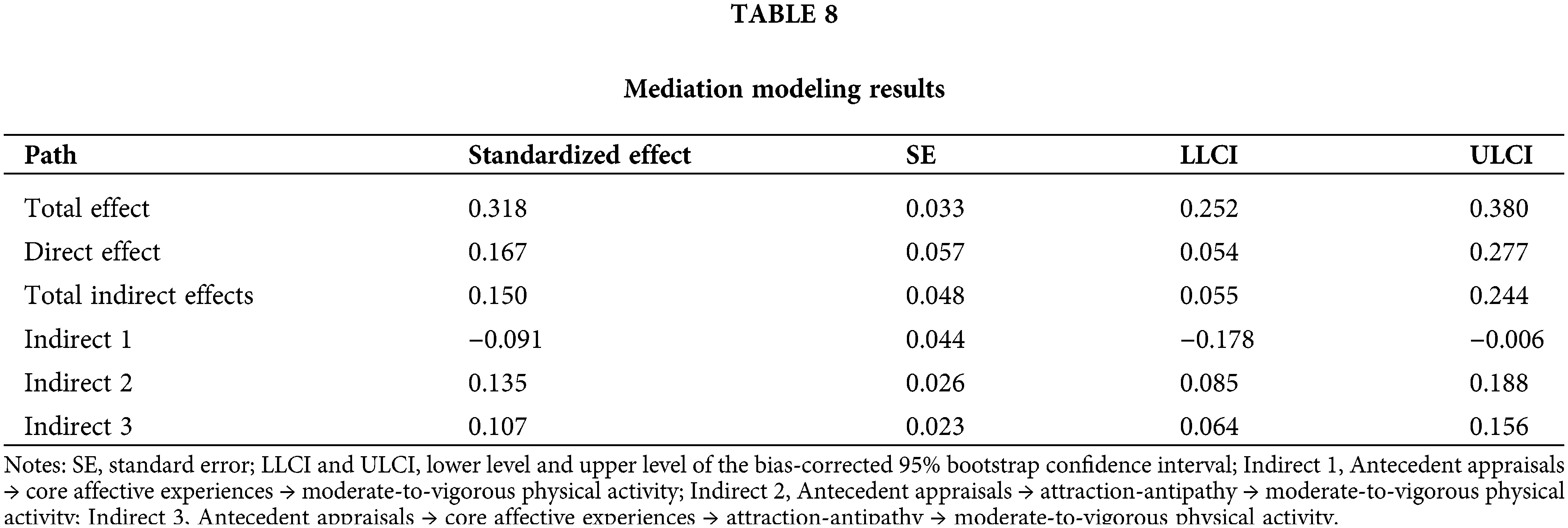
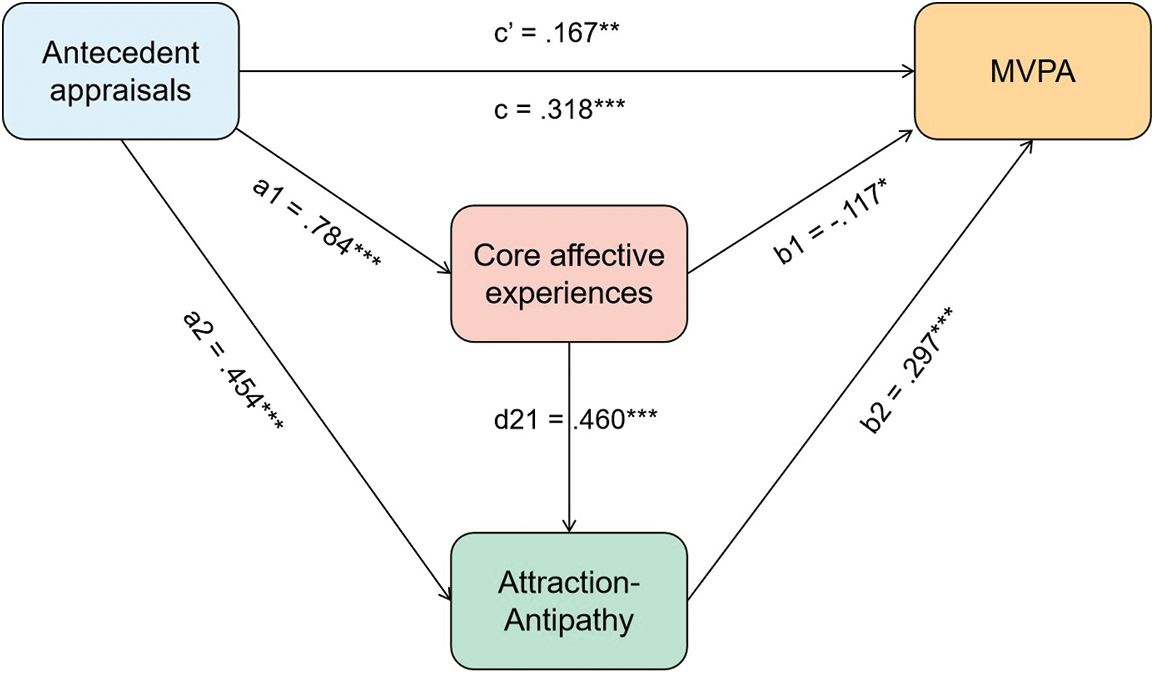
Figure 6: Statistical diagram of the multiple mediation model
Notes: MVPA = moderate-to-vigorous physical activity; Estimate values of each path are respectively presented by standardized path coefficients: a1, a2, d21, b1, b2, c, and c′; Of them, c′ stands for the direct path effect size from antecedent appraisals to moderate-to-vigorous physical activity, c stands for the total effect size between them. p < 0.05; p < 0.01; p < 0.001.
The main aims of the current study were to (a) determine whether higher-order construct scores and lower-order factor scores can be used independently via the bifactor analysis approach and (b) corroborate the positive association between the three constructs and PA level among Chinese college students. The results of our model comparison and bifactor analyses supported the use of higher-order construct scores of the AFFEXX-C in Chinese college students, as these findings suggested that the multidimensionality of the AFFEXX-C is not sufficient to negate the utilization of a total construct score (i.e., a strong general factor) [50]. In addition, our results indicated that all three constructs were positively correlated to MVPA level in our two studies. Moreover, core affective experiences and attraction-antipathy mediated the relationship between antecedent appraisals and MVPA levels.
Results of model comparison and the adequate model fit of bifactor models in two studies supported not only the scale multidimensionality but the presence of the general factors. Specifically, the good psychometric properties in bifactor analysis statistically confirmed our initial assumption about utilizing the total scores of the three constructs. As a challenging statistical method, bifactor model analysis allows for the commonality among the items explained by the general factor to be partitioned out, with the specific factors representing only the unique shared variance among the items on each factor. Due to its role in improving the scale’s usefulness as a benchmarking tool and the comprehensibility of participants’ feedback by measuring a similar super-ordinate construct, the bifactor analysis approach has been frequently applied in other studies [51,52]. Additionally, using the overall scores of affective exercise experiences can provide some benefits. For example, affective exercise experiences may contain not only an individual’s affective valence on various aspects of physical exercise but may also include information about the overall affective exercise experiences. This potential information is not exploited in the model of the original AFFEXX questionnaire. Moreover, single-factor scores may be easier to interpret if scores on factors of affective exercise experiences or antecedent appraisals can be correlated with their overall constructs’ scores. Lastly, using a structural score in a research or clinical setting makes it easier to provide feedback to the participant/patient given the fact that reporting and explaining up to seven separate factors’ scores to them is more difficult. Thus, the bifactor analysis approach is a valuable tool for deriving the overall score and the application of constructs’ scores increased the value of the information obtained from the participants without impacting the factors’ scores. Our validation of the use of structural scores has made the AFFEX-C scale more accessible, which might improve the degree to which the AFFEXX-C is utilized in the future.
In general, it is widely accepted that more pronounced positive affective exercise experiences are positively linked to future PA behavior [17], which is supported by the results of correlation analysis in this study (mainly presented in Tables 4 and 7) showing that individuals with greater core affective experiences reported higher PA levels. Furthermore, our finding is comparable to the observations of previous studies that reported positive correlations between the factors of core affective exercise experiences and the self-reported PA level [25,26]. A potential explanation for this phenomenon is that positive affect (including positive affective exercise experiences) plays a critical role in decision-making towards exercise by supporting ongoing exercise behavior [53]. Actually, engaging in physical exercise regularly requires not only the individual’s motivation to start actions (e.g., make exercise plans and do exercise) but also the individual’s ability to maintain exercise adherence. From this point of view, affective exercise experiences may have a greater impact on exercise adherence. For instance, a review suggested that enjoyment and the absence of unpleasant experiences is one of the key factors identified as relevant to increase adherence to physical exercise [54]. Thus, if negative emotions are elicited by negative affective exercise experiences (e.g., during physical exercise), this may play a part in contributing to the cessation of the physical exercise, and the lack of future motivation to engage in physical exercises, which, in turn, might necessitate a greater motivation demand for future participation in physical exercises [16].
Another important finding of the current study is that we identified a specific mechanism explaining the effect of AFFEXX-C on PA levels. In particular, as forecasted in our hypothesis, core affective exercise experiences and attraction-antipathy mediate the relationship between antecedent appraisals and MVPA level. Of note, the negative parameter of indirect effect path 1 (Antecedent appraisals → core affective experiences → MVPA) indicated a small direct mediation effect of core affective experiences. According to the observed positive relationship among these variables, we suggested that the negative path coefficient may be caused by co-linearity [55,56]. Another potential explanation is that the indirect effect offsets a part of the direct effect of the antecedent appraisals on the MVPA level, which can be interpreted as a kind of suppressing effect [57–60]. That said, core affective exercise experiences partially conceal the influence of antecedent appraisals on MVPA level, and this impact can be boosted by controlling the affective exercise experiences. Additionally, the findings also revealed that the effect size of the indirect effect path 3 was relatively larger among the three indirect effect paths and direct effect paths. The latter indicated that individuals’ exercise behavior may depend more on attraction-antipathy towards exercise, which is strongly influenced by antecedent appraisals and core affective exercise experiences.
A strength of the current study is that our findings provide novel insights into the scoring of the AFFEXX-C and the psychological mechanisms that potentially mediate the relationship between affective exercise experience and the level of regular PA. Several potential limitations should be recognized when interpreting the findings of the current study. Firstly, self-reports, as used in the current study, are prone to different sources of bias (e.g., social desirability bias). Hence, future studies should aim to verify (or refute) our findings by incorporating objective measures (e.g., assessing physical activity with accelerometers). Secondly, as our study focused on healthy college students, the generalizability of our findings is somewhat limited. Thus, further studies in other populations (e.g., people with mental disorders and older adults) are necessary to investigate whether our findings are generalizable to these cohorts.
In summary, the current study provides evidence that among our sample of Chinese college students, the overall scores of the three constructs of the AFFEXX-C are useful indicators, as demonstrated by the results of the bifactor analyses. Additionally, the findings of this study revealed that core affective exercise experiences and attraction-antipathy mediate the relationship between antecedent appraisals and MVPA level. These findings support the assumption that measuring affective exercise experiences in future research is important to gain a more nuanced understanding of the psychological mechanisms driving exercise behavior.
Funding Statement: This study was supported by the Start-Up Research Grant of Shenzhen University [20200807163056003]; the Start-Up Research Grant [Peacock Plan: 20191105534C].
Author Contributions: The authors confirm their contribution to the paper as follows: Ting Wang, Conceptualization, Methodology, Data Curation, Formal Analysis, Writing—Original Draft, Writing—Review & Editing, Visualization; Markus Gerber, Writing—Review & Editing, Formal Analysis; Fabian Herold, Write—Review & Editing; Joseph Bardeen, Methodology, Writing—Original Draft, Writing—Review & Editing, Visualization; Sebastian Ludyga, Formal Analysis; Alyx Taylor, Methodology, Formal Analysis; Arthur F. Kramer, Writing—Review & Editing, Formal Analysis; Liye Zou, Conceptualization, Methodology, Data Curation, Formal Analysis, Writing—Original Draft, Writing—Review & Editing, Visualization, Supervision, Project Administration, Funding Acquisition. All authors reviewed the results and approved the final version of the manuscript.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. World Health Organization. Global recommendations on physical activity for health [Internet]. 2010. [Google Scholar]
2. Chen LJ, Hamer M, Lai YJ, Huang BH, Ku PW, Stamatakis E. Can physical activity eliminate the mortality risk associated with poor sleep? A 15-year follow-up of 341,248 MJ Cohort participants. J Sport Health Sci [Internet]. 2022;11(5):596–604. doi:https://doi.org/10.1016/j.jshs.2021.03.001. [Google Scholar] [PubMed] [CrossRef]
3. Van de Zande SC, de Vries JK, Van den Akker-Scheek I, Zwerver J, Smit AJ. A physically active lifestyle is related to a lower level of skin autofluorescence in a large population with chronic-disease (LifeLines cohort). J Sport Health Sci [Internet]. 2022;11(2):260–5. doi:https://doi.org/10.1016/j.jshs.2020.09.007. [Google Scholar] [PubMed] [CrossRef]
4. Budde H, Schwarz R, Velasques B, Ribeiro P, Holzweg M, Machado S, et al. The need for differentiating between exercise, physical activity, and training. Autoimmun Rev [Internet]. 2016;15(1):110–1. doi:https://doi.org/10.1016/j.autrev.2015.09.004. [Google Scholar] [PubMed] [CrossRef]
5. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep [Internet]. 1985;100(2):126–31. [Google Scholar] [PubMed]
6. Van Baak MA, Pramono A, Battista F, Beaulieu K, Blundell JE, Busetto L, et al. Effect of different types of regular exercise on physical fitness in adults with overweight or obesity: systematic review and meta-analyses. Obes Rev [Internet]. 2021;22 Suppl 4(Suppl 4):e13239. [Google Scholar] [PubMed]
7. Wu PF, Lu H, Zhou X, Liang X, Li R, Zhang W, et al. Assessment of causal effects of physical activity on neurodegenerative diseases: a mendelian randomization study. J Sport Health Sci [Internet]. 2021;10(4):454–61. doi:https://doi.org/10.1016/j.jshs.2021.01.008. [Google Scholar] [PubMed] [CrossRef]
8. Huang Y, Jiang C, Xu L, Zhang W, Zhu F, Jin Y, et al. Mortality in relation to changes in physical activity in middle-aged to older Chinese: an 8-year follow-up of the Guangzhou Biobank Cohort Study. J Sport Health Sci [Internet]. 2021;10(4):430–8. doi:https://doi.org/10.1016/j.jshs.2020.08.007. [Google Scholar] [PubMed] [CrossRef]
9. Xie F, You Y, Huang J, Guan C, Chen Z, Fang M, et al. Association between physical activity and digestive-system cancer: an updated systematic review and meta-analysis. J Sport Health Sci [Internet]. 2021;10(1):4–13. doi:https://doi.org/10.1016/j.jshs.2020.09.009. [Google Scholar] [PubMed] [CrossRef]
10. Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. The Lancet [Internet]. 2017;390(10113):2643–54. doi:https://doi.org/10.1016/S0140-6736(17)31634-3. [Google Scholar] [PubMed] [CrossRef]
11. Mok A, Khaw KT, Luben R, Wareham N, Brage S. Physical activity trajectories and mortality: population based cohort study. BMJ [Internet]. 2019;365:l2323. doi:https://doi.org/10.1136/bmj.l2323. [Google Scholar] [PubMed] [CrossRef]
12. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet [Internet]. 2012;380(9838):247–57. doi:https://doi.org/10.1016/S0140-6736(12)60646-1. [Google Scholar] [PubMed] [CrossRef]
13. Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Health behavior and health education: theory, research, and practice [Internet]. 4th ed. San Francisco, CA, US: Jossey-Bass; 2008. p. 465–85. [Google Scholar]
14. Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Med Sci Sports Exerc [Internet]. 2002;34(12):1996–2001. doi:https://doi.org/10.1097/00005768-200212000-00020. [Google Scholar] [PubMed] [CrossRef]
15. Stevens CJ, Baldwin AS, Bryan AD, Conner M, Rhodes RE, Williams DM. Affective determinants of physical activity: a conceptual framework and narrative review. Front Psychol [Internet]. 2020;11:495. doi:https://doi.org/10.3389/fpsyg.2020.568331. [Google Scholar] [PubMed] [CrossRef]
16. Brand R, Ekkekakis P. Affective-reflective theory of physical inactivity and exercise. Ger J Exerc Sport Res [Internet]. 2018;48(1):48–58. doi:https://doi.org/10.1007/s12662-017-0477-9. [Google Scholar] [CrossRef]
17. Rhodes RE, Kates A. Can the affective response to exercise predict future motives and physical activity behavior? A systematic review of published evidence. Ann Behav Med [Internet]. 2015;49(5):715–31. doi:https://doi.org/10.1007/s12160-015-9704-5. [Google Scholar] [PubMed] [CrossRef]
18. Ekkekakis P, Hall EE, Petruzzello SJ. Practical markers of the transition from aerobic to anaerobic metabolism during exercise: rationale and a case for affect-based exercise prescription. Prev Med [Internet]. 2004;38(2):149–59. doi:https://doi.org/10.1016/j.ypmed.2003.09.038. [Google Scholar] [PubMed] [CrossRef]
19. Williams DM. Exercise, affect, and adherence: an integrated model and a case for self-paced exercise. J Sport Exerc Psychol [Internet]. 2008;30(5):471–96. doi:https://doi.org/10.1123/jsep.30.5.471. [Google Scholar] [PubMed] [CrossRef]
20. Puetz TW. Physical activity and feelings of energy and fatigue: epidemiological evidence. Sports Med [Internet]. 2006;36(9):767–80. doi:https://doi.org/10.2165/00007256-200636090-00004. [Google Scholar] [PubMed] [CrossRef]
21. Carfora V, Biella M, Catellani P. Affective components in promoting physical activity: a randomized controlled trial of message framing. Front Psychol [Internet]. 2022;13:968109. doi:https://doi.org/10.3389/fpsyg.2022.968109. [Google Scholar] [PubMed] [CrossRef]
22. Dukes D, Abrams K, Adolphs R, Ahmed ME, Beatty A, Berridge KC, et al. The rise of affectivism. Nat Hum Behav [Internet]. 2021;5(7):816–20. doi:https://doi.org/10.1038/s41562-021-01130-8. [Google Scholar] [PubMed] [CrossRef]
23. Hardy CJ, Rejeski WJ. Not what, but how one feels: the measurement of affect during exercise. J Sport Exerc Psycho [Internet]. 1989;11(3):304–17. doi:https://doi.org/10.1123/jsep.11.3.304. [Google Scholar] [CrossRef]
24. Kendzierski D, DeCarlo KJ. Physical activity enjoyment scale: two validation studies. J Sport Exerc Psycho [Internet]. 1991;13(1):50–64. doi:https://doi.org/10.1123/jsep.13.1.50. [Google Scholar] [CrossRef]
25. Ekkekakis P, Zenko Z, Vazou S. Do you find exercise pleasant or unpleasant? The Affective Exercise Experiences (AFFEXX) questionnaire. Psychol Sport Exerc [Internet]. 2021;55(10):101930. doi:https://doi.org/10.1016/j.psychsport.2021.101930. [Google Scholar] [CrossRef]
26. Wang T, Cheval B, Maltagliati S, Zenko Z, Herold F, Ludyga S, et al. Validation of the Chinese Version of the Affective Exercise Experiences Questionnaire (AFFEXX-C). Int J Ment Health Pr [Internet]. 2023. [Google Scholar]
27. Bornovalova MA, Choate AM, Fatimah H, Petersen KJ, Wiernik BM. Appropriate use of bifactor analysis in psychopathology research: appreciating benefits and limitations. Biol Psychiatry [Internet]. 2020;88(1):18–27. doi:https://doi.org/10.1016/j.biopsych.2020.01.013. [Google Scholar] [PubMed] [CrossRef]
28. Gibbons R. Bi-factor analysis. In: Michalos AC, editor. Encyclopedia of quality of life and well-being research [Internet]. Dordrecht: Springer Netherlands; 2014, p. 386–94. [Google Scholar]
29. Rodriguez A, Reise SP, Haviland MG. Evaluating bifactor models: calculating and interpreting statistical indices. Psychol Methods [Internet]. 2016;21(2):137–50. doi:https://doi.org/10.1037/met0000045. [Google Scholar] [PubMed] [CrossRef]
30. Zhang B, Sun T, Cao M, Drasgow F. Using bifactor models to examine the predictive validity of hierarchical constructs: pros, cons, and solutions. Organ Res Methods [Internet]. 2021;24(3):530–71. doi:https://doi.org/10.1177/1094428120915522. [Google Scholar] [CrossRef]
31. Bardeen JR, Fergus TA. Multidimensional inventory of hypochondriacal traits: an examination of a bifactor model and measurement invariance between those with and without a self-reported medical condition. Assessment [Internet]. 2020;27(1):206–15. doi:https://doi.org/10.1177/1073191117725173. [Google Scholar] [PubMed] [CrossRef]
32. Reise SP. The rediscovery of bifactor measurement models. Multivar Behav Res [Internet]. 2012;47(5):667–96. doi:https://doi.org/10.1080/00273171.2012.715555. [Google Scholar] [PubMed] [CrossRef]
33. Fan M, Lyu J, He P. Chinese guidelines for data processing and analysis concerning the International Physical Activity Questionnaire. Zhonghua liu xing bing xue za zhi= Zhonghua liuxingbingxue zazhi [Internet]. 2014;35(8):961–4. [Google Scholar] [PubMed]
34. Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc [Internet]. 2003;35(8):1381–95. doi:https://doi.org/10.1249/01.MSS.0000078924.61453.FB. [Google Scholar] [PubMed] [CrossRef]
35. Macfarlane DJ, Lee CCY, Ho EYK, Chan KL, Chan DTS. Reliability and validity of the Chinese version of IPAQ (short, last 7 days). J Sci Med Sports [Internet]. 2007;10(1):45–51. doi:https://doi.org/10.1016/j.jsams.2006.05.003. [Google Scholar] [PubMed] [CrossRef]
36. Sjostrom M, Ainsworth BE, Bauman A, Bull FC, Hamilton-Craig CR, Sallis JF. Guidelines for data processing analysis of the International Physical Activity Questionnaire (IPAQ)—short and long forms. 2005. [Google Scholar]
37. Muthén LK, Muthén BO. Mplus version 8 user’s guide: Muthen & Muthen. 2017. [Google Scholar]
38. Brunner M, Nagy G, Wilhelm O. A tutorial on hierarchically structured constructs. J Pers [Internet]. 2012;80(4):796–846. doi:https://doi.org/10.1111/j.1467-6494.2011.00749.x. [Google Scholar] [PubMed] [CrossRef]
39. Hu Lt, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model [Internet]. 1999;6(1):1–55. doi:https://doi.org/10.1080/10705519909540118. [Google Scholar] [CrossRef]
40. Dueber DM. Bifactor Indices calculator: a microsoft excelbased tool to calculate various indices relevant to bifactor CFA model [Internet]. 2016. [Google Scholar]
41. Rodriguez A, Reise SP, Haviland MG. Applying bifactor statistical indices in the evaluation of psychological measures. J Pers Assess [Internet]. 2016;98(3):223–37. doi:https://doi.org/10.1080/00223891.2015.1089249. [Google Scholar] [PubMed] [CrossRef]
42. Gorsuch RL. Factor analysis [Internet]. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum; 1983. [Google Scholar]
43. Reise SP, Bonifay WE, Haviland MG. Scoring and modeling psychological measures in the presence of multidimensionality. J Pers Assess [Internet]. 2013;95(2):129–40. doi:https://doi.org/10.1080/00223891.2012.725437. [Google Scholar] [PubMed] [CrossRef]
44. Stucky BD, Edelen MO. Using hierarchical IRT models to create unidimensional measures from multidimensional data. In: Handbook of item response theory modeling [Internet]. Routledge; 2014. [Google Scholar]
45. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed [Internet]. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. [Google Scholar]
46. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach [Internet]. The Guilford Press; 2013. [Google Scholar]
47. Hayes AF. Beyond Baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr [Internet]. 2009;76(4):408–20. doi:https://doi.org/10.1080/03637750903310360. [Google Scholar] [CrossRef]
48. Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther [Internet]. 2017;98:39–57. doi:https://doi.org/10.1016/j.brat.2016.11.001. [Google Scholar] [PubMed] [CrossRef]
49. Chen FF, Hayes A, Carver CS, Laurenceau J-P, Zhang Z. Modeling general and specific variance in multifaceted constructs: a comparison of the bifactor model to other approaches. J Pers [Internet]. 2012;80(1):219–51. doi:https://doi.org/10.1111/j.1467-6494.2011.00739.x. [Google Scholar] [PubMed] [CrossRef]
50. Rodriguez A, Reise SP, Haviland MG. Evaluating bifactor models: calculating and interpreting statistical indices. Psychol Methods [Internet]. 2016;21(2):137–50. doi:https://doi.org/10.1037/met0000045. [Google Scholar] [PubMed] [CrossRef]
51. Geerards D, van den Berg L, Pusic AL, Hoogbergen MM, Klassen AF, van der Hulst RRWJ, et al. Deriving an overall appearance domain score by applying bifactor IRT analysis to the BODY-Q appearance scales. Qual Life Res [Internet]. 2020;29(4):1065–72. doi:https://doi.org/10.1007/s11136-019-02366-8. [Google Scholar] [PubMed] [CrossRef]
52. Wirtz MA, Schulz A, Brähler E. Confirmatory and bi-factor analysis of the Short Form Health Survey 8 (SF-8) scale structure in a German general population sample. Health Qual Life Out [Internet]. 2021;19(1):73. doi:https://doi.org/10.1186/s12955-021-01699-8. [Google Scholar] [PubMed] [CrossRef]
53. Cameron DS, Bertenshaw EJ, Sheeran P. Positive affect and physical activity: testing effects on goal setting, activation, prioritisation, and attainment. Psychol Health [Internet]. 2018;33(2):258–74. doi:https://doi.org/10.1080/08870446.2017.1314477. [Google Scholar] [PubMed] [CrossRef]
54. Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, Del Coso J, Leyton-Román M, Luque-Casado A, et al. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: an umbrella review. Int J Env Res Pub He [Internet]. 2021;18(4):2023. doi:https://doi.org/10.3390/ijerph18042023. [Google Scholar] [PubMed] [CrossRef]
55. O’brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant [Internet]. 2007;41(5):673–90. doi:https://doi.org/10.1007/s11135-006-9018-6. [Google Scholar] [CrossRef]
56. Hair JF. Multivariate data analysis: an overview. In: Lovric M, editor. International encyclopedia of statistical science [Internet]. Berlin, Heidelberg: Springer; 2011. p. 904–7. [Google Scholar]
57. Wen Z, Ye B. Mediating effect analysis: methodology and model development. Adv Psychol Sci [Internet]. 2014;5:731–45. [Google Scholar]
58. MacKinnon DP, Krull JL, Lockwood CM. Equivalence of the mediation, confounding and suppression effect. Prev Sci [Internet]. 2000;1(4):173–81. doi:https://doi.org/10.1023/A:1026595011371. [Google Scholar] [PubMed] [CrossRef]
59. Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods [Internet]. 2002;7(4):422–45. doi:https://doi.org/10.1037/1082-989X.7.4.422. [Google Scholar] [CrossRef]
60. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods [Internet]. 2008;40(3):879–91. doi:https://doi.org/10.3758/BRM.40.3.879. [Google Scholar] [PubMed] [CrossRef]
Appendix
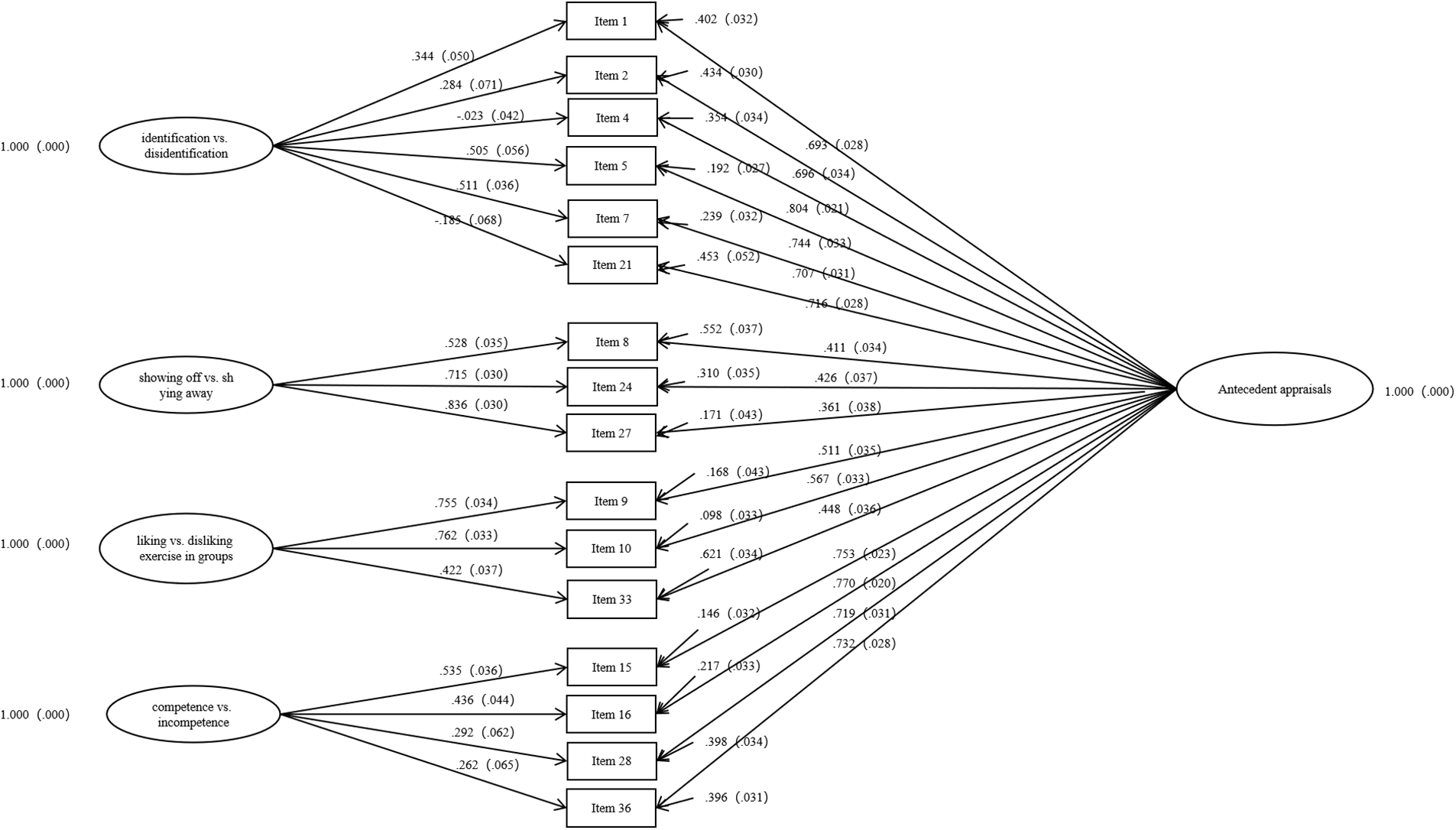
Figure S1: Illustration of factor loadings in bifactor analysis of antecedent appraisals in Study 2.
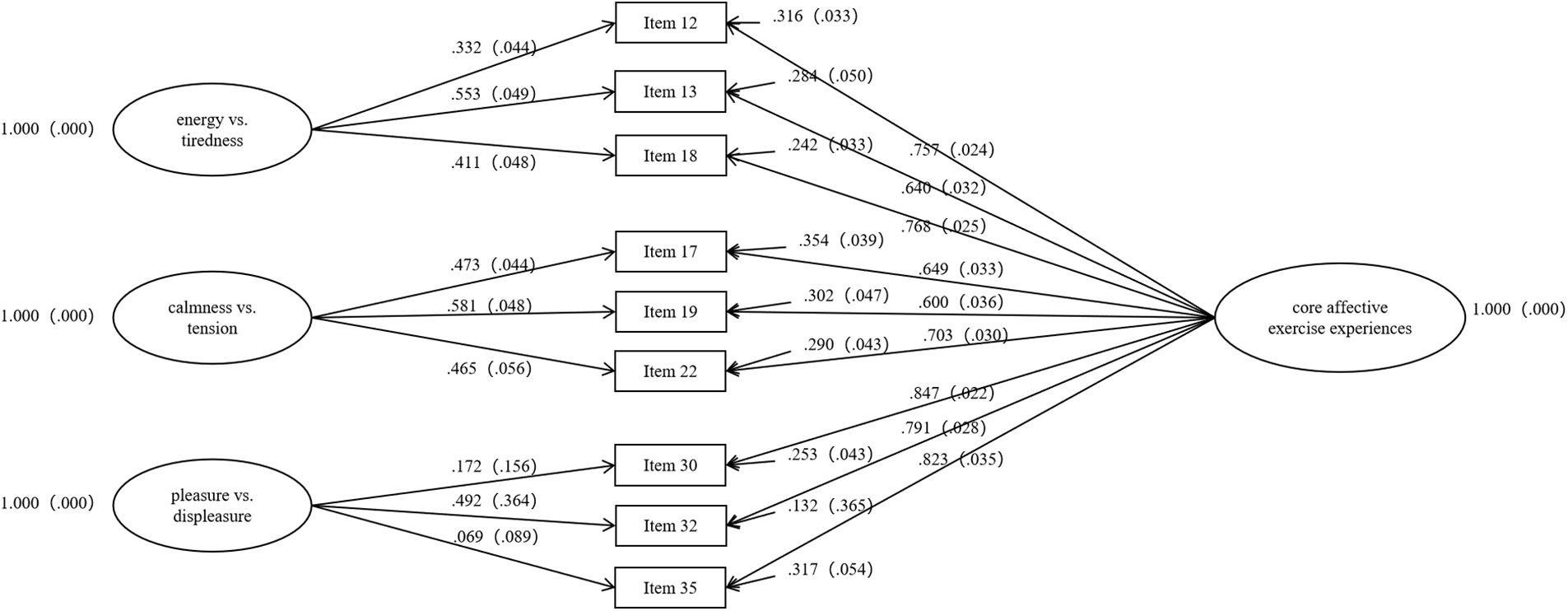
Figure S2: Illustration of factor loadings in bifactor analysis of core affective exercise experiences in Study 2.
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools