
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Coping with Trauma: The Relationship between Religiosity, Spirituality, and Post-Traumatic Symptoms among Civilians Exposed to Ongoing Rocket-Fire
Faculty of Welfare and Health Sciences, University of Haifa, Haifa, 31905, Israel
* Corresponding Author: Michael Weinberg. Email:
International Journal of Mental Health Promotion 2023, 25(10), 1137-1145. https://doi.org/10.32604/ijmhp.2023.029641
Received 01 March 2023; Accepted 20 June 2023; Issue published 03 November 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Living under ongoing shelling and missile attacks could cause a widespread of disruption of everyday life and emotional distress. Coping with such distress could be associated with the personal resources of religion and spirituality. The present study aimed to examine the relationships between religiosity and spirituality with Post Traumatic stress Disorder (PTSD) symptoms among a civilian population frequently exposed to missile and rocket threats. One hundred and twenty-four (N = 124) civilian participants living within 10 km from shelling and missile attacks fired towards them, completed demographic, religiosity, spirituality, and PTSD questionnaires. The study findings demonstrate that religiosity is associated with higher levels of PTSD symptoms while spirituality is associated with lower levels of PTSD symptoms. When dividing the sample into two groups-religious and secular, no association was found between religiosity and PTSD symptoms among the religious group, whereas among the secular group, there was a positive association. Spirituality was negatively associated with PTSD symptoms among both groups. This study may offer a significant contribution to models of intervention following continued exposure to trauma, emphasizing the importance of spiritually and sensitivity to religion while coping with PTSD symptoms. Theoretical and practical implications are discussed.Keywords
In recent years, residents of southern Israel have been under the constant threat of terror attacks. For nearly two decades, the city of Sderot, located approximately 10 km from the Israel–Gaza border, and its surrounding communities have suffered from ongoing shelling and missile attacks [1]. One of the intense rounds of escalation took place during November 2018 were over 400 rockets and mortar shells were fired into this area during a period of 2 days [2]. Living under such circumstances causes deaths, injuries, damage, and widespread disruption of everyday life for the civilian population. As a result, many residents of this area suffer from emotional distress, including depression, dissatisfaction of life, bereavement, the development of hostile and negative approaches to life, feelings of threat, tension and dysfunction, and posttraumatic stress disorder (PTSD) symptoms [3,4]. In contrast to a single terror attack, the rocket attacks on these communities have continued over time, causing heightened distress and disruption of daily life and undermining the sense of security among the civilian population [1]. In addition, many citizens have suffered the loss of social support and community resources as relatives and friends have moved away from the area [5].
The way that individuals cope with such distress can vary with the environmental and personal resources available to them [6]. According to the Conservation of Resources Theory [6–8], in order to deal with stressful situations and traumatic events, individuals strive to obtain, retain, and protect the resources available to them. As the level of access to these resources increases, the level of stress decreases. Similarly, an actual or threatened loss of resources can increase the level of stress experienced. Effective coping in these situations involves turning to and using internal and external resources from other areas to alleviate the experience of distress. Among the internal resources at the disposal of the individual dealing with stress and trauma, religiosity [9] and spirituality [10,11] have been found to significantly affect the development of PTSD symptoms.
Religiosity is defined by the research literature in various ways such as the belief in a divine or supreme power, belonging to a religious community, and formal and cultural institutionalization of spiritual conceptions, which include a broad spectrum of beliefs, such as Christianity, Islam, Buddhism, etc. [12]. Others have defined religiosity as loyalty to a set of values, moral codes, activities, customs, and rituals that have developed within a particular community [13]. In the present study, religiosity will be defined and examined as the extent to which one believes in God and is dedicated to a formal system of values, commandments, and his level of loyalty to the religious scholars.
Various studies conducted among diverse cultures and religions around the world have found that religiosity can aid mental health; enhance quality of life; produce a wide range of positive feelings, such as satisfaction and joy; and reduce negative feelings, such as anxiety and depression [14]. Over the past three decades, significant correlations have been found between religiosity and PTSD following traumatic events. Although there is no consensus regarding the direction of these relationships [9,15], most studies in this area have demonstrated negative relationships between religiosity and PTSD symptoms [15–17]. Studies have also indicated that religious activities and beliefs have a great impact on the way an individual perceives a traumatic event and may mediate the way in which environmental and personal components influence the development of PTSD [15]. Religious beliefs may moderate nonadaptive thoughts about a traumatic event and allow one to believe that there is a positive purpose for these kinds of events. In addition, religiosity provides many people with answers to difficult questions that arise after a traumatic event, can help to dissipate feelings of loneliness and can help affected individuals to assign the traumatic event a position in an orderly cognitive system, allowing a sense of inner control [9].
However, other studies have found that high levels of religiosity are associated with high levels of PTSD [18,19]. These findings suggest that traumatic exposure may cause the development of PTSD and, at the same time, intensify one’s use of religious activity and beliefs to cope with PTSD symptoms [15]. For example, religious conservatism may express a psychological need to reduce the uncertainty and the sense of threat created by the traumatic exposure [20]. In addition, research literature has found that different forms of negative religious coping strategies can cause high levels of distress, anxiety and depression and poor health-related outcomes while facing negative life stressors [21,22]. These negative religious coping include religious conflict within oneself, with God, and with other people [23]. For example, in response to traumatic stressors’ one might feel abandoned by God [24] or by his community of faith [22]. Some individuals’ religious beliefs can also lead them to view a traumatic event as a divine punishment or an act of the devil. Thus, increasing their sense of threat and distress [25]. In addition, one might suffer from feelings of guilt, a lack of love, and a sense that God acts in a careless manner. These feelings and thoughts can be detrimental to one’s self-worth and can undermine an individual’s sense of resilience, increasing levels of PTSD [24].
Another resource that relates to religiosity and which has also begun to be explored in recent years within the context of trauma is spirituality [10,11]. Spirituality refers to a person’s belief in a supreme power that is above his or her own existence and which provides the individual with a feeling of transcending the present realistic context [26], as well as a sense of harmony with one’s self, others, and one’s surroundings [27]. Some people will use the word God to express this experience, while others will prefer to use other terms [26]. While many studies have not sufficiently distinguished between spirituality and religiosity [13], others have referred to them as distinct phenomena and emphasized the need to distinguish between spirituality and religiosity both theoretically and operationally [12,28]. Following this second approach, spirituality can be defined as a concept connected to a variety of human traits that aid in mental-health issues and well-being [29]. According to Dyson et al. [27], spirituality represents an inner sense of wholeness and harmony with the environment and the community in which a person lives and includes diverse attributes such as the ability to give, forgive, receive love, and maintain beneficial interpersonal relationships and human contacts, including love, hope, attention, caring, trust, and honesty. Spirituality also encompasses a sense of meaning in life and internal integrity, which results from the adoption of beliefs and values that empower one’s inner resources and manifest in diverse fields in the life of the individual [27]. Similarly to Dysons’ approach, Howden [30] defined spirituality as the dimension of one’s being able to integrate or unify factors of interconnectedness, purpose and meaning in life, inner resources (harmony, balance, peace, etc.) and transcendence. In the present study, the term spirituality was distinguished from religiosity as demonstrated in Dysons’ and Howdens’ studies.
Various studies have found that spirituality helps individuals to cope with traumatic events, providing protection against negative effects of exposure to those events [31], and also helps to reduce PTSD symptoms [13,32]. For example, a study examining the relationship between spirituality and PTSD among African-American women who had experienced domestic violence, found that the women who reported higher levels of spirituality suffered less from depression [11]. Similar findings were also reported for victims of sexual assault who used spiritual resources to deal with the emotional distress they experienced due to that traumatic experience [33]. Another study, conducted after the September 11, 2001 terror attacks, found an increased need to adopt different aspects of spirituality among individuals who were exposed to the traumatic events of that day [34].
To date, research has examined the relationship between religiosity and spirituality, on the one hand, and PTSD, on the other, in the context of various types of trauma events. However, no studies have been conducted among a civilian population that is continuously exposed to missiles and rocket fire. In order to bridge this gap, the present study examined the relationship between religiosity and spirituality, on the one hand, and PTSD symptoms, on the other, among civilians in southern Israel who are frequently exposed to rocket fire and missile attacks.
Accordingly, two research hypotheses were examined:
1. A negative correlation will be found between religiosity and PTSD symptoms. Thus, higher levels of religiosity will be associated with lower levels of PTSD symptoms.
2. A negative correlation will be found between spirituality and PTSD symptoms. Thus, higher levels of spirituality will be associated with lower levels of PTSD symptoms.
In contrast, a null hypothesis (H0) of study variables will predict no correlations between religiosity and PTSD symptoms, and no correlations between spirituality and PTSD symptoms.
The sample of this study consisted of 124 residents living 10 km or less from the border of the Gaza Strip. All of them had been exposed to mortar fire and missile attacks over the previous 5 years. Ninety-four of the participants were women (75.8%) and 30 were men (24.2%). The average age of the participants was 38.16 (M = 38.16, SD = 14.21). The average duration of residence in this area was 19.25 years (SD = 15.38). All participants were Jewish. Sixty-two participants (50%) defined themselves as secular, 53 (42.7%) as religious, and the rest (nine participants; 7.3%) as traditional. Thirty-one participants were single, 88 were married, and 5 were divorced or widowed. The married participants had been married for an average of 16.34 years (SD = 12.27). Eighty-five participants (68.6%) reported that they had a high financial status, 35 (28.2%) reported an average financial status, and 4 (3.2%) reported a low financial status. On average, the participants had 14.62 years of education (SD = 2.43). As for exposure to previous traumatic events, 88 (71%) reported having experienced no previous traumatic events other than the rocket fire in their area of residence.
Demographic questionnaire. This questionnaire covered variables such as age, gender, education, financial status, country of birth, prior exposure to traumatic experience such as a car accident, sexual assault, severe violence, terrorist attack, participating in a combat exposure or other traumatic exposure (while allowing an open answer by the respondent), and duration of residence in the affected region. Additionally, participants were asked to determine whether they are secular or religious. It should be noted that in Israeli culture people who define themselves as secular are not necessarily detached from religious rituals and practices, and therefore may rate themselves at different levels of religiosity. Thus, many seculars believe in god, and maintain active connections with belief systems and Jewish cultural practices such as the ritual circumcision of males, and lighting candles on the eve of Saturday and holidays. Yet, while orthodox religious individuals expressly consider themselves to be committed to the Jewish laws, a person who defines himself as secular feels free to choose which customs and rituals he observes and which ones he does not observe [35].
Religiosity questionnaire. Religiosity was measured using a religiosity evaluation questionnaire compiled by Falach [36] and based on Ben–Meir and Kedem–Friedrich’s religiosity questionnaire [37]. This questionnaire examines religious faith and the living of a religious lifestyle, defining the level of religiosity in principle without any affiliation with any particular religion. This questionnaire includes seven items that are each rated on a 7-point Likert scale ranging from 1 (not at all) to 7 (very much). Higher scores represent higher levels of religiosity (Example questions: “To what extent do you believe in God”; “To what extent do you feel obligated to fulfill your religious obligations”; “To what extent do you feel obligated to obey the religious leaders”). The Cronbach’s alpha internal consistency coefficient for this scale in the current study was 0.97.
Spirituality questionnaire. Spirituality was measured using the Spirituality Assessment Scale (SAS), which was developed by Howden [30] and has been proven to be reliable and valid for the measurement of spirituality, regardless of the individual’s religious activity. The 28 items of the SAS are each rated on a 6-point scale ranging from strongly disagree to strongly agree. (Example questions: “I have a sense of inner harmony or peace”; “My life has meaning and purpose”; “I can enter a spiritual dimension within myself for guidance”). The Cronbach’s alpha internal consistency coefficient for the SAS scale in the current study was 0.63.
PTSD symptoms. PTSD symptoms were evaluated using the PTSD Symptom Levels Scale (PSL) questionnaire compiled by Gil et al. [38]. The PSL is a 20-item, self-report questionnaire that aims to assess the level of PTSD symptoms over the preceding week, complying with the criteria for PTSD diagnosis as presented in the DSM-5. The severity of each item is rated on a 4-point Likert scale ranging from 1 (not at all or once a week) to 4 (five times a week or more). The scale is divided into four clusters: intrusion (Questions 1–5), avoidance (Questions 6 and 7), negative alterations (Questions 8–14), and alterations in arousal (Questions 15–20). In the present study, high correlations were found between the different subscales, therefore data analysis was based on the total score of PSL. The total severity score is calculated as the mean of the respondent’s ratings of the 20 items. Cronbach’s alpha internal consistency coefficient of the present scale in this study was 0.93.
Following the approval of the University of Haifa ethics committee (408/18), Israelis living up to 10 km from the Gaza Strip border were invited to participate in the study. The request was made via social networks to fill research questionnaires accessed through an Internet link. A total of 124 participants exposed to ongoing rocket fire over the past 5 years voluntarily completed the research questionnaires. No compensation was offered for participation in the study.
The data analysis involved three stages. In the first stage, descriptive statistics, frequency distributions, and means and their standard deviations were examined, in order to analyze demographic variables and the study variables. In the second stage, Pearson product-correlation coefficients were calculated to identify correlations between study variables and PTSD symptoms (Table 1). In addition, Pearson tests were conducted to examine the relationship between the subscales of PTSD symptoms (intrusiveness, avoidance, negative changes and arousal). Since high correlations were found between different subscales (ranging from r = 0.58 to r = 0.87), statistical tests were examined in relation to the total scale of PSL. In the third stage, a hierarchical multiple regression was conducted to ascertain the relative contributions of demographic variables (education, early exposure to trauma, and economic status) and study variables (religiosity and spirituality) to the development of PTSD symptoms.
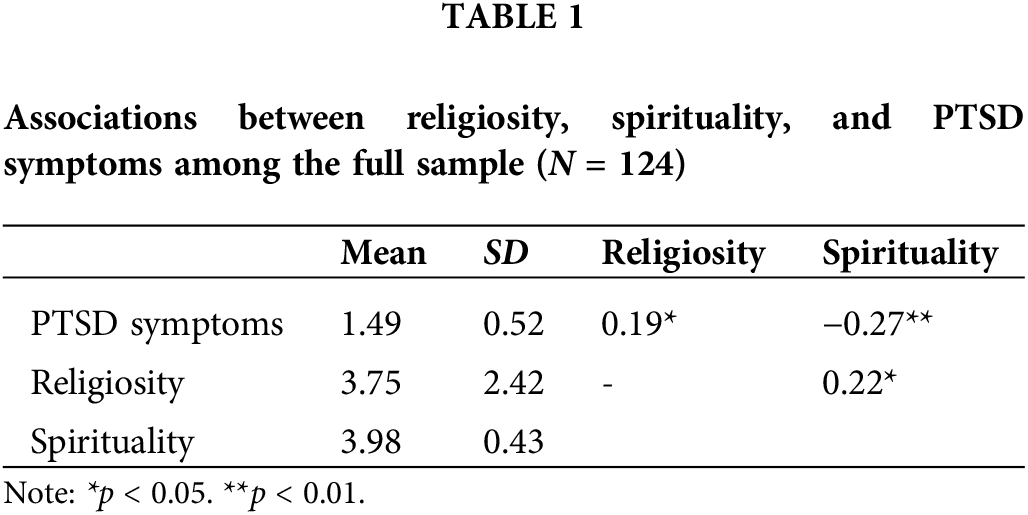
As demonstrated in Table 1, Pearson product-correlation coefficients for the total sample revealed a positive correlation between religiosity and PTSD symptoms (r = 0.19, p < 0.05); whereas a negative correlation was found between spirituality and PTSD symptoms (r = −0.27, p < 0.01).
To gain a better understanding of the study results, the total sample was also divided into two groups according to the way participants defined their relationship with their religion. The first group included participants who defined themselves as secular and the second group included participants who defined themselves as traditional or religious (hereafter religious; Table 2). Among the secular sub-group the mean of religiosity was 1.59 (SD-0.97), and the mean of spirituality was 3.88 (SD-0.39). Among the religious group the mean of religiosity was 5.91 (SD-1.16), and the mean of spirituality was 4.08 (SD-0.44). In addition, Independent samples T-Test was conducted in order to examine differences in PTSD symptoms between the two sub-groups, and no significant difference was found. Further examination of the two subgroups (i.e., religious and secular) revealed no correlation between religiosity and PTSD symptoms among the religious group; whereas among the secular group, there was a positive correlation between those variables (r = 0.42, p < 0.01). In addition, we added a scatter plot with fit line graphs presenting the correlations between religiosity and PTSD symptoms in both subgroups as well as individual observations (Fig. 1). In order to control possible bias of high scored out liners in PTSD symptoms scale as presented in Fig. 1, we examined the same data while removing PSL results that were higher than 3. Yet, positive correlations were still presented in the secular sub-group while no correlations were presented in the religious sub-group.
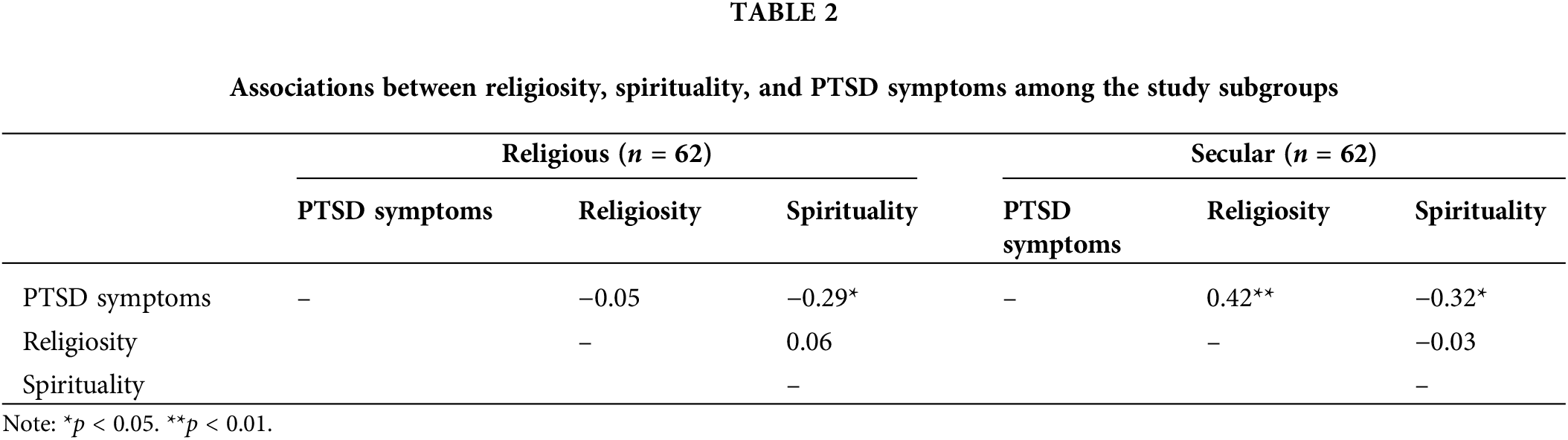
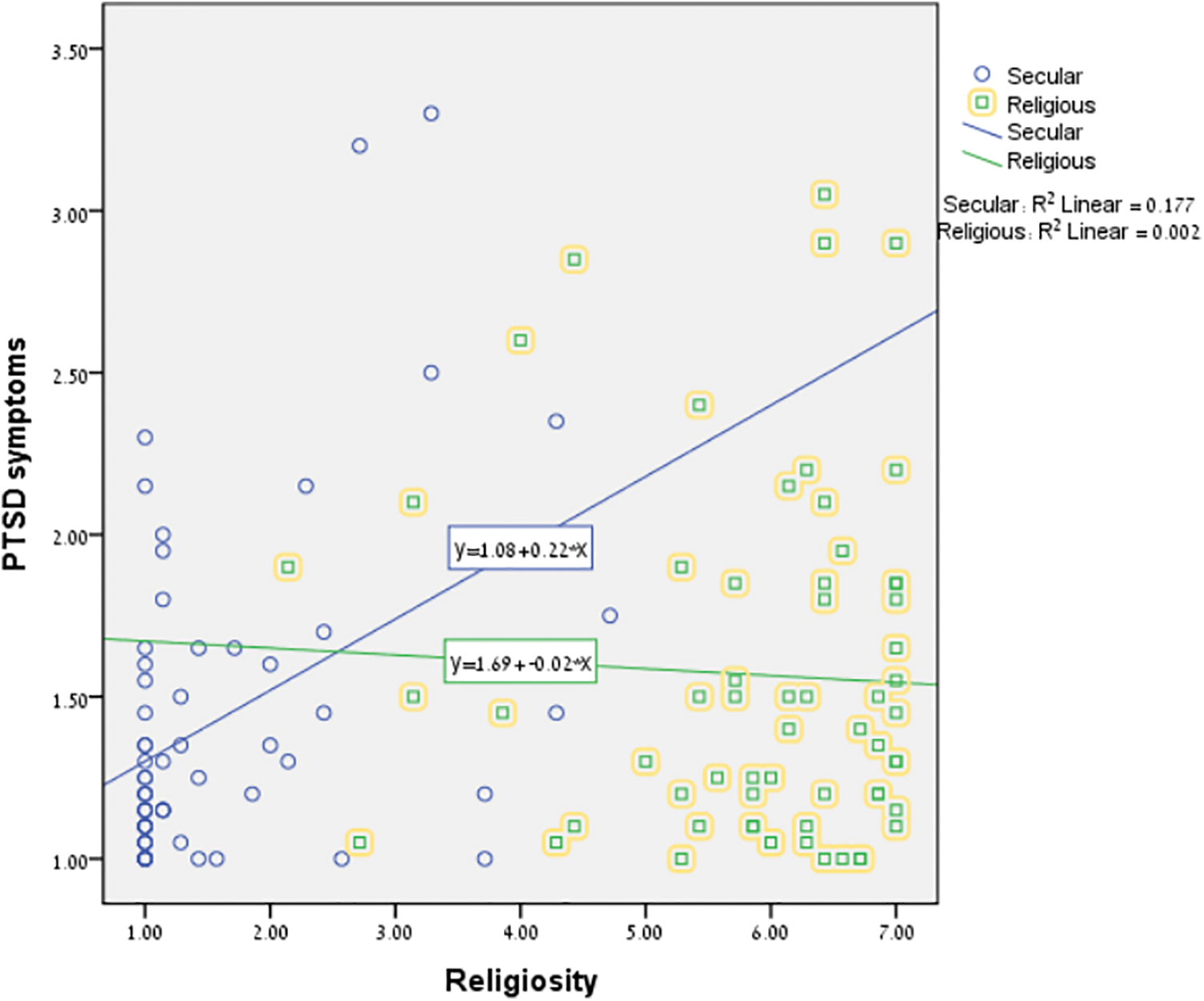
Figure 1: Scatter plot with fit line graphs presenting the correlations between religiosity and PTSD symptoms in both subgroups.
A hierarchical multiple regression was also conducted among the entire sample in order to ascertain the relative contributions of the demographic variables (Step 1: education, previous exposure to trauma, and economic status) and the study variables (Step 2: religiosity and spirituality) to the development of PTSD symptoms (as presented in Table 3). For the benefit of the analysis “Previous exposure to trauma” was defined as an interval variable with 2 values (1-Exposed to early trauma 2-Not exposed to early trauma).
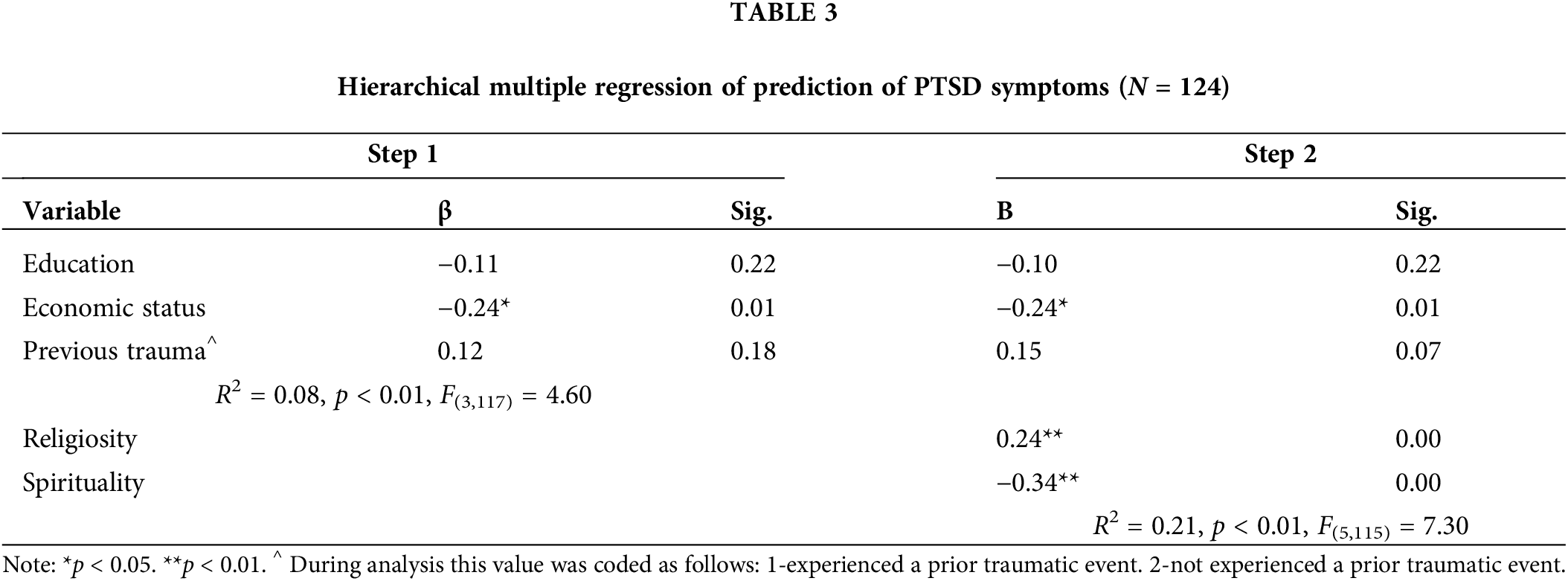
As shown in Table 3, in Step 1, the explained variance for PTSD symptoms was R2 = 0.08 (p < 0.01) and only economic status significantly contributed to the explained variance (β = −0.24, p < 0.05). In the second step, when the variables religiosity and spirituality were entered, the explained variance was R2 = 0.21 (p < 0.01). The variables that significantly contributed to the explained variance in Step 2 were economic status (β = −0.24, p < 0.01), religiosity (β = 0.24, p < 0.01), and spirituality (β = −0.34, p < 0.01).
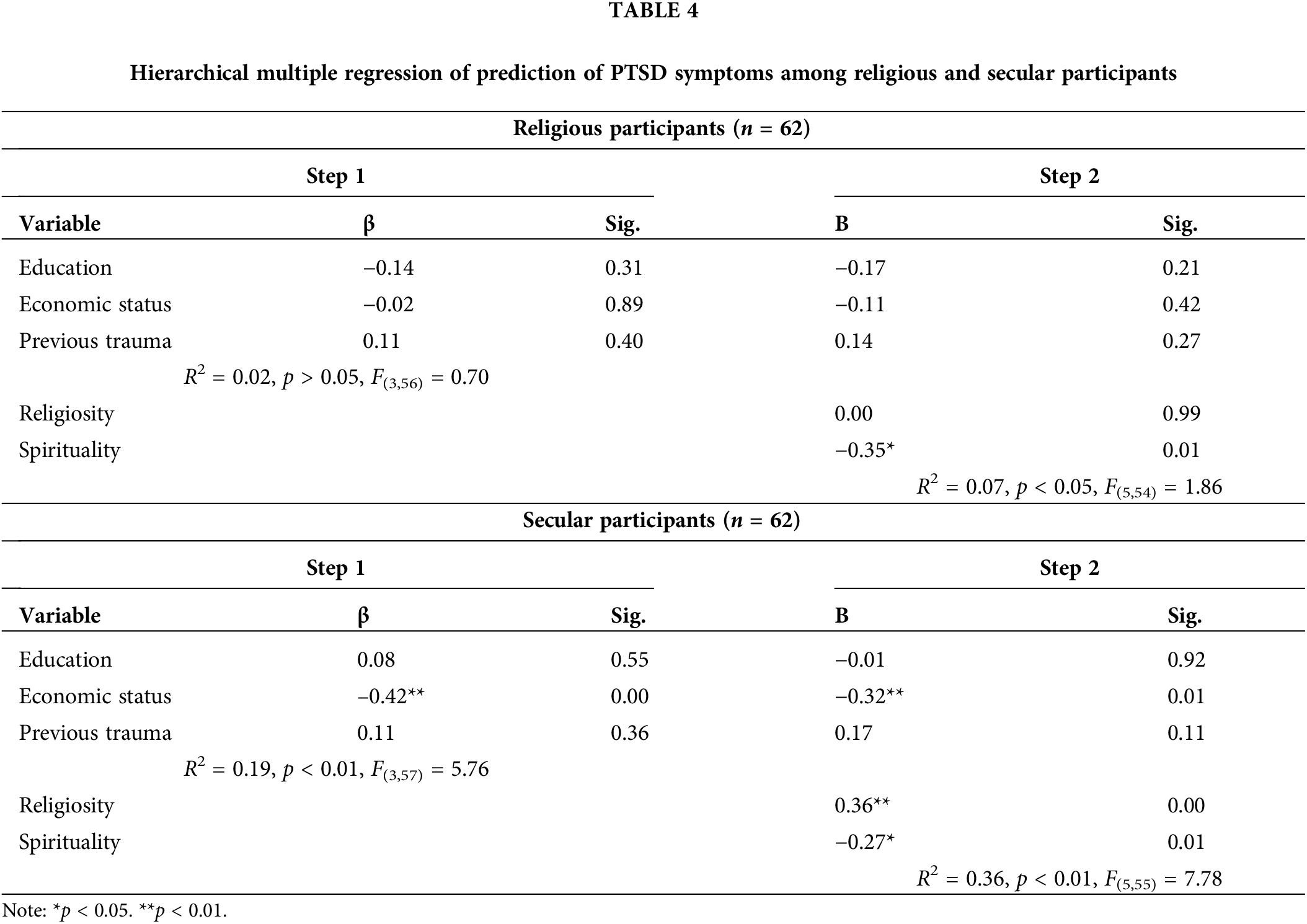
In addition, hierarchical multiple regressions were conducted within each of the two subgroups (Table 4). As shown in Table 4, among the religious group, Step 1 was not significant. In Step 2, the explained variance was R2 = 0.07 (p < 0.05) and only spirituality contributed to PTSD symptoms (β = −0.36, p < 0.05). In contrast, among the secular group, the explained variance in Step 1 was R2 = 0.19 (p < 0.01) and financial status contributed significantly to PTSD symptoms (β = −0.42, p < 0.01). In Step 2, the explained variance for PTSD symptoms was R2 = 0.36 (p < 0.01) and financial status (β = −0.32, p < 0.01), religiosity (β = 0.34, p < 0.01), and spirituality (β = −0.26, p < 0.05) were found to be significant for the development of PTSD symptoms.
Exposure to traumatic events and ongoing terror incidents are positively correlated throughout the literature with higher levels PTSD symptoms [1,3]. Within the research literature, religiosity [9] and spirituality [10,11] have been reported to be significant for the development of PTSD. However, studies have not yet examined the relationships between these variables and the development of PTSD symptoms among a civilian population continuously exposed to missiles and rocket fire. Therefore, the present study examined these relationships among Israelis living within 10 km the border of the Gaza Strip, who have been exposed to ongoing mortar fire and missile attacks in recent years.
Previous studies have documented a negative relationship between religiosity and PTSD symptoms, emphasizing the role of religiosity in coping with traumatic events [9]. However, surprisingly and contrary to our research hypothesis, we found a positive relationship between religiosity and PTSD symptoms. This discrepancy between our results and those of previous studies could be attributed to a potential link between religiosity and coping with trauma. According to Chen et al. [15], traumatic exposure may cause the development of PTSD and, at the same time, intensify individuals’ religious activities and the beliefs that they use to cope with PTSD symptoms. Thus, the observed positive relationship might indicate an attempt to cope with the traumatic experience through intensified religious activity. Moreover, different forms of negative religious coping strategies such as feeling that God acts in a careless manner accompanied by feelings of abandonment by God [24] or by one’s community of faith [22], and viewing the traumatic event as a divine punishment [25], might lead to high levels of PTSD symptoms [21,22,24]. Exposure to a traumatic event violates one’s inner sense of protection and following the experience that the world is a threatening and dangerous place [39]. It can be assumed that in dealing with ongoing trauma, the individual repeatedly experiences the trauma and evil in the world, and therefore may develop this kind of negative religious coping. As for the current study, it seems that the prolonged exposure to rocket fire may have been the cause of a negative religious form of coping and therefore of higher levels of PTSD symptoms.
Within the context of religiosity and trauma, research has often referred to a single traumatic event [e.g., 18] or traumatic events such as war among soldiers or veterans [e.g., 16,17]. However, the present study was conducted among civilians exposed to ongoing terrorist threats in a context that includes the routines of civilian life [1]. It may be that in cases of a single traumatic event or prolonged traumatic exposure within a war context, the individual understands that at the end of the event, that life will return to normal. Therefore, individuals may be able to use internal and external resources, including religiosity, to help them cope with the threat. In these cases, increased use of religiosity may indicate effective coping with the traumatic exposure. In contrast, as civilians deal with ongoing terrorist attacks over many years, they need to manage an emergency routine while trying to maintain normative daily life. Life under these circumstances includes an ongoing sense of threat, uncertainty, lack of control, vigilance for a possible renewed attack and the hope that these events will come to an end [4]. In such situations, the increased need to appeal to the religious resource, characterized by religious life changes including changes in religious practice and increased devotion, might conflict with the need to return to a normal life routine. According to Cohen-Louck et al. [40], citizens living under constant threat may resort to different types of coping. Thus, they offer 4 different types of coping-derived by combining 2 axes scores: high–low problem coping and high–low emotion coping. Their research findings indicate that an Adaptive Type of coping was the most effective facing ongoing terrorist attacks. This coping style consists of low levels of both Problem-focused and emotional focused styles. Cohen-Louck et al. argue that adaptive type perceives terrorism as part of a lifestyle routine rather than a crisis and therefore does not see a need to employ coping styles. In this sense, with regard to our findings, it seems that in situations of ongoing threat, an increased use of religiosity may indicate difficulty in coping with the ongoing threat and with the need to return to a normal course of life and may also indicate emotional distress, expressed by a higher rate of PTSD symptoms.
Moreover, it should be noted that the current study was conducted about a month after the escalation of violence in the region, as residents were trying to return to their regular routines. The results of this study might have been different had it been conducted during a period of escalated threat, as shown by previous studies [16,17]. Furthermore, although most of the research literature in this area has argued for the existence of a negative relationship between religiosity and PTSD, the positive relationship between these variables that was found in this study supports the findings of other studies that have reported a positive relationship between these variables and concluded that religiosity weakens mental resilience and increases the risk for developing PTSD after exposure to terrorist events [19,41].
Interestingly, among the religious participants, no correlation was found between religiosity and PTSD symptoms; whereas among the secular group, a positive correlation was observed and that correlation was stronger than the correlation observed among the entire sample. It is important to note that in Israeli culture, people who define themselves as secular may still have a religious affiliation, and sometimes even hold religious ceremonies and hold religious beliefs. In other words, it is hard to say whether a person is objectively ‘religious’ or non-religious in a binary form, but it is mainly about self-determination. However, there are changes between different individuals-religious and secular—in relation to their level of religiosity [35]. Many of the religious participants may have been accustomed from childhood to a religious lifestyle and belief in God, such that they did not relate to their religiosity as an internal coping resource. They may have maintained their religious activities out of habit or as their regular lifestyle, as opposed to having specifically turned to religiosity, in order to deal with the traumatic threat that had become part of their daily life. Therefore, among the religious group, possibly religiosity would not have served as an essential resource in dealing with the ongoing distress that is characteristic of life under the threat of rocket fire.
In contrast to religious individuals who do not experience major conflict between their religious lifestyle and their self-definition and social identity, for secular individuals, an affinity for religiosity is inconsistent with their self-definition as secular. Therefore, the referral to religious resources by these individuals may have been done for utilitarian reasons. According to Laufer et al. [9], individuals may engage in religiosity out of a desire to achieve social or personal goals such as mental well-being. However, the religion resource might not be a stable one and exposure to traumatic events may undermine it. Moreover, it could be assumed that religiosity lies on one’s belief in it, and that religiosity beliefs are a necessary condition for its benefits. There for, the religious resource might be less stable and less helpful for secular individuals in dealing with exposure to trauma as they consist of lower rates of religiosity beliefs. According to Hobfoll’s Conservation of Resources Theory [6,8], the loss of a resource can exacerbate PTSD symptoms. Therefore, the religious resource that has served individuals positively in the past may now begin, after exposure to a traumatic event, to undermine their mental resilience. For example, individuals might interpret the threat situation as a form of divine punishment for their sins.
In accordance with the second research hypothesis, a negative relationship was found between spirituality and PTSD. These findings reinforce previous research that has found spirituality to be associated with lower levels of PTSD symptoms and mental distress [31,34]. However, no previous studies have investigated the contribution of spirituality to the coping of a civilian population frequently exposed to missile and rocket threats. The findings of this study emphasize the importance of spirituality for effectively dealing with exposure to ongoing terrorist threat, as well as for efforts to attempt to maintain a normal life routine in this complex reality. In ongoing terror situations, the individual may suffer from feelings of meaninglessness and uncertainty, as well as various feelings of distress such as stress, tension, anxiety, sadness, despair, and depression [3,5]. Spirituality may help to moderate these negative feelings and promote positive emotions [32,42].
Many previous studies have referred to religiosity and spirituality as overlapping variables, without sufficiently distinguishing between them [13]. However, this study demonstrated the difference between these two factors, as a negative relationship was demonstrated between spirituality and PTSD symptoms, but not between religiosity and PTSD symptoms. Thus, these findings reinforce the idea that spirituality can be defined differently from religiosity and can represent a variety of positive human qualities and a sense of meaning and feelings of wholeness with oneself and one’s environment [27].
These research findings constitute a significant contribution to the understanding of spirituality and religiosity as internal resources that are significant for the well-being of individuals who have been exposed to trauma. These findings emphasize the unique importance of spirituality as an internal and accessible resource associated with reduced emotional distress and effective coping with prolonged exposure to rocket fire and missile attack. Therefore, when constructing intervention plans, we recommended that spirituality be considered an essential resource that may reduce negative feelings accompanying traumatic exposure, instil positive emotions, and deepen the sense of meaning when life is fraught with danger, threat, and turmoil. As for religiosity, it seems that this resource should be treated with caution when dealing with emotional distress, especially among secular individuals. The distinction made in this study between spirituality and religiosity and the differences found between the subgroups in this study (religious and secular) may shed light on the mixed findings in the research literature regarding the relationship between religiosity and PTSD symptoms [9,15], expand our understanding of these factors, and provide a basis for further investigation of the reciprocal relationship between them.
Several limitations of this study should be noted. The cross-sectional study design precludes conclusions regarding causal relationships. In addition, the unique nature of the sample and the relatively small sample size necessitate that caution be used when generalizing the findings. Nevertheless, despite these limitations, the findings of this study are of great importance especially when considering the fact that the study was conducted in close proximity to the escalation of violence in the region. This study may offer a significant contribution to models of intervention with residents living under ongoing terrorist threats, emphasizing the importance of spiritually and sensitivity to religion while coping with PTSD symptoms.
Acknowledgement: We thank the reviewers for their important feedback regarding this study.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: Jonathan Wolkinson and Michael Weinberg; data collection: Jonathan Wolkinson; analysis and interpretation of results: Jonathan Wolkinson and Michael Weinberg; draft manuscript preparation: Jonathan Wolkinson and Michael Weinberg. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data will be provided upon request to the corresponding author.
Ethics Approval: The study was approved by the University of Haifa Ethics Committee (408/18).
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Greene T, Itzhaky L, Bronstein I, Solomon Z. Psychopathology, risk, and resilience under exposure to continuous traumatic stress: a systematic review of studies among adults living in southern Israel. Traumatology [Internet]. 2018;24(2):83–103. [Google Scholar]
2. Meir Amit Intelligence and Terrorism Information Center. https://www.terrorism-info.org.il/en/. [Accessed 2021]. [Google Scholar]
3. Besser A, Neria Y. PTSD symptoms, satisfaction with life, and prejudicial attitudes toward the adversary among Israeli civilians exposed to ongoing missile attacks. J Trauma Stress [Internet]. 2009;22(4):268–75. [Google Scholar] [PubMed]
4. Lahad M, Leykin D. Ongoing exposure versus intense periodic exposure to military conflict and terror attacks in Israel. J Trauma Stress [Internet]. 2010;23(6):691–8. [Google Scholar] [PubMed]
5. Besser A, Priel B. Personality vulnerability, low social support, and maladaptive cognitive emotion regulation under ongoing exposure to terrorist attacks. J Soc Clin Psychol [Internet]. 2010;29(2):166–201. [Google Scholar]
6. Hobfoll SE. Social and psychological resources and adaptation. Rev Gen Psychol [Internet]. 2002;6(4):307–24. [Google Scholar]
7. Hobfoll SE. Conservation of resources: a new attempt at conceptualizing stress. Am Psychol [Internet]. 1989;44(3):513–24. [Google Scholar] [PubMed]
8. Hobfoll SE. The influence of culture, community, and the nested-self in the stress process: advancing conservation of resources theory. J Appl Psychol [Internet]. 2001;50(3):337–421. [Google Scholar]
9. Laufer A, Solomon Z. The role of religious orientations in youth’s posttraumatic symptoms after exposure to terror. J Relig Health [Internet]. 2011;50(3):687–99. [Google Scholar] [PubMed]
10. Bradley R, Schwartz AC, Kaslow NJ. Posttraumatic stress disorder symptoms among low income, African American women with a history of intimate partner violence and suicidal behaviors: self-esteem, social support and religious coping. J Trauma Stress [Internet]. 2005;18:685–96. [Google Scholar] [PubMed]
11. Watlington CG, Murphy CM. The roles of religion and spirituality among African American survivors of domestic violence. J Clin Psychol [Internet]. 2006;62(7):837–57. [Google Scholar] [PubMed]
12. Harris K, Howell D, Spurgeon D. Faith concepts in psychology: three 30-year definitional content analyses. Psychol Relig Spirit [Internet]. 2018;10(1):1–29. [Google Scholar]
13. Shaw A, Joseph S, Linley PA. Religion, spirituality, and posttraumatic growth: a systematic review. Ment Health Relig Cul [Internet]. 2005;8(1):1–11. [Google Scholar]
14. Hamren K, Chungkham HS, Hyde MR. Religion, spirituality, social support and quality of life: measurement and predictors CASP-12(v2) amongst older Ethiopians living in Addis Ababa. Aging Ment Health [Internet]. 2015;19(7):610–21. [Google Scholar] [PubMed]
15. Chen Y, Koenig H. Traumatic stress and religion: is there a relationship? A review of empirical findings. J Relig Health [Internet]. 2006;45(3):371–81. [Google Scholar]
16. Hasanović M, Pajević I. Religious moral beliefs inversely related to trauma experiences severity and presented posttraumatic stress disorder among Bosnia and Herzegovina war veterans. J Relig Health [Internet]. 2015;54(4):1403–15. [Google Scholar] [PubMed]
17. Sharma V, Marin DB, Koenig HK, Feder A, Iacoviello BM, Southwick SM, et al. Religion, spirituality, and mental health of U.S. military veterans: results from the national health and resilience in veterans study. J Affect Disorders [Internet]. 2017;217:197–204. [Google Scholar] [PubMed]
18. Bleich A, Gelkopf M, Solomon Z. Exposure to terrorism, stress-related mental health symptoms, and coping behaviors among a nationally representative sample in Israel. JAMA [Internet]. 2003;290(5):612–20. [Google Scholar] [PubMed]
19. Plante TM, Manuel GM. The Persian Gulf War: civilian war-related stress and the influence of age, religious faith, and war attitudes. J Clin Psychol [Internet]. 1992;48(2):178–82. [Google Scholar] [PubMed]
20. Bonanno GA, Jost JT. Conservative shift among high-exposure survivors of the September 11th terrorist attacks. Basic Appl Soc Psych [Internet]. 2006;28(4):311–23. [Google Scholar]
21. O’Brien B, Shrestha S, Stanley MA, Pargament KI, Cummings J, Kunik ME, et al. Positive and negative religious coping as predictors of distress among minority older adults. Int J Geriatr Psych [Internet]. 2019;34(1):54–9. [Google Scholar]
22. Pargament K, Feuille M, Burdzy D. The brief RCOPE: current psychometric status of a short measure of religious coping. Religions [Internet]. 2011;2(1):51–76. [Google Scholar]
23. Exline JJ. Religious and spiritual struggles. In: Pargament KK, Exline JJ, Jones JW, editors. APA handbook of psychology, religion, and spirituality [Internet]. vol. 1. Washington DC: American Psychological Associates; 2013. p. 459–75. [Google Scholar]
24. van Hook MP. Spirituality as a potential resource for coping with trauma. Social Work and Christianity [Internet]. 2016;43(1):7–25. [Google Scholar]
25. Blanc J, Rahill GJ, Laconi S, Mouchenik Y. Religious beliefs, PTSD, depression and resilience in survivors of the 2010 Haiti earthquake. J Affect Disorders [Internet]. 2016;190:697–703. [Google Scholar] [PubMed]
26. King M, Speck P, Thomas A. The effect of spiritual beliefs on outcome from illness. Soc Sci Med [Internet]. 1999;48(9):1291–9. [Google Scholar] [PubMed]
27. Dyson J, Cobb M, Forman D. The meaning of spirituality: a literature review. J Adv Nurs [Internet]. 1997;26(6):1183–8. [Google Scholar] [PubMed]
28. Carmassi C, Stratta P, Calderani E, Bertelloni C, Menichini M, Massimetti E, et al. Impact of mood spectrum spirituality and mysticism symptoms on suicidality in earthquake survivors with PTSD. J Relig Health [Internet]. 2016;55(2):641–9. [Google Scholar] [PubMed]
29. Burkhart L, Solari-Twadell A. Spirituality and religiousness: differentiating the diagnoses through a review of the nursing literature. Int J Nurs Termin Cl [Internet]. 2001;12(2):45–54. [Google Scholar]
30. Howden J. Development and psychometric characteristics of the spirituality assessment scale (Doctoral Dissertation). Texas Woman’s University: Denton, Texas; 1992. [Google Scholar]
31. Gill CS, Minton CAB, Myers JA. Spirituality and religiosity: factors affecting wellness among low-income, rural women. J Couns Dev [Internet]. 2010;88(3):293–302. [Google Scholar]
32. Langman L, Chung MC. The relationship between forgiveness, spirituality, traumatic guilt and posttraumatic stress disorder (PTSD) among people with addiction. Psychiat Quart [Internet]. 2013;84(1):11–26. [Google Scholar] [PubMed]
33. Kennedy JE, Davis RC, Taylor BG. Changes in spirituality and well-being among victims of sexual assault. J Sci Stud [Internet]. 1998;37(2):322–8. [Google Scholar]
34. Briggs MK, Apple KJ, Aydlett AE. Spirituality and the events of September 11: a preliminary study. Couns Values [Internet]. 2004;48(3):174–82. [Google Scholar]
35. Troen I. Secular judaism in Israel. Society [Internet]. 2016;53(2):153–62. [Google Scholar]
36. Falach A. Emuna be’gilgul neshamot, datiut oopachad mipney mavet ishi [Belief in reincarnation, religiosity and fear of personal death] (MA Thesis). University of Haifa: Israel; 2001. [Google Scholar]
37. Ben-Meir Y, Kedem-Friedrich P. Madad datiut avoor hauchloosia b’Israel [Index of religiosity for the Jewish population in Israel]. Megamot: Rivon Lemadaei Hahitnahagut [Internet]. 1979;24:353–62. [Google Scholar]
38. Gil S, Weinberg M, Or-Chen K, Harel H. Risk factors for DSM 5 PTSD symptoms in Israeli civilians during the Gaza war. Brain Behav [Internet]. 2015;5(4):1–9. [Google Scholar]
39. Jannof-Bulman R. Shattered assumptions: towards a new psychology of trauma [Internet]. New York: Free Press; 2010. [Google Scholar]
40. Cohen-Louck K, Ben-David S. Coping with terrorism: coping types and effectiveness. Int J Stress Manage [Internet]. 2017;24(1):1–17. [Google Scholar]
41. Martz E. Death anxiety as a predictor of posttraumatic stress levels among individuals with spinal cord injuries. Death Stud [Internet]. 2004;28(1):1–17. [Google Scholar] [PubMed]
42. Wills E. Spirituality and subjective well-being: evidence for a new domain in the personal well-being index. J Happiness Stud [Internet]. 2009;10(1):49–69. [Google Scholar]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools