
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Associations between Mental Health Outcomes and Adverse Childhood Experiences and Character Strengths among University Students in Southern China
1 The First Dongguan Affiliated Hospital, Guangdong Medical University, Dongguan, 523710, China
2 Research Center for Quality of Life and Applied Psychology/Department of Psychology, Guangdong Medical University, Dongguan, 523808, China
3 Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, 90110, Thailand
4 Student Mental Health Education and Counseling Center, Guangdong Medical University, Dongguan, 523808, China
* Corresponding Authors: Wit Wichaidit. Email: ; Chonghua Wan. Email:
(This article belongs to the Special Issue: Social Stress, Adversity, and Mental Health in Transitional China)
International Journal of Mental Health Promotion 2023, 25(12), 1343-1351. https://doi.org/10.32604/ijmhp.2023.043446
Received 07 July 2023; Accepted 02 November 2023; Issue published 29 December 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Adverse childhood experiences (ACEs) can negatively affect mental health, whereas character strengths seem to be positively correlated with mental health. Detailed information on the history of ACEs among university students in China and the extent which mental health is associated with ACEs and character strengths can contribute to the needed empirical evidence for relevant stakeholders. Objectives of this study are 1) to estimate the prevalence of ACEs among undergraduate students in Southern China; and 2) to assess the extent which mental health outcomes (positive growth, well-being, and depression) are associated with ACEs and character strengths among undergraduate students in Southern China. We conducted a self-administered survey among first and second-year students at a university in Southern China and analyzed data using descriptive statistics and linear regression analyses. Among the 779 students who completed the questionnaire, 283 were males, 439 were females, and 57 did not indicate their gender. The prevalence of ACEs among the participants was 32.1%. History of ACEs was associated with lower positive growth score (Adjusted Beta = −0.20; 95% CI = −0.37, −0.02; p = 0.030) and lower well-being score (Adjusted Beta = −1.13; 95% CI = −2.04, −0.23; p = 0.014). Vitality domain of character strength was associated with all three mental health outcomes after adjusting for covariables (all p-values < 0.001). Our study findings provide empirical evidence for stakeholders in university mental health. However, caveats regarding lack of temporality, selection bias, social desirability bias, and lack of generalizability should be considered in the interpretation of the study findings.Keywords
Adverse childhood experiences (ACEs) refer to negative events that an individual experiences in childhood that cause harm or threat to their mental and physical health [1,2]. There are three categories of ACEs: abuses (physical, emotional, sexual), neglects (physical, emotional), and household dysfunctions (family history of mental illness, incarceration, substance abuse, divorce, or domestic violence) [3,4]. Adults with a history of ACEs tend to have more short-term and long-term health problems and higher premature deaths than those without such a history [5] through differences in physiological development and health-damaging behaviors [6]. History of ACEs is also associated with depression [7] among children [8], university students [9,10], as well as homosexual men [11].
However, individuals who experienced ACEs can also undergo positive changes [12]. These positive changes are referred to as positive growth [13,14]. Similarly, those who have experienced trauma can undergo Posttraumatic growth, and those who have faced adversity can undergo adversarial growth [15,16].
Positive growth is associated with environmental conditions (type and severity of adverse event, elapsed time since event, previous life stressors), social factors (social support, religious involvement), psychological processes (rumination, coping), and positive mental health resources (hope, optimism, and self-esteem) [17,18].
The OTHERS(S) model for personal development suggests that promoting 8 core resources (i.e., the namesake of the acronym) can help promote Posttraumatic growth: Optimism, True meaning, Humor, Emotional intelligence, Resilience, Spirituality, and Self-confidence [19]. Relatedly, character strengths refer to the positive, trait-like capacities for thinking, feeling, and behaving in ways that benefit oneself and others [20]. Nearly all of the 24 types of character strengths include core resources mentioned in the OTHERS(S) model, and thus can be used as the model’s substitute measures. Previous studies have found positive associations between character strengths and Posttraumatic growth and valued outcomes (e.g., thriving, well-being, life satisfaction) [21]. Character strengths also helped to moderate the association between trauma and mental health issues such as depression [22–26].
University years (generally, when a person is 18 to 22 years of age) are a developmentally crucial period and a turbulent time whence the first onset of a broad range of mental disorders generally appears [27], especially among those with ACEs [28]. Approximately one-fourth of students in the People’s Republic of China experience anxiety [29]. However, mental health care for Chinese university students is complicated by misconceptions, stigma, low mental health literacy, and difficulty in accessing care [30]. Although a previous study found that Chinese cultural values of collectivism, deference to authority, and familyism influenced character strengths among health facility patients [31], Chinese cultural values, particularly those centered on Confucianism (e.g., deference to authority, modesty, harmony, and collectivism) also limit the ability to generalize findings from studies conducted in Western countries [32]. For example, youths who experienced abuse may regard their experience not as a traumatic experience but as a regular part of their family’s dynamics [33]. Growth from such experiences could be considered not as Posttraumatic or post-adversity growth but rather as part of a normal developmental process.
However, despite the vast literature on ACEs in high-income countries [6,34], few such studies have been conducted in China. Moreover, existing research in China tends to explore ACEs from the perspective of trauma [28–30]. Thus, there exists a knowledge gap on the association between ACEs, character strengths, positive growth, well-being, and depressive symptoms among university students in China. Such findings can provide empirical evidence for stakeholders in undergraduate mental health.
The objectives of this study are 1) to estimate the prevalence of ACEs among undergraduate students in Southern China; and 2) to assess the extent which mental health outcomes (positive growth, well-being, and depression) are associated with ACEs and character strengths among undergraduate students in Southern China.
We conducted a cross-sectional study using a self-administered survey at a university in Southern China. The university focused on health sciences and had approximately 20,000 students, mainly from the same region. The university also provided on-campus accommodation to students.
Study participants and sample size calculation
We included first and second-year undergraduate students over the age of 18 from all faculties. At the study university, undergraduates in the first and second years are generally between 18 to 20 years of age. We did not include upper-level students as their availability might vary according to the need to do an internship or practicum. We selected our study participants using systematic sampling with probability proportional to size.
We performed sample size calculation based on the first objective (to estimate the prevalence of ACEs among the students). We assumed that the population was infinite, and that 50% of the students had experienced one or more ACEs (p = 0.50) [35,36], with a margin of error of 5% (d = 0.05), at a 95% level of confidence (Z1−α/2 = 1.96). We used following formula for the calculation of sample size for proportion estimation:
We obtained a sample size of 384 students. However, we wished to obtain an adequate number of those who experienced four or more types of ACEs; thus, we decided to enlarge the sample size by an arbitrary 60% and obtained a sample size of 615 persons. We sent invitation to participate in our study to the students online. Thus, we assumed that an arbitrary 55% of those who received an electronic invitation would not respond to the invite and complete the survey, and further enlarged our sample size to 1400 students.
To assess the extent that ACEs and character strengths were associated with mental health outcomes (positive growth, well-being, and depressive symptoms), we calculated the sample size based on an assumption that 60% of the students with ACEs experienced a mental health problem (p1 = 0.60), whereas 40% of students without ACEs experienced a mental health problem (p2 = 0.40) [37]. We used the following formula for sample size calculation to assess the association between two proportions:
We obtained a sample size of 107 participants with ACEs and 107 participants without ACEs, or 214 participants in total. Assuming a non-response rate of 20%, we adjusted our sample size to 134 students in each group, or 268 students in total, for the mentioned assessment.
Our study instrument was a self-administered questionnaire that consisted of the following sections: 1) essential characteristics; 2) adverse childhood experiences (ACES); 3) character strengths; and 4) measurements of mental health outcomes, including positive growth, well-being, and depressive symptoms. Essential characteristics included gender, grade, family income per month, self-reported academic achievement, and whether the respondent had undergone psychological counseling.
Measurement of adverse childhood experiences (ACEs)
We used the Chinese version of the Adverse Childhood Experiences Questionnaire to measure the ACEs of our participants [1,38–40]. The questionnaire includes ten questions. The Chinese version of ACEs was developed using translation, back-translation, and cultural adaptation [39]. We assigned to each participant a score of 1 point for each reported adverse experience and 0 point for the otherwise. We used the Chinese version of the instrument [39] in the present study and added a follow-up question on each item concerning onset age for those who had the adverse experience. The reliability coefficient was 0.62 in the present study.
Measurement of character strengths
We used the Values in Action Inventory of Strengths (VIA-IS) instrument [41] to assess the character strengths of our study participants. The VIA-IS included 24 character strengths and the mean reliability coefficient of 24 character strengths was 0.85 [41]. We used the 72-item Chinese version of the instrument in this study. The Chinese version was developed under the World Health Organization’s basic guidelines for the translation and revision of measurement tools, balancing cultural commonality and cultural specificity [42]. We performed exploratory factor analysis on the responses to the VIA-IS questions and identified six factors/domains of character strengths. They were: Factor 1, humanity (six character strengths: appreciation of beauty and excellence, gratitude, kindness, spirituality, citizenship, love); Factor 2: wisdom (six character strengths: prudence, social intelligence, perspective, open-mindedness, self-regulation, leadership); Factor 3: temperance (three character strengths: fairness, forgiveness, humility/ modesty); Factor 4: vitality (two character strengths: zest, hope); Factor 5: courage (six character strengths: bravery, creativity, love of learning, integrity, persistence, curiosity); and Factor 6: humor (one character strength: humor). We have included the specific results of factor analyses as supplementary materials for reference. The mean reliability coefficient of all 24 strengths was 0.77 with the range of 0.61 to 0.89 in the present study.
Measurement of positive growth
We used the Chinese version of the Posttraumatic Growth Inventory (PTGI) [16] to measure positive growth among the study participants. The Chinese version of PTGI was developed using translation, back-translation, cultural adaptation, semantic analysis, and then reliability and validity analyses [43]. The PTGI consisted of 21 questions and assessed positive growth in 5 domains: New Possibilities, Relating to Others, Personal Strength, Spiritual Change, and Appreciation of Life. For this study, we used the Chinese version of the PTGI with Cronbach’s α coefficient being 0.83 and the re-test coefficient after two weeks was 0.71 [44]. The reliability coefficient was 0.95 in the present study.
We used the Chinese version of the WHO-5 questionnaire issued in 2007 by the Psychiatric Research Unit, WHO Collaborating Center for Mental Health, Frederiksborg General Hospital [45] to measure the well-being of our study participants. The WHO-5 [46] consists of 5 self-reported questions regarding the subjective well-being of the respondents. The original instrument’s sensitivity was 0.86, and the specificity was 0.81 [46]. Based on the responses, we summed the responses and calculated the raw well-being score, which ranged from 0 points (lowest level of well-being) to 25 points (highest level of well-being). The reliability coefficient was 0.91 in the present study.
Measurement of depressive symptoms
We measured depressive symptoms using the Centre for Epidemiologic Studies Depression Scale-Short Form (C-CES-D-SF). The instrument consisted of 9 self-reported depressive symptoms measurement questions with 4-point Likert scales [47]. We used a well-developed and widely used Chinese version of the CES-D-SF [48,49] with an internal consistency reliability of 0.86. All-item total correlations were higher than 0.5. The cut-off scores of the short version were 10 for depressive tendencies and 17 for high-risk depression. The reliability coefficient was 0.72 in the present study.
Investigators obtained the list of all first and second-year undergraduate students from the university. The investigators then used systematic sampling to sample 1400 students from the list. Investigators then sent electronic invitations (e-invitations) through the university’s e-learning system to the 1400 students and invited them to join the study. Students who responded were invited to the campus meeting hall. Research assistants then provided students with more information about the study and invited them to join the survey and answer the questionnaire. Research assistants told the students they were free to refuse participation with no consequence. Students who decided to participate went to the classroom next to the meeting hall to fill out the study questionnaire.
Study participants were asked to sign an informed consent form before completing the survey questionnaires. Due to the sensitive nature of the study and the respect for anonymity, we considered surveys from participants who gave consent but decided not to sign their name or used a pseudonym to be valid and included these responses in the analyses. We asked the study participants to sit adequately apart (one participant in every three seats) to prevent each participant from overlooking others’ responses. Participants who had finished filling their survey questionnaire were asked to place the questionnaire in an opaque box by themselves.
After receiving the questionnaires, the research assistant examined their completion and validity. Investigators considered questionnaires with less than two-thirds of the questions answered to be incomplete. Investigators excluded 5 participants (0.6%) who did not finish the ACE questionnaire and 28 participants (3.6%) who did not meet the other sections. The research assistant entered data from the remaining questionnaires into an electronic dataset.
We used descriptive statistics to describe the prevalence of ACEs and their co-occurrence among the study participants. We used the chi-square test of independence to compare the socio-demographic characteristics between participants with ACE(s) and those with no ACE. To assess the extent which ACEs and character strengths were associated with positive growth, well-being, and depressive symptoms, we used univariate (presence or absence of history of ACEs was the independent variable; positive growth, well-being, depressive symptoms were the dependent variables) and multivariate linear regressions (six domains of character strengths were the independent variables; positive growth, well-being, and depressive symptoms were the dependent variables). We identified confounders for multivariate linear regression based on factors associated with adverse childhood experiences as identified using the chi-square test of independence, as mentioned previously.
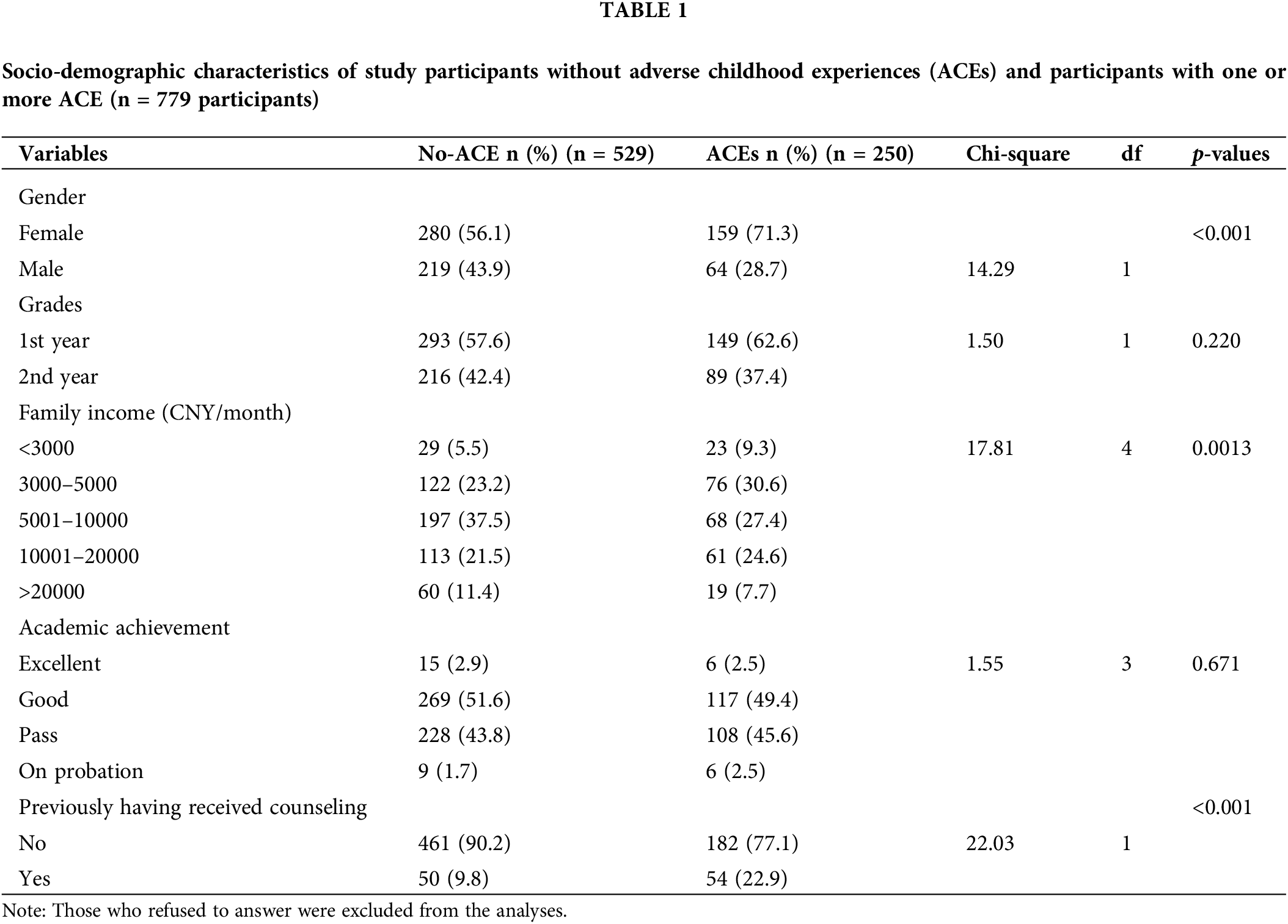
We sent invitations to 1400 students, with 588 (42%) males and 812 (58%) females. Then, 1103 students answered the invitation, 784 agreed to fill out the questionnaire, and 779 students finished the questionnaires. Among the 779 students who completed the questionnaire, 283 (36.3%) were males, 439 (56.4%) were females, and 57 (7.3%) did not indicate their gender. Participants who reported ACEs were more likely than participants who did not report ACEs to be female, to come from families with income of less than $700 per month, and to document a history of having received counseling (Table 1).
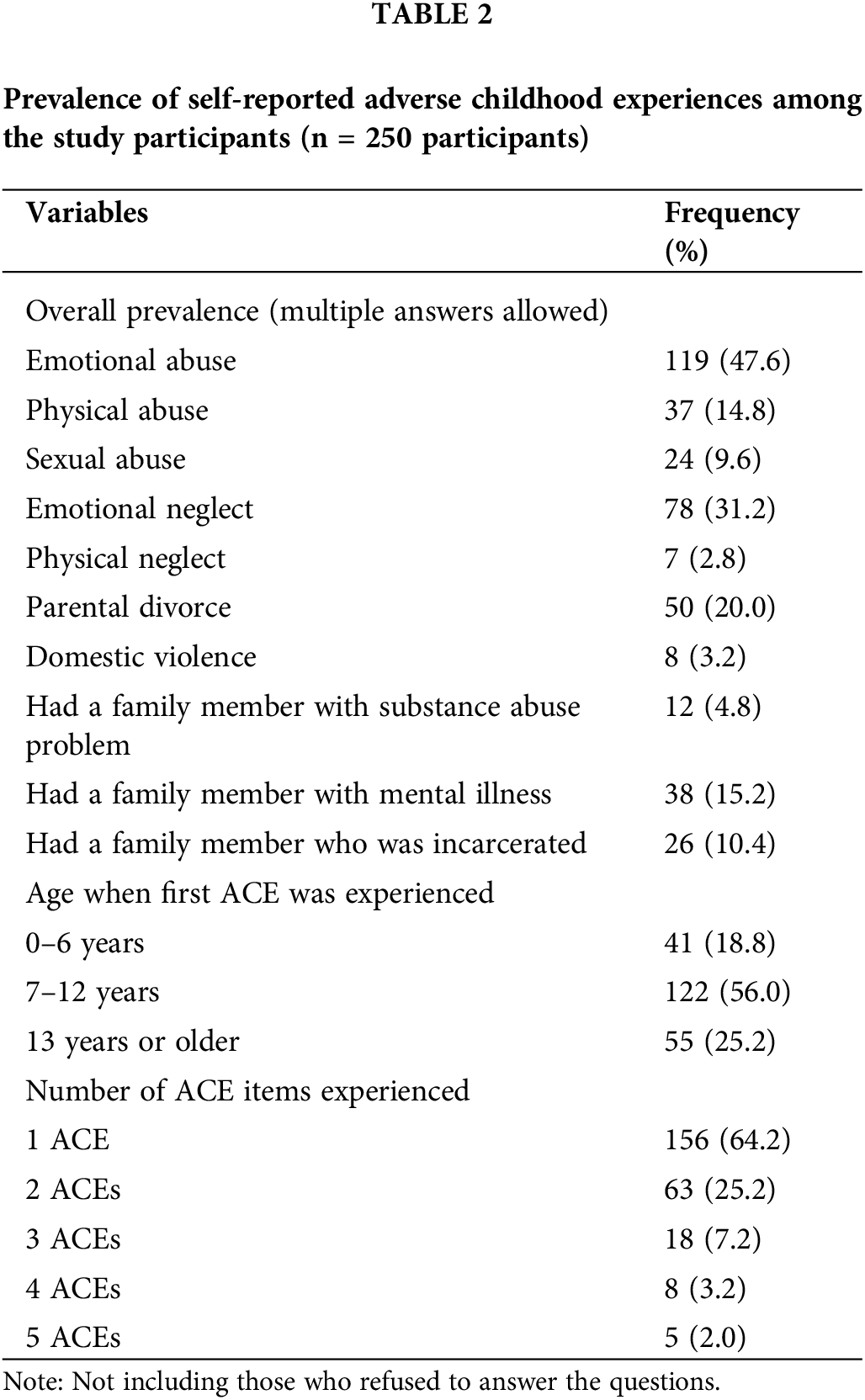
Of the 779 students who finished the questionnaire on ACEs, 250 students (32.1%) reported having experienced one or more ACEs, and approximately 13% of the participants said having experienced two or more ACEs. Among participants who reported ACEs, the most popular ACE was emotional abuse, followed by emotional neglect and parental divorce. The most common co-occurring ACE was also emotional abuse (Table 2). The number of experienced ACEs ranged from 1 to 5, and the most common age range when ACE was first experienced was 7 to 12 years old.
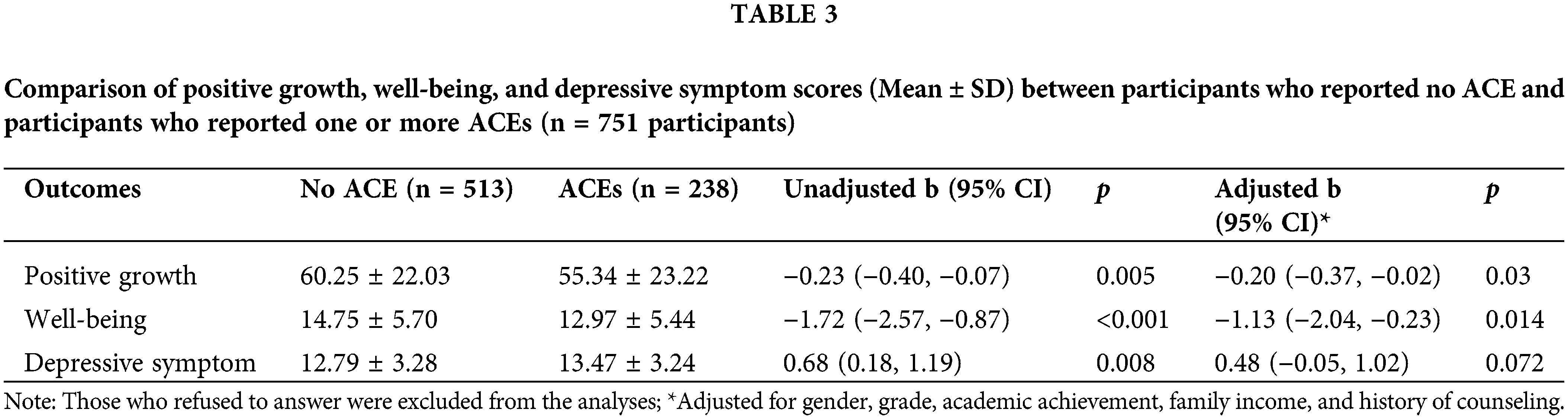
Compared to participants with no history of ACE, participants with a history of ACEs had significantly lower positive growth scores (Adjusted regression coefficient Beta = −0.20; 95% CI = −0.37, −0.02; p = 0.03*), significantly lower well-being scores (Adjusted Beta = −1.13; 95% CI = −2.04, −0.23; p = 0.014*), and marginal significantly higher depressive symptoms scores (Adjusted Beta = 0.48; 95% CI = −0.05, 1.02; p = 0.072) after adjusting for confounders (history of receiving counseling, gender, family income, and level of academic achievement) (Table 3).
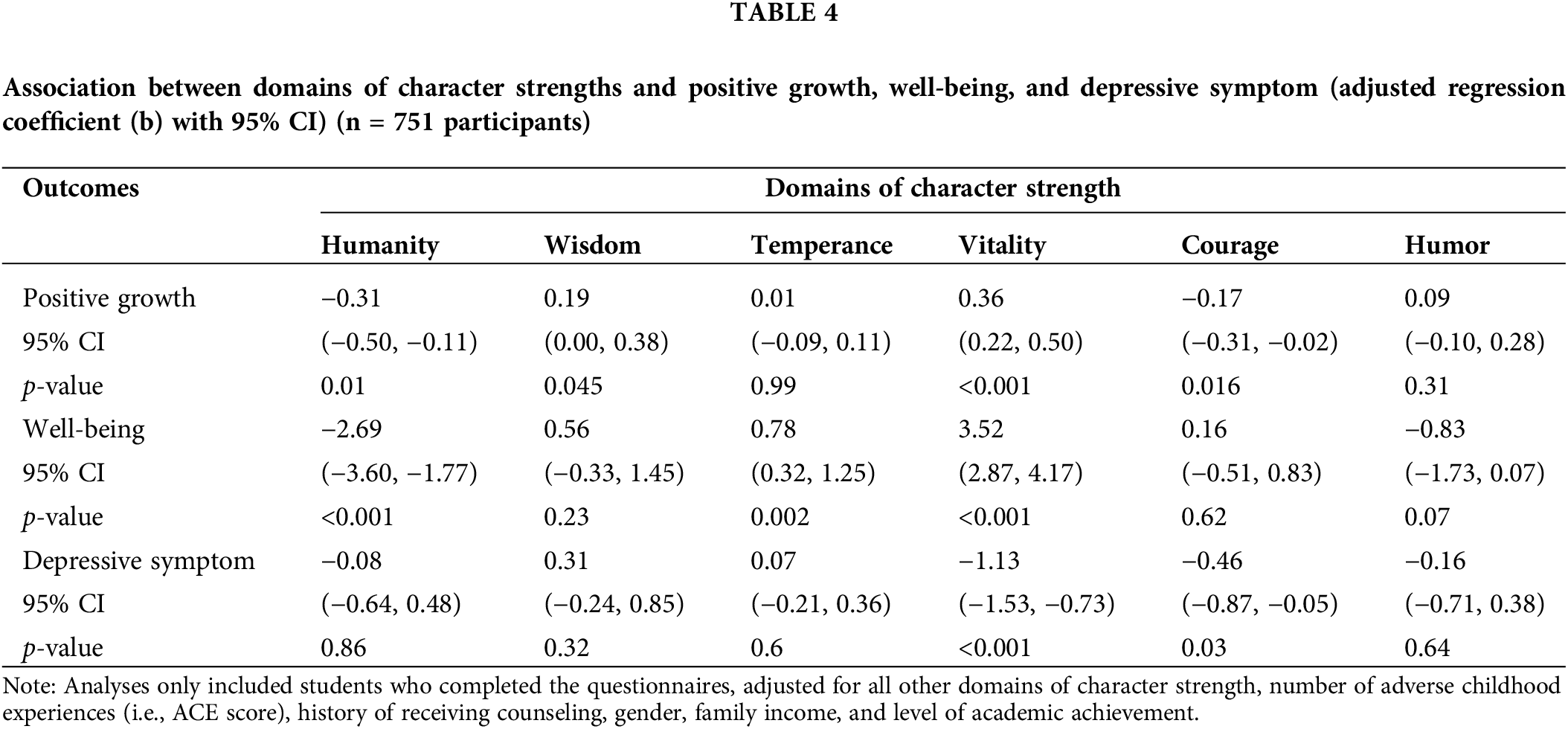
Associations between domains of character strength and mental health outcomes were heterogeneous (Table 4). Positive growth was significantly associated with humanity, wisdom, vitality, and courage. Well-being was significantly associated with humanity, temperance, and vitality. Depressive symptoms were associated with vitality and courage. Vitality was the only domain that was significantly associated with all three outcomes.
In this cross-sectional study, we described the prevalence and patterns of ACEs among university students in Southern China. We also found that positive growth, well-being, and depressive symptoms were associated with ACEs and various domains of character strengths. The findings of this study provide potentially helpful basic information for stakeholders in student mental health and also have implications for future intervention development.
The prevalence of ACEs among our study participants was lower than that among college students in the United States [50,51], Zambia [52], and Eritrea [53]. However, domestic violence and family dysfunctions are not commonly reported or discussed in public in China due to the perception of being a “private matter” and the fear of “losing face”. If the influence of such social desirability was present in our study, then the prevalence of ACEs could have been underestimated.
The proportion of students with more than 4 ACEs in our study was lower than in other studies. Students with multiple ACEs might have a lower chance of attending university, as ACEs are associated with health problems [5], reduced intelligence [54], and cognitive deficits [55] during childhood and adolescence. Thus, our findings are generalizable only to university students in similar settings.
History of ACEs was negatively associated with positive growth and well-being. These findings were similar to those of previous major studies that ACEs were associated with poorer mental health [6–9,56]. However, the outcomes of our study were measured using a self-reported questionnaire with no probing. Such under-reporting could have introduced information bias to the study findings.
Domains of character strengths were associated with positive growth, well-being, and depressive symptom scores, with vitality being significantly associated with all three outcomes. The findings of our study were consistent with those of a survey among earthquake survivors in Sichuan, China [57], which found an association between character strengths and Posttraumatic growth. Vitality explained 32% of the variance in post-traumatic or positive growth among those with indirect trauma. According to our exploratory factor analysis, vitality included hope and zest. Peterson and colleagues also found that hope and zest are strongly associated with posttraumatic growth among those who have experienced at least one traumatic event [21]. It is possible that positive growth and well-being can be promoted among university students and depressive symptoms can be relieved through interventions involving hope and zest. Character strengths-based intervention (CSI) is an intervention in positive psychology that aims to identify, use, and develop character strengths [22,23]. Future studies should consider incorporating hope and zest into CSI as a way to promote growth and mental health among university students with ACEs.
Positive growth was significantly associated with humanity, wisdom, vitality, and courage. These associations indicated that identifying, using, and developing the following strengths might promote positive growth among university students with ACEs: appreciation of beauty and excellence, gratitude, kindness, spirituality, citizenship, love, prudence, social intelligence, perspective, open-mindedness, self-regulation, leadership, zest, hope, brave, creativity, love of learning, integrity, persistence, and curiosity. Well-being was significantly associated with humanity, temperance, and vitality. Thus, identifying, using and developing the following strengths might increase well-being among university students with ACEs: appreciation of beauty and excellence, gratitude, kindness, spirituality, citizenship, love, fairness, forgiveness, humility/modesty, zest, and hope. Depressive symptom was associated with vitality and courage, which suggested that identifying, using, and developing the following strengths might decrease depressive symptoms among university students with ACEs: zest, hope, bravery, creativity, love of learning, integrity, persistence, and curiosity.
All factors but humor had a significant association with one of the outcomes among positive growth, well-being, and depressive symptoms. Therefore, a long-term intervention to identify, use, and develop all 24 character strengths as a course might be a possible way to support university students with ACEs.
A number of limitations existed in our study. Firstly, the study’s cross-sectional design did not allow for causal inference. Secondly, participants might not have been able to recall adverse childhood experiences, potentially introducing information bias into the study findings. Thirdly, our survey was conducted in a classroom on campus with the instructor located at the back of the classroom, which could have invoked reactivity and social desirability bias, potentially contributing to the under-reporting of ACEs. Lastly, our participants were students at one university in Southern China. The findings of the study might have limited generalizability to other populations. These caveats should be considered in the interpretation of the study findings.
The prevalence of ACEs among university students in Southern China was relatively high. ACEs were negatively associated with positive growth, and well-being and marginally positively related to depressive symptoms. In contrast, the vitality domain of character strength was the opposite, and positively related to positive growth and well-being and negatively associated with depressive symptoms. The findings of this study contributed empirical evidence for stakeholders in university mental health and can potentially inform the development of future interventions. However, caveats regarding lack of temporality, selection bias, social desirability bias, and lack of generalizability should be considered in the interpretation of the study findings.
Acknowledgement: We would like to thank the study participants for sharing their experiences and time. We also would like to thank all research assistants and support staff for working on this study.
Funding Statement: This research was funded by the Guangdong Provincial Philosophy and Social Science Planning Project (GD22XJY25).
Author Contributions: The authors confirm their contribution to the paper as follows: study conception and design: Y. Yulan, C. Rassamee; data collection: Y. Yulan, K. Hujiao, W. Chonghua; analysis and interpretation of results: Y. Yulan, W. Wit, W. Chonghua; draft manuscript preparation: Y. Yulan. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available from now on in the following link: https://figshare.com/s/434411b28621e4da3ebb.
Ethics Approval: We received ethical approval for the study from the Human Research Ethics Committee, Faculty of Medicine, Prince of Songkla University, Hat Yai, Thailand (Approval Number: REC.63-382-18-1) and the Medical Ethics Committee of the Affiliated Hospital of Guangdong Medical University (Approval Number: PJ2020-097).
Conflicts of Interest: The authors declare they have no conflicts of interest to report regarding the present study.
References
1. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. Am J Prev Med. 1998;14(4):245–58. doi:10.1016/S0749-3797(98)00017-8. [Google Scholar] [PubMed] [CrossRef]
2. Ji S, Wang H. ERPs study of the relationship between adverse childhood experiences and inhibitory ability among college students. Chin J Sch Health. 2018;39:1667–70. doi:10.16835/j.cnki.100-9817.2018.11.018. [Google Scholar] [CrossRef]
3. Anda RF, Butchart A, Felitti VJ, Brown DW. Building a framework for global surveillance of the public health implications of adverse childhood experiences. Am J Prev Med. 2010;39(1):93–8. doi:10.1016/j.amepre.2010.03.015. [Google Scholar] [PubMed] [CrossRef]
4. World Health Organization. Adverse Childhood Experiences International Questionnaire (ACE-IQ). Available from: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq) (accessed on 28/01/2020) [Google Scholar]
5. Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield CH, Perry BD, et al. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):174–86. doi:10.1007/s00406-005-0624-4. [Google Scholar] [PubMed] [CrossRef]
6. Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, et al. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health. 2017;2(8):e356–66. doi:10.1016/S2468-2667(17)30118-4. [Google Scholar] [PubMed] [CrossRef]
7. Freeny J, Peskin M, Schick V, Cuccaro P, Addy R, Morgan R, et al. Adverse Childhood experiences, depression, resilience, & spirituality in African-American adolescents. Journ Child Adol Trauma. 2021;14(2):209–21. doi:10.1007/s40653-020-00335-9. [Google Scholar] [PubMed] [CrossRef]
8. Lew D, Xian H. Identifying distinct latent classes of adverse childhood experiences among us children and their relationship with childhood internalizing disorders. Child Psychiatry Hum Dev. 2019;50(4):668–80. doi:10.1007/s10578-019-00871-y. [Google Scholar] [PubMed] [CrossRef]
9. Burlaka V, Hong JS, Churakova I, Serdiuk O, Proskura V, Shvets D. The role of adverse childhood experiences and corporal punishment in early adulthood depression and substance use among Ukrainian college students. J Fam Violence. 2020;35(3):285–95. doi:10.1007/s10896-019-00110-x. [Google Scholar] [CrossRef]
10. Seon J, Cho H, Choi G, Son E, Allen J, Nelson A, et al. Adverse childhood experiences, intimate partner violence victimization, and self-perceived health and depression among college students. J Fam Violence. 2021. Available from: https://link.springer.com/article/10.1007/s10896-021-00286-1 (accessed on 17/07/2021) [Google Scholar]
11. Ding C, Wang T, Chen X, Li J, Wang W, Huang D, et al. Association of Adverse childhood experience and attention deficit hyperactivity disorder with depressive symptoms among men who have sex with men in China: Moderated mediation effect of resilience. BMC Public Health. 2019;19(1):1706. doi:10.1186/s12889-019-8016-2. [Google Scholar] [PubMed] [CrossRef]
12. Wu X, Kaminga AC, Dai W, Deng J, Wang Z, Pan X, et al. The prevalence of moderate-to-high posttraumatic growth: A systematic review and meta-analysis. J Affect Disorder. 2019;243:408–15. doi:10.1016/j.jad.2018.09.023. [Google Scholar] [PubMed] [CrossRef]
13. Linley PA, Joseph S. Positive change following trauma and adversity: A review. J Traum Stress. 2004;17:11–21. doi:10.1023/B:JOTS.0000014671.27856.7e. [Google Scholar] [PubMed] [CrossRef]
14. Russo-Netzer P, Moran G. Positive growth from adversity and beyond: Insights gained from cross-examination of clinical and nonclinical samples. Am J Ortho psychiatry. 2018;88(1):59–68. doi:10.1037/ort0000224. [Google Scholar] [PubMed] [CrossRef]
15. Fortune D, Richards H, Griffiths C, Main C. Adversarial growth in patients undergoing treatment for psoriasis: A prospective study of the ability of patients to construe benefits from negative events. Psychol Health Med. 2005;10(1):44–56. doi:10.1080/13548500512331315352. [Google Scholar] [CrossRef]
16. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: Measuring the positive legacy of trauma. J Traum Stress. 1996;9(3):455–71. doi:10.1002/jts.2490090305. [Google Scholar] [CrossRef]
17. Levine SZ, Laufer A, Stein E, Hamama-Raz Y, Solomon Z. Examining the relationship between resilience and posttraumatic growth. J Trauma Stress. 2009;22(4):282–6. doi:10.1002/jts.20409. [Google Scholar] [PubMed] [CrossRef]
18. Nuttman-Shwartz O. Shared resilience in a traumatic reality: A new concept for trauma workers exposed personally and professionally to collective disaster. Trauma Violence Abuse. 2015;16(4):466–75. doi:10.1177/1524838014557287. [Google Scholar] [PubMed] [CrossRef]
19. Fazio RJ. Growth consulting: Practical methods of facilitating growth through loss and adversity. J Clin Psychol. 2009;65(5):532–43. doi:10.1002/jclp.20590. [Google Scholar] [PubMed] [CrossRef]
20. Peterson C, Seligman MEP. Character strengths and virtues: A handbook and classification. New York, USA: American Psychological Association; 2004. [Google Scholar]
21. Peterson C, Park N, Pole N, D’Andrea W, Seligman MEP. Strengths of character and posttraumatic growth. J Trauma Stress. 2008;21:214–7. doi:10.1002/jts.20332. [Google Scholar] [PubMed] [CrossRef]
22. Kumar PA, Mohideen F. Strengths-based positive schooling interventions: A scoping review. Contemp School Psychol. 2021;25:86–98. doi:10.1007/s40688-019-00260-1. [Google Scholar] [CrossRef]
23. Niemiec RM. Character strengths interventions: A field guide for practitioners. Gottingen, Germany: Library of Congress Cataloging in Publication; 2017. [Google Scholar]
24. Schutte NS, Malouff JM. The impact of signature character strengths interventions: A meta-analysis. SpringerLink. 2018. Available from: https://link.springer.com/article/10.1007/s10902-018-9990-2 (accessed on 18/09/2021) [Google Scholar]
25. Niemiec RM. VIA character strengths—research and practice: The first 10 years. Available from: http://link.springer.com/chapter/10.1007/978-94-007-4611-4_2 (accessed on 12/09/2021) [Google Scholar]
26. Niemiec RM. Six Functions of character strengths for thriving at times of adversity and opportunity: A theoretical perspective. Appl Res Qual Life. 2020;15(2):551–72. doi:10.1007/s11482-018-9692-2. [Google Scholar] [CrossRef]
27. Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27(1):281–95. doi:10.1038/s41380-021-01161-7. [Google Scholar] [PubMed] [CrossRef]
28. Bruffaerts R, Mortier P, Kiekens G, Auerbach RP, Cuijpers P, Demyttenaere K et al. Mental health problems in college freshmen: Prevalence and academic functioning. J Affect Disorder. 2018;225:97–103. doi:10.1016/j.jad.2017.07.044. [Google Scholar] [PubMed] [CrossRef]
29. Wang X, Liu Q. Prevalence of anxiety symptoms among Chinese university students amid the COVID-19 pandemic: A systematic review and meta-analysis. Heliyon. 2022;8(8):e10117. doi:10.1016/j.heliyon.2022.e10117. [Google Scholar] [PubMed] [CrossRef]
30. Ning X, Wong JPH, Huang S, Fu Y, Gong X, Zhang L, et al. Chinese university students’ perspectives on help-seeking and mental health counseling. Int J Environ Res Public Health. 2022;19(14):8259. doi:10.3390/ijerph19148259. [Google Scholar] [PubMed] [CrossRef]
31. Yan T, Chan CWH, Chow KM, Li M. Experiences and perception of character strengths among patients with breast cancer in China: A qualitative study. BMJ Open. 2022;12(10):e061994. Available from: https://pubmed.ncbi.nlm.nih.gov/36307158/ (accessed on 14/09/2023) [Google Scholar]
32. Shek DTL, Yu L, Fu X. Confucian virtues and Chinese adolescent development: A conceptual review. Int J Adolesc Med Health. 2013;25(4):335–44. doi:10.1515/ijamh-2013-0031. [Google Scholar] [PubMed] [CrossRef]
33. Xia Y, Li SD, Liu TH. The interrelationship between family violence, adolescent violence, and adolescent violent victimization: An application and extension of the cultural spillover theory in China. Int J Environ Res Public Health. 2018;15(2):371. doi:10.3390/ijerph15020371. [Google Scholar] [PubMed] [CrossRef]
34. Stoltenborgh M, Bakermans-Kranenburg MJ, Alink LRA, van IJzendoorn MH. The Prevalence of child maltreatment across the globe: Review of a series of meta-analyses. Child Abuse Rev. 2015;24(1):37–50. doi:10.1002/car.2353. [Google Scholar] [CrossRef]
35. Fu H, Feng T, Qin J, Wang T, Wu X, Cai Y, et al. Reported prevalence of childhood maltreatment among Chinese college students: A systematic review and meta-analysis. PLoS One. 2018;13(10):e0205808. doi:10.1371/journal.pone.0205808. [Google Scholar] [PubMed] [CrossRef]
36. McGavock L, Spratt T. Prevalence of adverse childhood experiences in a university population: Associations with use of social services. Brit J Soc Work. 2014;44(3):657–74. doi:10.1093/bjsw/bcs127. [Google Scholar] [CrossRef]
37. Liming KW, Grube WA. Wellbeing outcomes for children exposed to multiple adverse experiences in early childhood: A systematic review. Child Adolesc Soc Work J. 2018;35(4):317–35. doi:10.1007/s10560-018-0532-x. [Google Scholar] [CrossRef]
38. CDC. About the CDC-kaiser ACE study. Violence Prevention. Injury Center. 2021. Available from: https://www.cdc.gov/violenceprevention/aces/about.html (accessed on 30/07/2021) [Google Scholar]
39. Mints. Adverse childhood experience, ACE. Psych Space. 2020. Available from: https://www.psychspace.com/psych/viewnews-15485 (accessed on 15/06/2020) [Google Scholar]
40. Weber S, Lynch S. Understanding the relations among adverse childhood experiences (ACEsubstance use, and reoffending among detained youth. Child Abuse Negl. 2021;120(4):105211. doi:10.1016/j.chiabu.2021.105211. [Google Scholar] [PubMed] [CrossRef]
41. McGrath RE. Technical report: The VIA assessment suite for adults: Development and initial evaluation. Revised Edition. Cincinnati, OH: VIA Institute on Character; 2019. [Google Scholar]
42. Tsinghua University Positive Psychology Center. Chinese version of character strength scale. WJX. Available from: https://www.wjx.cn/xz/42969879.aspx? (accessed on 31/07/2021) [Google Scholar]
43. Wang J, Chen Y, Wang Y, Liu X. Revision of the posttraumatic growth inventory and testing its reliability and validity. J Nurs Sci. 2011;26:26–8. doi:10.1007/s12144-021-02645-z. [Google Scholar] [CrossRef]
44. Geng Y, Xu Q, Liu H, Xu X. Reliability and validity analysis of The Chinese version of the post-traumatic Growth Inventory in multiple trauma survivors. Chin J Nurs. 2011;46:1003–5. [Google Scholar]
45. Psykiatric Center North Zealand. WHO5-Chinese-PR. 2007. Available from: https://www.psykiatri-regionh.dk/who-5/Documents/WHO5_Chinese_PR.pdf (accessed on 31/07/2021) [Google Scholar]
46. Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 well-being index: A systematic review of the literature. PPS. 2015;84(3):167–76. doi:10.1159/000376585. [Google Scholar] [PubMed] [CrossRef]
47. Martens MP, Parker JC, Smarr KL, Hewett JE, Ge B, Slaughter JR, et al. Development of a shortened center for epidemiological studies depression scale for assessment of depression in rheumatoid arthritis. Rehabil Psychol. 2006;51(2):135–139. doi:10.1037/0090-5550.51.2.135. [Google Scholar] [CrossRef]
48. He J, Chen Z, Guo F, Zhang J, Yang Y, Wang Q. Short form of Chinese version of center for epidemiologic studies depression scale. Chin J Behav Med & Brain Sci. 2013;22:1133–6. doi:10.3760/cma.j.issn.1674-6554.2013.12.023. [Google Scholar] [CrossRef]
49. Zhang B, Li J. Reliability and validity of a short version of center for epidemiologica studies depression scale in national adult population. Chin Ment Health J. 2011;25:506–11. doi:10.3969/j.issn.1000-6729.2011.07.007. [Google Scholar] [CrossRef]
50. Grigsby TJ, Rogers CJ, Albers LD, Benjamin SM, Lust K, Eisenberg ME, et al. Adverse childhood experiences and health indicators in a young adult, college student sample: Differences by gender. Int J Behav Med. 2020;27(6):660–7. doi:10.1007/s12529-020-09913-5. [Google Scholar] [PubMed] [CrossRef]
51. Lemon ED, Vu M, Roche KM, Hall KS, Berg CJ. Depressive symptoms in relation to adverse childhood experiences, discrimination, hope, and social support in a diverse sample of college students. J Racial Ethnic Health Disparities. 2022. Available from: https://link.springer.com/article/10.1007/s40615-021-01038-z (accessed on 18/07/2021) [Google Scholar]
52. Zhang J, Tang B, Liu M, Yuan S, Yu H, Zhang R, et al. Association of adverse childhood experiences with health risk behaviors among college students in Zambia. IntJ Behav Med. 2020;27(4):400–5. doi:10.1007/s12529-020-09863-y. [Google Scholar] [PubMed] [CrossRef]
53. Wang P, Kelifa MO, Yu B, Yang Y. Classes of childhood adversities and their associations to the mental health of college undergraduates: A nationwide cross-sectional study. Environ Health Prev Med. 2021;26(1):73. doi:10.1186/s12199-021-00993-7. [Google Scholar] [PubMed] [CrossRef]
54. Platt J, Luedtke A, Ahern J, Kaufman A, Keyes K. Targeted estimation of the relationship between childhood adversity and fluid intelligence in a US population sample of adolescents. Am J Epidemiol. 2018;187(7):1456–66. doi:10.1093/aje/kwy006. [Google Scholar] [PubMed] [CrossRef]
55. Geoffroy MC, Pinto Pereira S, Li L, Power C. Child neglect and maltreatment and childhood-to-adulthood cognition and mental health in a prospective birth cohort. J Am Acad Child PSY. 2016;55(1):33–40.E3. doi:10.1016/j.jaac.2015.10.012. [Google Scholar] [PubMed] [CrossRef]
56. Moore KA, Ramirez AN. Adverse childhood experience and adolescent well-being: Do protective factors matter? Child Ind Res. 2016;9(2):299–316. doi:10.1007/s12187-015-9324-4. [Google Scholar] [CrossRef]
57. Duan W, Guo P. Association between virtues and posttraumatic growth: Preliminary evidence from a Chinese community sample after earthquakes. PeerJ. 2015;3:e883. doi:10.7717/peerj.883. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools