
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Workplace Wellness, Mental Health Literacy, and Usage Intention of E-Mental Health amongst Digital Workers during the COVID-19 Pandemic
1
Faculty of Creative Multimedia, Multimedia University, Cyberjaya, 63000, Malaysia
2
Faculty of Applied Communication, Multimedia University, Cyberjaya, 63000, Malaysia
3
International Medical University (IMU), Bukit Jalil, 57000, Malaysia
* Corresponding Author: Ah-Choo Koo. Email:
International Journal of Mental Health Promotion 2023, 25(1), 99-126. https://doi.org/10.32604/ijmhp.2022.025004
Received 17 June 2022; Accepted 19 August 2022; Issue published 29 November 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
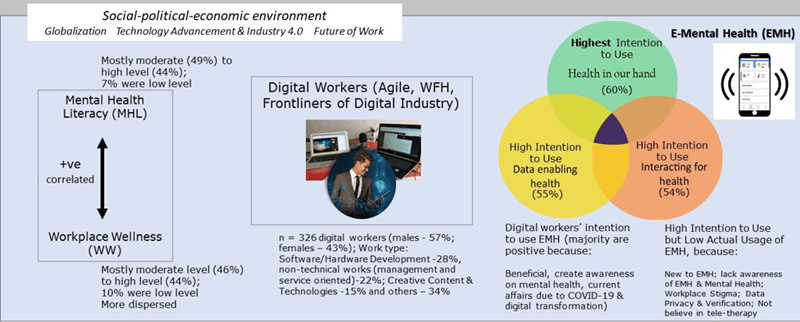
The prevalence of mental health problems in both Malaysian and global workplaces has significantly increased due to the presence of the coronavirus disease (COVID-19) pandemic, globalization, technology advancement in Industry 4.0, and other contributing factors. The pervasiveness of the issue poses a huge challenge to improving the occupational safety and health (OSH) of workers in various industries, especially in the digital industry. The emergence of the innovative industry is evident mainly due to the rapid development of Industry 4.0 and the relevant demands of multiple businesses in the digital transformation. Nonetheless, limited studies and academic discussions were conducted on the OSH topic of digital employees. Hence, the current study serves to fill the existing gap and provide academic contributions by scrutinising the perceptions of digital workers regarding their workplace well-being, mental health literacy, and the impression of employing e-mental health. The objectives of this study are: 1) To examine the mental health literacy and workplace wellness of digital workers, 2) to explore the emental health usage intention and actual e-mental health utilization, and 3) to identify digital workers’ feedback on e-mental health. In the current context, e-mental health focuses on three dimensions, namely, 1) “health in our hand (HIOH)”, 2) “interacting for health (IFH)”, and 3) “data enabling health (DEH)”. The present study employed an online cross-sectional survey and received 326 digital workers’ completed responses. Variables, such as “mental health literacy (MHL)”, “workplace wellness (WW)”, and e-mental health intention and usage were explicated by analysing the data through descriptive statistics. The study results indicated a moderate to a high level of the MHL and the WW. More than half of the workers possessed a high intention level to employ e-mental health, with the HIOH dimension being the most prevalent domain. Nevertheless, the actual e-mental health usage was very low, owing to the online resources being a new concept amongst digital employees. Numerous confounding factors also existed in affecting the low usage, such as privacy concerns, data security levels, and health verification issues. In addition, the mental health issue has not been openly and widely discussed in Malaysian workplaces due to stigmatisation. As such, the current findings could provide additional insights into the OSH literature; it could serve as a guideline for the OSH decision-makers, employers, and eHealth developers when establishing a feasible framework for the practical adoption of e-mental health services by digital workers.Graphic Abstract
Keywords
The current study focused on exploring e-mental health usage intention and actual utilization, workplace wellness, and mental health literacy amongst digital workers, particularly during the coronavirus disease (COVID-19) pandemic in Malaysia. The traditional mental health service system is encountering multiple challenges in delivering pertinent care to individuals in need due to the stigma surrounding mental illness and the prevalence of the negative perception in developing countries, including Malaysia. Resultantly, numerous individuals with mental health difficulties embrace their hardships in silence without seeking external support and avoid beneficial treatments [1].
Past studies demonstrated that, even if Malaysian employees increased personal awareness of available mental health resources, the workers would remain reluctant to receive succour, mainly due to poor mental health literacy [2]. Other barriers preventing individuals from gaining access to required treatment included financial, attitudinal, and geographical factors, such as low accessibility to isolated populations and a lack of resources to consult with healthcare practitioners [2]. Furthermore, the COVID-19 pandemic has aggravated mental health issues and negatively affected employee well-being worldwide. In Malaysia specifically, the enforcement of multiple movement control orders (MCOs) restricted the established operations of enterprises, workers, and public activities, thus negatively impacting the mental health of both workers and the general population, while generating various concerns and discussions in the occupational safety and health (OSH) field.
1.1 Research Background and the OSH Development
The recent emphasis on the OSH work was concerning the protection of workers’ wellness during and after the COVID-19 pandemic, as well as other challenges, such as natural disasters, social or political disruptions, and the unanticipated ramifications of technological advancement in Industry 4.0, including artificial intelligence (AI) and robotic technology, on employee safety, health, and wellness overall [3,4]. Correspondingly, an evidence-based systems model was proposed to illustrate the relative impacts of intertwining contextual forces in the social-political-economic environment during the COVID-19 pandemic on the future of work amongst enterprises and workers from the OSH perspective (refer to Fig. 1; [3]). The model delineated multilevel factors affecting enterprises and their workers’ well-being, resilience, and productivity by adapting the works of Sorenson et al. [5] to account for the effects produced by the COVID-19 pandemic. The systems-level model was a holistic guide for diverse parties or stakeholders to develop effective strategies for enhancing workplace wellness, which, according to the authors, approaches and strategies derived from this model can modify the needs of workers in different industries and countries.

Figure 1: The evidence-based systems model illustrating the complexity of various contextual forces in the OSH Field, such as the COVID-19 Pandemic and the Social-Political-Economic Environment [3] *Reprinted with permission from Elsevier for the work by Peters et al. (p. e189) [3]
A collective appeal has been announced by the Centers for Disease Control and Prevention (CDC) and the National Institute for Occupational Safety and Health (NIOSH) in the United States of America (USA) to increase the number of relevant research works and discussions concerning the future of work. Correspondingly, the CDC and NIOSH proposed an integrated framework, which consisted of pertinent topics and sub-topics for the “Future of Work” initiative [4]. The initiatives include “to compile existing studies on the future of work, to promote research amongst new industries, technologies, organizational designs, job arrangements, risk profiles, and ways to control risks, and to connect trends in workplace, work, and workforce changes to prepare for future workers’ safety, health, and well-being” [4]. Concurrently, the initiative background arose from various emergencies, such as disasters, the pandemic, abrupt alterations from globalization, and social disruptions, which significantly affected workplaces, work, the workforce, and the OSH. As such, the integrated framework could provide a versatile and multidisciplinary approach to positively confront the complexity of the future of work by incorporating the following key topics suggested in CDC/NIOSH Future of Work Initiative Priority Topics (p. 1066–1067), namely 1) the future of the workplace (organizational design, technological job displacement, work arrangement), 2) the future of work (AI, robotics, technologies), and 3) the future of the workforce (demographics, economic security, skills)”, with other respective sub-topics [6].
The OSH researchers are simultaneously urged to comprehend the significant implications of future work scenarios and translate effective interventions and measures in safeguarding workers’ safety, health, and well-being [4]. In Malaysia, the Safety and Health Policy established by the NIOSH of the Ministry of Human Resources Malaysia (2018) is committed to “ensure a safe and healthy working environment to all employees and others involved in or affected by its operation taking into account statutory requirements and relevant national and international standards and codes of practices”, and the OSH-related matters will be provided similar emphasis with other major business objectives to guide employers [6]. Accordingly, initiatives are present to be implemented by an employer to foster employee well-being [7]. The development of appropriate policies and practices in enterprises or organizations could also further employers’ business interests and operations by providing adequate paid leave, supporting workers for returning to work (post-injury), good management of disabilities, and the opportunity of earning higher remunerations. The benefits of employee wellness programmes which could be promoted and executed at both public and private institutions, regardless of the size of the company or organization [7].
1.2 The Emergence of Digital Industry and Mental Health Issues
The acceleration of technological development and advancement has created uncertainty and disruption in various workplaces and commercial operations, especially in the digital industry. The digital industry refers to “the integration of digital technology across businesses to support digital transformation; and this adoption of technology results in a fundamental change to the organization and the way they operate” [8]. The term “digital” mainly alludes to a greater focus on emerging technologies, such as cloud computing, big data analytics, machine learning, and mobile devices and apps [8]. Nonetheless, the technologically advanced era has engendered unique challenges for employee well-being and health, which created a research gap in the OSH field [9]. Therefore, relevant research works are required to investigate the impacts of the innovative work environment on distinctive psychological factors of workers [9].
Technology adoption could support the OSH initiative, in which pertinent studies were conducted to discover beneficial approaches to safeguarding employee mental health with technology, resultantly propounding different technological innovations to support mental health [10–13]. The past findings demonstrated a promising application aspect, albeit e-mental health studies, especially advanced technology utilization, were generally considered in the infancy stage [4]. Amongst the technology applications regularly employed in promoting e-mental health, the popular selections included mobile devices, smart wearables, virtual reality (VR), teleconferencing systems, and the AI implementation for mental health solutions. Accordingly, eHealth solutions were expounded in three dimensions in terms of e-mental health applications and innovation [14], concurrent with the current study methodology. E-mental health would be beneficial in sustaining the digital workers’ wellness due to the unique ability to provide high accessibility levels to individuals or groups where physical resources provided by the current healthcare system were difficult to acquire [3]. Hence, e-mental health, via the collaboration of various digital technologies, possesses the potential to bridge the accessibility gap by allowing mental health services to be highly attainable by underprivileged individuals [3].
1.3 Research Questions and Research Objectives
The present study sought to fulfill the research inquiries:
1. While the COVID-19 pandemic has accelerated the digital industry and digital economy, how do digital workers manage their wellness?
2. Do their mental health literacy influence digital workers’ wellness?
3. How are digital employees’ acceptance, usage, and feedback towards e-mental health?
By answering the research questions, the current study anticipated providing empirical evidence of digital workers’ wellness status and personal perceptions of e-mental health utility for personal health advantage. Meanwhile, the study findings would be discussed under the COVID-19 pandemic context amongst digital workers, especially in a developing country, such as Malaysia. Correspondingly, three specific objectives to guide the research are as follows:
1) To examine the “mental health literacy (MHL)” and “workplace wellness (WW)” of digital workers during the COVID-19 pandemic.
2) To explore the “intention to use e-mental health (ITU-EMH)” and “usage of e-mental health (UO-EMH)”.
3) To identify digital employees’ feedback on the EMH.
The following section, Section 2, concentrates on a literature review of mental health challenges in the workplaces of healthcare workers and digital workers during the pandemic. Particularly, the background of contemporary workforces in the digital industry and Industry 4.0 and the COVID-19 pandemic impacts on digital workers and mental health were perused. Section 2 also focuses on digital workers’ usage intention and the actual EMH employment with a relevant exposition on the influence of workplace change characteristics, such as the increasing agility demand, on employee wellness. Moreover, several contextual scenarios of Malaysian workers were reviewed before presenting the respective EMH solution domains after analyzing specific acceptance types of EMH solutions by digital workers. Meanwhile, Section 3 portrays the study methodology, while Section 4 reports the study results with detailed discussions to fulfil the research objectives. Subsequently, Section 5 elucidates the overall discourses of the findings by referring to previous related studies investigating workplace wellness and the EMH. Ultimately, Section 6 summarizes the discussions by concluding the key study implications with future recommendations in the OSH field.
Healthcare workers, who are simultaneously front liners in combating the COVID-19 pandemic, have been directly and significantly impacted psychologically by COVID-19 [15]. Numerous academicians had appealed for enhanced efforts in protecting and prioritizing the healthcare workforce’s mental health and well-being and of other worker groups who were the front liners during the COVID-19 pandemic. The escalating mental and psychological stress in health workers would negatively impact healthcare providers’ professionalism, care delivery quality, work efficiency, and overall life quality [15]. As such, the importance of health literacy measures to counteract workplace challenges should be supported and provided to the relevant workers as public health emergency measures in the form of self-care strategies, evidence-based interventions, and organizational approaches to improve existing policies by healthcare leaders and health systems [15].
2.1 Industry 4.0 and Digital Workers’ Mental Health
Industry 4.0, or I4.0, involves the digital transformation of the entire industrial and consumer markets, ranging from smart manufacturing to the convergence between various industries, businesses, and other processes [16]. The revolution primarily describes information technology-driven changes from smart manufacturing to digitizing entire value delivery channels, which would affect every essence of human experience in various sectors [17]. Advanced digitalization within factories, combining internet technologies and future-oriented technologies in “smart” products, has resulted in a new fundamental paradigm shift in efficient and effective industrial production [16,18].
Digital transformation has led the Malaysian workforce to be at the vanguard of introducing the national level policy regarding the I4.0 [19] and other initiatives, such as the Malaysia Digital spearheaded by the Malaysia Digital Economy Corporation (MDEC) in 2021. The recent rebranding of the Malaysia Multimedia Super Corridor (MSC) initiative launched 25 years ago to Malaysia Digital had witnessed the latest alterations to a digital economy with the creation of the digital industry. The MDEC is the agency leading the Malaysia Digital initiatives and developing the digital industry at both regional and national levels, in which the initiatives are complementing the contemporary demands of the mutually reinforcing I4.0 and digital economy [20]. Notwithstanding an abundance of national strategies which have been introduced in Malaysia, the well-being of the talents or employees who are the vanguards of the digital economy is scarcely examined.
In the I4.0 development, digital workers’, or the I4.0 pioneers’, mental health and well-being should thoroughly be inspected [21]. Nevertheless, “the impacts of the introduction of I4.0 related technologies on occupational health and safety (OSH) are uncertain” [9]. Correspondingly, the metamorphosis engendered by the I4.0 would be pertinent to integrating modern computational and sensory technologies, such as the internet of things, temperature sensors, and smart wearables. into the physical world in communicating information and applying other digital systems related to health and well-being [22]. Thus, a systematic review of 59 eligible studies was administered by employing the PRISMA model to include manuscripts related to the discussion of the relationships between the I4.0 and the OHS. Subsequently, a qualitative analysis of the 59 documents was conducted regarding the I4.0 technological applications specified by Zorzenon et al. [9], such as “Artificial Intelligence (AI), additive manufacturing, augmented reality, big data, cloud computing, cyber-physical systems, digital twin, internet of things, robotics, simulation, and virtual reality”. The I4.0 itself is defined by “the joint and combined incorporation of diverse technologies” [22].
Meanwhile, the negative aspect of the I4.0 technologies reported by Zorzenon et al. [9] includes increased psychosocial risks, elevated tension, frequent mental fatigue, reduced surveillance due to increased reliance on smart devices, sedentarism, overwork owing to increased task complexity, greater work demands, and physical complications, such as risks of electric shock; risk in the intimate robotic interactions, and risks of cyber-attacks.
Different types of health strains due to the digital transformation and the I4.0 technology application were also discovered [9]. For instance, adopting technology innovations would render related disruptions to a business environment by introducing unfamiliar risks to workers of an organization, wherein the work from home (WFH) approach generated unprecedented health risks, such as a sedentary lifestyle and unclear boundaries of work-life balance. Besides, gig workers, characterized by short-term contracts or freelance work with tight deadlines in the intensive labor market, would be highly exposed to job insecurity, which directly escalated the workers’ mental health distress [7]. Furthermore, the demand for workers’ agility in task completion was elevating, which posed certain challenges, including “promoting temporal and spatial flexibility, integrating resources, engaging in innovative activity, and utilizing communication and digital technology” [23]. Accordingly, employee well-being was the main research scope of future studies, as employees were the major pillars of industrial development in the I4.0, while the work environment would significantly contribute to the I4.0 industrial advancement [9].
An interview of a total of 35 digital employees (15 ordinary workers & 20 decision-makers) from the ten selected companies to unveil the positive and negative effects on perceived well-being and perceived performance throughout the transition phases of “before”, “during”, and “after” the I4.0 implementation [21]. Accordingly, the negative impacts affecting employee well-being and performance were manifested to outweigh the benefits produced by the positive aspects of the 14.0 implementation [21]. The negative inclination was due to the incomplete development of innovative digital technologies which contained several flaws during the implementation phase, where technology uncertainty and unreliability would usually emerge. Hence, the ambiguous situation would lead to stressful events and scenarios experienced by digital workers. Apart from that, limited knowledge or training and poor work divisions which occurred during the I4.0 technology adaptation were also contributing factors to digital employee wellness [21]. Summarily, perceived employee well-being and performance were not significantly influenced in the “before” phase; however, the psychological indicators were exacerbated in the “during” phase, before eventually being improved in the “after” phase [21].
2.1.1 Agility Demand from Digital Workers during the Pandemic and Endemic Eras
The COVID-19 pandemic revolutionized various industries across the globe and accelerated digital transformation in multiple life aspects, in which numerous workplaces, particularly digital work-related offices, were compelled to shift to online mode. The transformation resulted in a greater number of Malaysian working adults, particularly digital workers employed in digital industries and involved in information and communications technology (ICT)-related work areas, being subject to the transition from working from offices (WFOs) to the WFH by depending on different digital services, technologies, and applications [24]. Nonetheless, technology-based companies, such as Google and Amazon, considered return-to-work plans for their employees in the endemic era, with a majority of digital workers adopting the hybrid work policy [25]. The hybrid approach was owing to most technology-based companies delivering digital works to clients, either internally or externally, which allowed flexible arrangements of returning to face-to-face work by considering the team goals, such as meetings or collaboration in groups, brainstorming, or community building [25]. In the current study, only human employees with digital skills and competencies were referred to as digital workers, while excluding automated solutions, such as software or robots which were programmed to perform specific tasks or processes in collaboration with human colleagues, in the research definition [26].
COVID-19 has and continues to change the work landscape. Many organizations reassessed their workforce capabilities and rapidly upskill and reskill their workers to perform in critical roles [27]. As such, digital literacy and skills have emerged as an important subset required from digital workers. 70% of the employees surveyed by the PricewaterhouseCoopers (PwC) expressed personal beliefs on the transformations engendered by the I4.0 technology on their current jobs in the short term (3–5 years), while 82% perceived the impact to be evident in the medium term (6–10 years), in which the skills gap became a pressing issue in various industries and necessitated constant learning in the ‘new normal’ workplaces. Accordingly, firm owners were concerned with employee readiness with the new norm of working patterns after recognizing the critical upskilling needs amongst their workers. Therefore, the survey conclusively demonstrated that the upskilling responsibilities were respectively contingent on workers themselves (49%) and business entities (31%) to ensure relevant employee value to the organizations and industries [27].
2.1.2 The WFH Policy Blurs the Work-Life Balance Boundary
The WFH policy provides the benefits of “Flexi-working hours” and “Flexi-working locations”. Nevertheless, certain drawbacks will exist if the policy is not optimally managed by digital workers, such as the blurring of work and personal life boundaries. Previous articles confirmed that the respective boundaries between work-related jobs, work-life balance, tasks, and personal chores were categorically defined [28,29]. Amongst 104 employees who responded to a survey conducted by Marimuthu et al. [28], 81 workers (78%) conveyed their high frustration and frequent sleep disturbance levels during the COVID-19 pandemic and the MCOs. The negative psychological impacts were owing to workplaces being teemed with demanding deadlines and high-performance delivery, which subject workers to constant stress and burnout risk. Burnout at work can be defined as exhaustion, it can be viewed as a clinical issue or as a management problem in dealing with the relationship of people with workplaces [30]. In a survey conducted by PwC [29], amongst 2003 employees, “only 28% can disconnect from work outside working hours, and only 25% say their employer helps them manage stress and focus on creating mental and emotional well-being. At the same time, only 22% are encouraged to take short breaks in the working day”. The vexatious condition resulted in the increased workload and working hours due to constant connectivity, which increased work pressure and a higher risk of developing other psychosocial problems [31]. Thus, promoting a healthier work-life balance and preventing burnout were encouraged to sustain employees’ higher performance degrees.
Digital workers’ well-being is imperative to be safeguarded, as the workers belong to the essential and talented workforce with critical skillsets for leading digital transformation. As reported in the AIA Vitality Healthiest Workplace Report 2019 [32], 51% of Malaysians encountered at least one type of work-related stress with an increment of approximately one per cent from the previous year, compared to the findings of the similar survey in 2018. Specifically, 53% of the digital workers slept less than seven hours a night, while 66% conducted less than 150 min of physical activities weekly (equivalent to less than 21 min per day) [32]. Consequently, Malaysia suffers from a high loss of productivity, with an annual RM2.7 million dissipation for health-related absenteeism and presenteeism per enterprise, or similarly, the Malaysian workforce squandered over 3 months or a cumulative of 73.1 working days per worker per year (7.7 days due to absenteeism and 65.4 days because of presenteeism) [32].
The deterioration of health while WFH was due to reduced physical exercise, a lack of communication with colleagues, increased intake of junk food, and being compelled to constantly provide care to children while at home. Additionally, WFH also caused higher distraction levels, which was strongly associated with poor mental health outcomes [28]. Specifically, around two-thirds of the respondents reported possessing at least one new physical health problem, and nearly three-quarters with at least one new mental health problem [33]. The statistics depicted alarming concerns for Malaysian workers’ health and well-being, which would result in a significant negative impact on organizational performance.
2.2 Malaysian Workers’ Mental Health Status
The COVID-19 pandemic has engendered numerous workers with increased job insecurity and challenges [34]. Contemporarily, 48,000 adults of their working age experienced mental diseases, as recorded by the Department of Social Welfare [35]. Malaysian adults are suffering from mental health depression with the national prevalence at 2.3% of the population or nearly half a million people [36]. Meanwhile, the report on Malaysian adolescents recorded a high frequency wherein the figures in 2018 manifested that 5.5 million adolescents aged between 13 and 17 years old were enduring melancholy to different degrees [37]. Particularly, depression, anxiety, and stress were the ubiquitous mental issues in which anxiety was at the highest indication, with two-fifths experiencing anxiety complications.
Amongst 694.4 thousand unemployed individuals reported in November 2021 [38], a segment of the total unemployed encountered financial issues and challenges due to the exorbitant living cost. Particularly, research evidence demonstrated that unfavourable financial factors contributed to increasing mental health problems of Malaysian generation Y, or Gen Y, in which a significant positive relationship between financial health (as opposed to social and physical health) and mental health was discovered from Gen Y [39]. Furthermore, stress could spring from fear, uncertainty, financial stress, and limited in-person interactions [40,41]. Subsequently, combined with compelled solitude in limited spaces due to the MCO implementation, restricted movement and contact precautions, indignation, confusion, a sense of hopelessness, the presence of anxiety symptoms, depression, and post-traumatic stress disorder would produce interacting effects negatively on individuals situated in mandated home quarantine for a long duration. Other reasons, such as risk perception and insufficient information during quarantine, could also lead to distress, frustration, and apprehension [40,41].
2.3 The EMH and Respective Domains
Digital technology has generated significant reverberations in healthcare, self-management, contact tracing, infection data management, and other relevant areas, particularly during the COVID-19 pandemic, where digital health or eHealth received surging attention in the areas of education, communication, and patient management [42]. The central foundation of this change will be the development and implementation of new ways of remote and digital health working [42]. The e-mental health (EMH) refers to “the use of the Internet and related technologies to deliver or enhance mental health information and services” [43]. It possesses the potential to bridge the gaps present in traditional mental healthcare systems. Moreover, the EMH assisted by various digital technologies could provide enhanced treatment access to geographically secluded populations, preserve anonymity when receiving treatment by individuals who perceive a strong stigma with mental health therapy, and reduce medical expenditures in terms of operating costs while reaching many patients simultaneously [44].
According to Lal [43], the EMH solutions could be categorised into various purposes, such as providing mental health-related information, mental health screening, self-assessment and monitoring, and community or peer support. A meta-analysis was conducted by Fu et al. [45] on young adults from low-income and middle-income countries between 20 and 35 years old who experienced depression or substance misuse. By comparing a total of 2,351 participants who received a digital psychological intervention with 1,753 counterparts in the control group, the researchers revealed that “digital psychological interventions are moderately effective when compared with control interventions” [45]. Hence, the EMH could enhance accessibility and capability to regulate personal health by enabling virtual communication between physicians and clients and combining data analysis results to produce insights for better diagnosis [12]. Correspondingly, the COVID-19 pandemic created unique opportunities for web and app-based digital mental health interventions (DMHIs) to target pandemic-related distress [12]. A review conducted by Lattie et al. [12] on digital mental health highlighted technological utility in boosting access to care by gingerly considering the design and implementation of digital mental health solutions to maximise the effectiveness and accessibility to users.
A systematic literature review paper by Goetz et al. [11] stated that the EMH applied more advanced technology, such as the AI and machine learning, to extract insights from self-reported data related to physiological biomarkers, including electroencephalogram (EEG). The EEG was extensively administered due to high accuracy, portability, and cost-effectiveness. The six industrial domains or sectors involved in the review included 1) health services with pertinent data analysis of clinical data, 2) the construction sector, 3) transportation industry, 4) the mining industry, 5) public services, and 6) general working environment towards stress management. Nonetheless, the authors (p. 9) suggested that “there are still many gaps to be filled with other sectors of the industry” and reiterated that future studies could consider incorporating industry sectors and working conditions. Meanwhile, certain researchers preferred to employ the electrocardiogram (ECG) and galvanic skin response (GSR) to predict emotional states, as the ECG precisely registered the heart rate (HR) and heart rate variability (HRV). Furthermore, pupillary response (PR), a physiological response based on pupil diameter, could be also referred to in gauging patients’ psychological conditions [11].
To quote from Shaw et al. [14], “eHealth is defined as the usage of digital technologies to monitor, track, and inform; the use of digital technologies to facilitate communicative encounters between health stakeholders; and the use of data to improve health and health services”. Past researchers performed several thematic analysis interviews with health care research experts and revealed an eHealth model with three general domains, namely, 1) “Health in our hands is the use of technologies to monitor, track, and inform health status”; 2) “Interacting for health involves the use of technologies to communicate between stakeholders in health”; 3) “Data enabling health is the use of technology to collect, manage, and use health data for a more precise diagnostic” (refer to Fig. 2) [14]. The development of the EMH model in the present study was guided by the eHealth model which integrated the expounded three domains, with the central overlap of the three domains indicating the optimal point of EMH with the greatest impact potential in promoting mental wellness. As suggested by Shaw et al. [14], the eHealth model could serve to guide the establishment of highly impactful eHealth innovations, as every eHealth intervention was recommended to encompass the three domains to be the most beneficial. The EMH model employed in the current study is illustrated in Fig. 2. The three domains were respectively applied to operationalise the EMH dimensions in the present study questionnaire. The EMH examples delineated in Fig. 1 were conveyed to the respondents to further probe personal notions and usage intentions of available digital mental health services and products offered.

Figure 2: The EMH model adapted from the domains proposed by Shaw et al. [14]
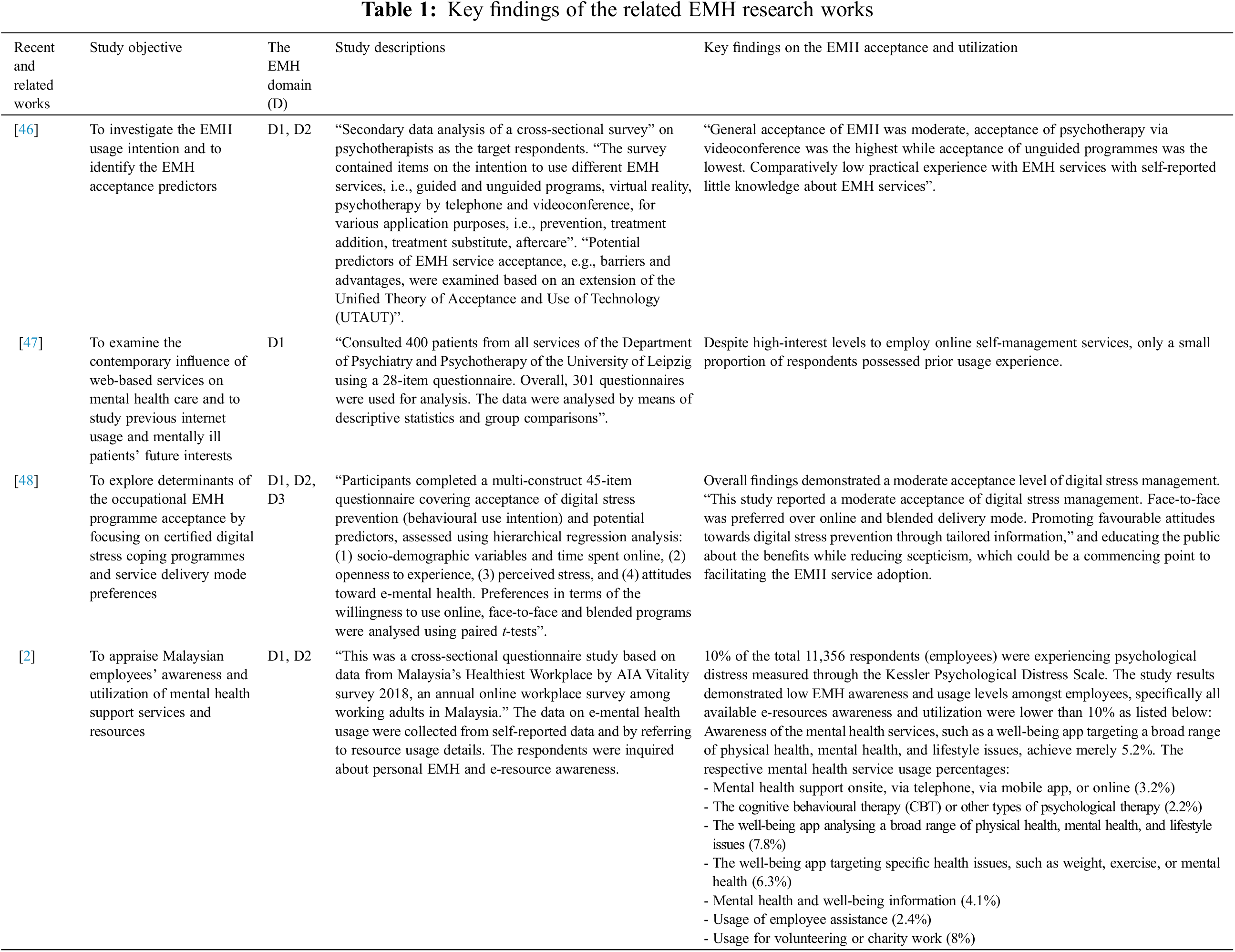
The EMH research was gaining traction in recent years where more advanced technology was applied as per the domain developed by Shaw et al. [14]. The current section reviewed relevant studies revealing a similar finding on the contrast between a higher acceptance but low prior experience of the EMH utilization (refer to Table 1). The literature review justified and provided an understanding of the current findings by providing scientific evidence of the EMH acceptance, in which a low to moderate EMH acceptance was generally discovered. As detailed in Table 1, the EMH domains explored in the present study were commonly Domain 1 (D1) and Domain 2 (D2). Nevertheless, an increasing interest in Domain 3 (D3) to develop applicable EMH solutions and enhance acceptance levels was also discovered from the manifested trends reported in review studies [9,11]. In addition, the comprehensive review of past findings assisted in identifying the determinants of the EMH acceptance and utilization, which were essential for more sustainable and prolonged EMH adoption in the future, as explored in the sections Results and Discussions.
2.5 The EMH Usage Intention as a Behavioural Construct
Feasibility was discovered to possess an indirect positive influence on the EMH utilization intention, thus positing a significant link between favourable EMH attitudes and imperative mental support in alleviating work stress [49]. Particularly, employees with previous records of sickness absence (higher risk of early retirement) would contain a low favourability attitude towards the EMH (11%), hence necessitating a prerequisite education, including promotion of the EMH awareness [49]. Workers were encouraged to be highly aware of the EMH tools by possessing relevant usage knowledge and self-confidence in the features and security before practically utilising the apparatuses, as a higher eHealth acceptance level was correlated with a higher eHealth knowledge level [14,50]. Meanwhile, the MHL scarcity was highlighted as a major impediment to mentally ill individuals seeking pertinent care. Conversely, increased awareness of mental health issues and discussions would urge employees to disclose personal mental health. Acceptance levels of stress-management applications could also be influenced by the severity degrees of stress symptoms [51]. Nonetheless, no conclusive evidence was revealed to significantly link the relationship between stress and the EMH acceptability [48], owing to the diverse cultural aspects of the targeted users.
The current study employed a cross-sectional survey to assess the mental health of digital workers from different Malaysian ICT organizations. The digital employees were purposively selected due to their high involvement levels with digital technologies in performing daily tasks and the possession of relevant experience, background, and technical knowledge in the ICT areas. The respondents were mainly recruited from the alumni of the eleven Malaysian Premier Digital Technology Institutions (PDTIs), where digital workers could be feasibly recruited to participate in the present study. Besides, the study was conducted by gathering data from the target respondents via a Google Forms questionnaire. The questionnaire was disseminated via various online communication channels, such as email, WhatsApp, and Facebook Messenger, due to the MCO implementation during the data collection stage, which was conducted from March to July 2021. Amongst 390 responses collected, only 326 responses were valid (due to their completeness) for subsequent analysis.
The employed questionnaire consisted of questions related to respondent demographics, items related to the MHL, the WW, the ITU-EMH, and open-ended feedback on the EMH. The MHL items were adapted from the eHealth Literacy Scale (eHEALS) [49], which comprised five questions measured on a five-point Likert scale, ranging from “Strongly disagree” (1) to “Strongly agree” (5). Meanwhile, the WW items were adapted from the five-item of World Health Organization (WHO) Well-Being Questionnaire and the Utrecht Work Engagement Scale (UWES) [52], which contained five questions assessed on a seven-point Likert scale, ranging from “At no time” (0) to “All of the time” (6). The ITU-EMH items, adapted from the unified theory of acceptance and use of technology (UTAUT) [53], measured respondents’ utilization intention through the three EMH domains, which consisted of nine questions appraised on a five-point Likert scale, ranging from “Strongly disagree” (1) to “Strongly agree” (5). The three EMH domains respectively comprised three questions each examining the usage intention in terms of “ITU-health in our hands” (ITU-HIOH), “ITU-interacting for health” (ITU-IFH), and “ITU-data enabling health” (ITU-DEH). Concurrently, 13 questions measured the usage of the EMH (UO-EMH) on a five-point Likert scale ranging from “Never” (0) to “Always” (4). The above items employed in the present study were included in Appendix A.
All questionnaire items were tested for face and content validity by six reviewers, namely three psychology practitioners, two psychology lecturers, and one experienced social science researcher. A pilot study was ensuingly conducted in an information and communication technology and multimedia-based university, which comprised two campuses with a total population of approximately 14,000 staff and students. The online questionnaire was distributed via email to 70 academicians and technical staff with more than five years of working experience. The staff were primarily managing and educating the undergraduates of both campuses of information technology, creative multimedia, and engineering-based faculties. The final number of collected responses was from 41 staff participating in the pilot study, which demonstrated an acceptable reliability level for all variables of the employed questionnaire items. Simultaneously, several language issues were resolved and improved based on the experts’ reviews.
The study results were delineated in three sections. Section 4.1 presents digital employees’ demographic characteristics and background information regarding personal job types, including work experiences, job scopes, and job roles, in the digital industry. Section 4.2 depicts the MHL and WW statuses of the digital industry. Meanwhile, Section 4.3 describes the ITU-EMH and the UO-EMH, whereas Section 4.4 portrays the summarisation of digital workers’ perspectives as garnered from their open feedback on the EMH. The SPSS version 23 was administered to generate descriptive statistics representing digital workers’ demographics, MHL, WW, ITU-HIOH, ITU-IFH, ITU-DEH, and UO-EMH. All respective responses corresponding to the MHL, WW, ITU-HIOH, ITU-IFH, ITU-DEH, and UO-EMH were averaged and encapsulated to obtain mean scores and represent distinctive data distributions visually.
4.1 Digital Workers’ Demographics and Background Information
Table 2 presents a summary of the demographic information and work-related attributes collected from 326 digital workers. Specifically, more than half of the respondents were males (56.7%, n = 185), while approximately 66% (n = 216) were below 40 years old, wherein 36% (n = 117) were between 20 and 29 years old (below 30 years old). Furthermore, Malaysian Chinese workers were the majority of the respondents (65.3%, n = 213), followed by Malays (26.7%, n = 87), and Indians (4.3%, n = 14) respectively. The ethnicity proportion was not concurrent with the actual Malaysian ethnic structure, where Malays belong to the majority group, followed by Chinese and Indians.
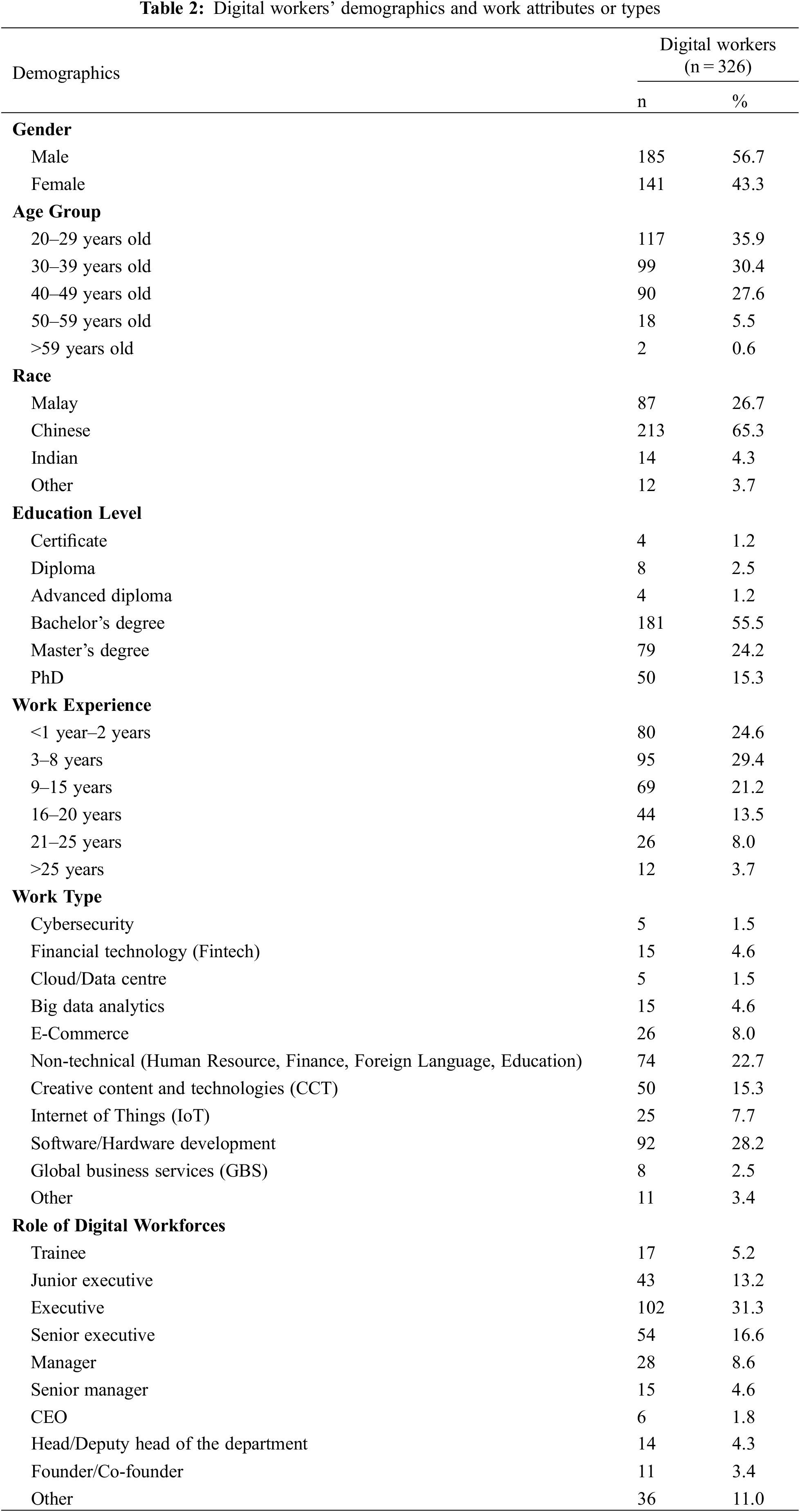
29.4% (n = 95) of the participants were employees with 3 to 8 years of working experience, while the remaining (75.2%, n = 244) possessed 15 years and below of working experience. The workers were involved in several major job types in the digital industry, including software or hardware development (28.2%, n = 92), non-technical work (human resource management, finance, management, and education; 22.7%, n = 74), and creative content and technologies (15.3%, n = 50). A total of 55.5% (n = 181) possessed a Bachelor’s degree, 24.2% (n = 79) a Master’s degree, and 15.3% (n = 50) a PhD. A total of 31.3% (n = 102) were holding a role as an executive in their current workplace, followed by 16.6% (n = 54) as a senior executive, while another 9.5% (31) performing leadership roles, such as the chief executive officer, founder, and head of the department.
4.2 The MHL and WW Levels amongst Digital Workers
The data distributions or histograms of the MHL and WW variables (refer to Table 3) demonstrated a satisfactory normal distribution (refer to each thumbnail image) with acceptable skewness statistics, which were −0.42 and −0.30 for both MHL and WW variables, respectively. As the two values were within the skewness threshold of –2.00 and +2.00, the results suggested the two variables were normally distributed amongst the respondents. Table 3 and Fig. 3 respectively depict the moderate to high MHL levels amongst the respondents.
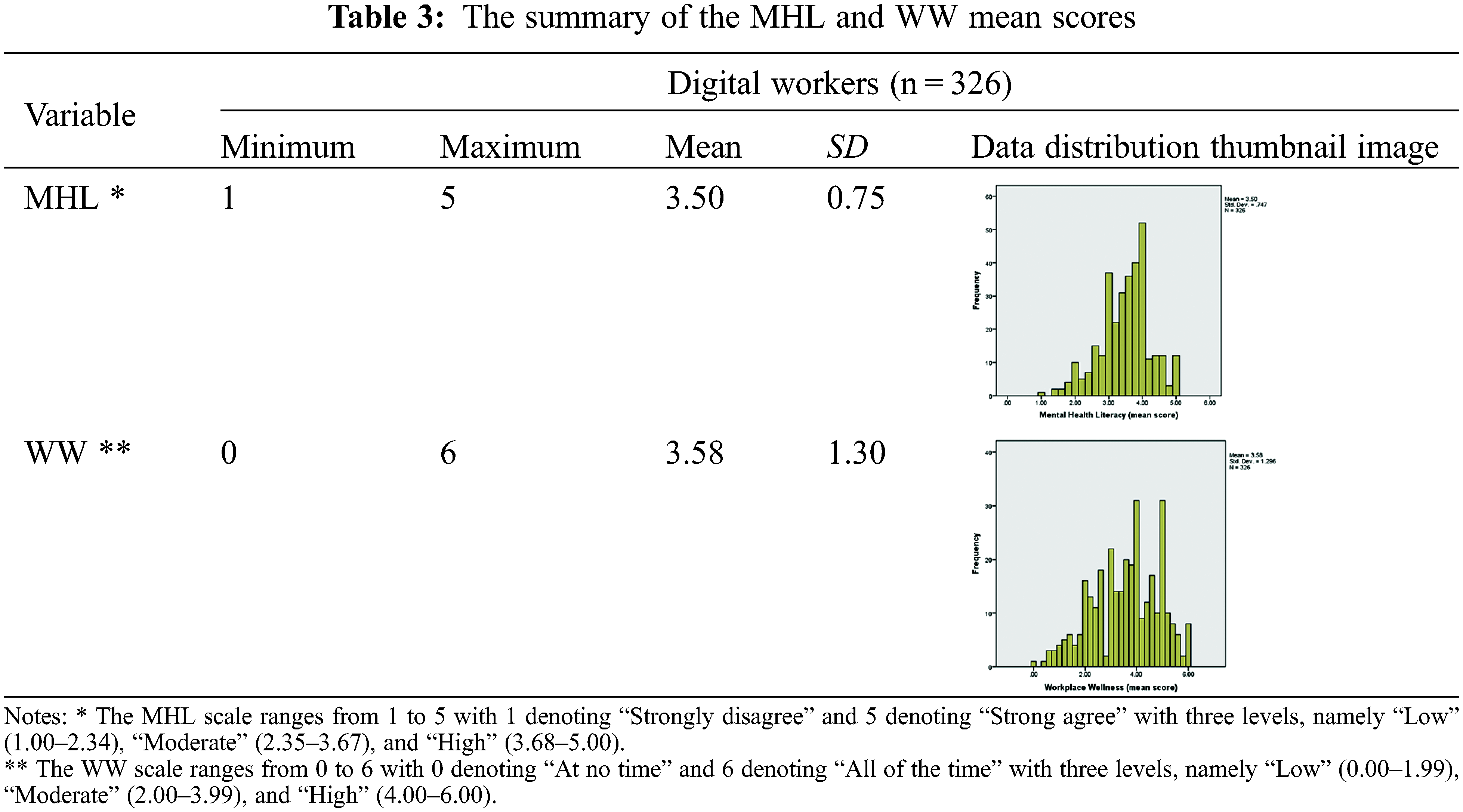

Figure 3: The MHL and WW variables categorised at high, moderate, and low levels
The MHL and WW scores were categorised into three levels by equally dividing the scales employed for the variables. The MHL score included the levels of “Low” (1.00–2.34), “Moderate” (2.35–3.67), and “High” (3.68–5.00), whereas the WW score included the degrees of “Low” (0.00–1.99), “Moderate” (2.00–3.99), and “High” (4.00–6.00). The frequency of each category was calculated and both variables revealed similar distributions, although the WW variable was slightly more dispersed. Meanwhile, the MHL descriptive measures demonstrated the following indicators, namely mean = 3.50 and SD = 0.75, with 49% (n = 160) of the respondents at a moderate level and another 44% (n = 143) at the high level. For the WW variable, the mean was discovered at 3.58 and SD at 1.30, with 46% (n = 150) of the respondents at the moderate level while another 44% (n = 143) at the high level. Although merely a small percentage or number of digital workers scored low in the MHL (7%, n = 23) and the WW (10%, n = 33) variables, mental health issues should not be neglected as organizational or environmental support was essential to their well-being.
A simple bivariate analysis employing the Pearson correlation method on the MHL and WW variables was conducted. The one-tailed significance result is displayed in Table 4, which shows a positive correlation between the variables (r = 0.150, p < 0.05). The finding revealed a significant positive relationship between the two variables, suggesting a higher MHL level would enhance respondents’ WW. Several studies also reported the MHL importance on an individual’s wellness. For instance, Lee et al. [54] discovered from a sample size of 732 that higher MHL degrees contributed to a more positive mental health attitude and greater acceptance of mental health stigma. Similarly, Kurki et al. [55] revealed that participants in a mental health programme increased their mental health knowledge and improved personal emotional symptoms, which were adequately sustained as manifested in a follow-up study after two months. As such, the participants ably maintained the beneficial results of reduced stress and improved ability to seek pertinent assistance.

4.3 The EMH Usage Intention and Utilization Levels
The data distribution or histograms of the ITU-HIOH, ITU-IFH, and ITU-DEH variables (refer to Table 5) manifested acceptable normal distributions respectively (see each thumbnail image), with the skewness statistics of the three intention variables as –0.30, –0.36, and –0.47. As the values were situated in the skewness threshold range of –2.00 and +2.00, the results suggested that the data of the three variables were normally distributed.

The ITU-HIOH variable possessed the highest mean value (mean = 3.82, SD = 0.65) compared to other two EMH dimensions, namely the ITU-IFH (mean = 3.70, SD = 0.72) and the ITU-DEH (mean = 3.66, SD = 0.75). Similarly, the data distributions of the three variables were categorised into three levels, namely “Low” (1.00–2.34), “Moderate” (2.35–3.67), and “High” (3.68–5.00). Meanwhile, the UO-EMH variable was categorised into the same three levels with different ranges, in which “Low” between (0.00 and 1.34), “Moderate” between (1.35 and 2.67), and “High” between 2.68 and 4.00. Fig. 4 demonstrates that digital workers (79%, n = 257) who belonged to the “Low” category indicated a minimal utilization extent of the EMH applications in personal daily life, while only 4% (n = 13) were considered active users (“High” category), and 18% (n = 59) were “Moderate” EMH users. The findings also revealed that the mostly employed eHealth services were mobile applications related to fitness and exercise, wearable devices, such as the Apple Watch and Samsung Galaxy Watch, which could measure stress levels and record sleep patterns, calorie counters or diet tracker mobile applications, online meeting technologies, including Zoom, Google Meet, or Facebook Live, to attend mental health experts’ webinars in providing mental health educational discourses.

Figure 4: Digital workers’ high, moderate, and low percentages of the ITU-HIOH, ITU-IFH, ITU-DEH, and UO-EMH variables
4.4 Digital Workers’ EMH Open Feedback
The qualitative analysis of digital workers’ open feedback revealed a finding trend in personal EMH perspectives regarding workplaces (refer to Fig. 5), after receiving voluntary responses from 80 of the total participants. The following analyses (with percentage values) were administered solely on 80 respondents’ feedback by perusing and categorising each response into relevant themes as presented in Fig. 5. 22% of the total responses were related to the EMH being innovative support in the contemporary era, for example, “… still not very common for discussion in Malaysia society” and “not really have much feedback as this sounds very new to me, but appreciate you started to work on it”. The remaining participants who did not provide any open feedback contributed personal thoughts or comments only in the form of quantitative data, as explored in the previous sections.

Figure 5: Digital workers’ EMH open feedback
Several participants conveyed a highly positive EMH view and expressed the importance of increasing mental health awareness. About 45% of the open feedback specified respondents’ EMH positivity, for instance, “E-mental health is important for the advancement of today’s society no matter in developed or developing countries, … the well-being of all plays key roles to healthy nation-building”, or “… good initiative and valuable information to provide improvement plans for all the related organizations… to drive National Digital Development framework”. Simultaneously, certain respondents (10%) stated that the current EMH study was highly timely, which was perceived as beneficial research work (11%) and should be promoted during the COVID-19 pandemic since mental health was a major societal issue. Specifically, “I am unaware of e-mental services being available until doing this survey. Mostly, for my own mental health I will perform my own readings or consult counsellors”, “I think it will be a good approach, some more during movement control orders, seeing nowadays with the pandemic, people’s health is affected heavily”, “Good for people as nowadays almost everyone has their own gadgets and city stress level high”, and “Mental health is one of the most neglected public health, hopefully e-mental health applications may be promoted to all for self-help via professional counselling. Linked up with Befriender, maybe great to support this”.
Several participants (5%) mentioned that they encountered mental health and stress issues and communicated that they would require more knowledge of employing the EMH, such as “I always feel uncomfortable with my mental health… need more data & assist from this info”, “I am glad to know there is such a thing because mental health has been quite an issue in my life for the past few years”, and “So far only use mobile apps like for exercising to help release stress, I wish to know if there are groups that provide counselling to talk about the problem”. Nevertheless, certain respondents informed personal concerns about the EMH innovation, especially regarding data security and privacy (8%). For instance, “E-mental health would be better and more accepted if the data privacy, security is taken care of”. Besides, a small number of the respondents (6%) mentioned that the EMH was not a necessity due to personal perception of the inefficiency in providing enhanced therapy for mental health patients. 4% of the participants also expressed that mental health was a social stigma and taboo, especially in workplaces. For example, “Some big companies will perform a background check and specific inquiries whether you have a history of past mental illness or not. Malaysia still has discrimination against people who have past mental illnesses”. Notwithstanding, several optimistic EMH comments existed, such as “E-mental health should be or might be very helpful to people nowadays as most of the people might feel ashamed or not confident to share their story or problems face to face with outsiders.” Summarily, the expressed opinions were valuable in gauging digital workers’ actual mental health and EMH viewpoints.
While the digital industry and digital economy have been accelerated by the COVID-19 pandemic, several pertinent research questions existed regarding digital workers’ wellness management methods, the MHL influence on personal wellness, and personal EMH acceptance, usage, and feedback levels to be addressed and discussed. During the COVID-19 pandemic, digital workers from various digital firms possessed MHL and WW ranging from moderate to high levels, in which both variables were significantly and positively associated based on the correlation analysis. Concurrently, the existing literature [28,31,51] reported the pandemic challenges experienced by digital workers, especially the blurring of the work-life balance boundary, which engendered an increase in the prevalence of mental health issues. Particularly, at least 51% of Malaysian workers reported at least one work-related stress dimension in 2019 [32]. The current study also demonstrated that 46% of digital workers were moderately well while a small percentage of them (10%) possessed low wellness levels in the workplace. Summarily, about 56% of digital workers had encountered certain workplace challenges, consistent with the findings of the AIA Healthiest Workplace Survey [32], whereas the remaining 44% achieved a high WW level. Nevertheless, a moderate wellness level suggested the general experience of satisfactory wellness with occasionally a stress-related workplace issue.
5.1 Wellness Programmes for Digital Workers
The current study demonstrated that 10% of digital workers (n = 33) and 7% (n = 23) reported low WW and MHL levels, respectively. Although merely a small percentage experiencing the low MHL and WW levels, small group intervention programmes could be tailored to this group. Similarly, as analysed from the open feedback, four respondents mentioned their mental health issues experiences past several years, in which the EMH could serve as a promising solution for required mental health support. The EMH played an important role in broadening access to care and maximising the effectiveness and accessibility of mental health services [12].
Although digital workers in the digital industry manifested a high EMH usage intention level, the EMH utilization was recorded at a low degree [47]. The innovative service was the main contributing factor to the low usage percentage, thus suggesting higher EMH exploration levels to raise mental health awareness amongst digital workers. The gap between high-interest levels but low usage numbers was also revealed by past findings that increased EMH acceptance did not directly translate into high utilization extents [46]. Contemporarily, various EMH interventions remained in the infancy stage and were less well-known in Malaysia as evidenced by the low actual EMH usage, wherein the respondents rarely employed the services or lacked prior usage experiences [2]. The finding was also supplemented by participants’ open feedback that the EMH is an unfamiliar application and higher awareness levels were required, due to several factors, such as unstandardised regulations for data quality and protection or the willingness of both patients and therapists to participate in web-based therapeutic endeavours [47]. Nevertheless, the COVID-19 pandemic could also contribute to the higher EMH usage intention level in the present study. Webelhorst et al. [47] propounded that the COVID-19 circumstances might have accelerated the use of remote services and could positively influence acceptance scores of available EMH services albeit the usage experience was limited.
As manifested by the study findings, applications, or apps, related to personal self-management, mindfulness, and the HIOH contents were slightly more accepted compared to apps comprising the IFH and DEH domains. The higher acceptance indicated that the HIOH domain should be prioritised when implementing pertinent EMH innovations. Nevertheless, all three EMH domains possessed respective potentials by offering different strengths to assist in digital employees’ mental health support, as mental health issues were more prevalent during the pandemic. As such, the EMH is important and beneficial to be applied in the current digital era, especially in Malaysian society, where mental health remains a taboo topic and rarely discussed in workplaces and societies. Lattie et al. [12] propounded that the EMH ably maintained the anonymous identity of individuals seeking support while providing highly accessible teletherapy opportunities. To increase the EMH acceptance level, existing issues, such as user privacy, data security, and diagnosis verification (reliability and verifiability) were required to be foremostly addressed. The concerns are the fundamental criteria for enhancing user acceptance with high levels of security, accuracy, and reliability before the EMH could extensively and continuously be promoted.
Another study pointed out that lacking the EMH treatment knowledge would engender uncertainties on the effectiveness and subsequently result in a lower future usage willingness [56], as eHealth intervention knowledge was frequently associated with higher acceptance ratings of the interventions [50,57]. Similarly, e-health interventions would not be refused or reluctantly accepted by users who possessed relevant utilization experience. Nonetheless, the issues were centred on awareness scarcity regarding technology instrumentality. To enhance the EMH intervention acceptance, a higher EMH literacy level, which is done by constantly promoting the EMH utilization benefits while elevating the EMH accessibility, would be imperative [56].
Professional learning and development personnel are required to be introduced to various EMH applications before elucidating the app functionality to potential users, medical institution employees, and patients to effectively execute the EMH technology. To be concurrent with the e-health development progress and provide versatile health improvement tools, users’ health literacy plays a significant role in seamlessly applying available e-health or EMH applications [58]. It is also asserted that the EMH service acceptance would be highly dependent on familiarity and personal attitudes [48]. To accelerate the preventive innovation process, the action of promoting and educating the public, healthcare providers, and employers about the EMH benefits is essential. For instance, relevant EMH acceptance-promoting programmes could be developed to inculcate the importance of achieving long-term, sustainable, and positive health outcomes through the EMH employment. Tailored EMH education could also assist in alleviating public scepticism surrounding mental health [48].
The current study employed only purposive sampling, and the digital workers’ population did not comprehensively represent the entire Malaysian digital employees, which might produce potential biases in certain industrial groups. Furthermore, the data were collected mainly from the alumni of selected universities, as the questionnaire was disseminated with the alumni representatives’ assistance during the data collection phase. The MCO implementation due to the COVID-19 pandemic situation could also affect the extensive population coverage during the survey distribution stage. Besides, the present study did not qualitatively collect in-depth EMH usage data, although open feedback from approximately one-fourth of the respondents was received. Hence, in-depth interviews or focus group discussions could be conducted to garner further insights regarding personal EMH utilization and generate highly comprehensive findings to thoroughly explicate the relationship between high usage intention and interest yet low actual utilization.
The study contributed to the existing knowledge corpus by establishing a concise EMH framework regarding Malaysian digital workers’ EMH usage intention, wherein the HIOH dimension received slightly higher acceptance than the IFH and DEH dimensions. During the COVID-19 pandemic, the digital workers demonstrated moderate to high MHL and WW levels, and both variables were discovered to be positively correlated. Table 6 outlines a summary of the current study findings, in which a high EMH usage intention was revealed, but the actual EMH usage remained at a low level. As such, an in-depth analysis would be required to determine the applicable methods of the EMH integration into workplaces in boosting digital employees’ mental health. For example, informing the workers about mental health services at different stages and investigating personal usage patterns or habits would be effective in increasing the EMH awareness and acceptance degrees. Moreover, collecting further EMH usage data could assist in identifying the contributing factors to the low utilization rate.

As the EMH availability could enable higher accessibility to required mental health services, relevant EMH literacy campaigns and seminars should be highly conducted to create more awareness, particularly in workplaces. Accordingly, the factors of openness, security, data privacy protection, and data verification would be key to promoting actual and higher usage levels. The current findings would also provide valuable insight and guidance for OSH experts, eHealth developers, services providers, and policymakers in the practical EMH adoption.
Future studies are recommended to conduct meticulous analyses to appraise the relationships of additional variables than those measured in the current study, including demographic variables and the ITU-EMH domain. For example, inferential statistics or partial least squares regression could be administered to perform the succeeding analysis level. A subsequent effort is also suggested to introduce the EMH amongst digital employees to promote actual usage and improve mental health support in workplaces. Correspondingly, qualitative interviews could be conducted to investigate personal EMH usage in multiple aspects to allow the collected data in revealing highly comprehensive insights, such as utilization habits or patterns, favourable or unfavourable features, and usage challenges. The findings could assist in identifying the reasons behind the currently low EMH usage before developing a more effective and sustainable EMH implementation in workplaces.
Employees from various industries could be investigated regarding personal EMH usage intention and actual employment. The discovered findings would benefit most Malaysian workers by providing a deeper understanding of personal EMH views and requirements before deploying the mental health support innovation to workplaces extensively. In addition, organizational measures and interventions to aid in boosting digital workers’ mental health and well-being are research efforts to be undertaken by future studies. Exploring applicable transformations would be effective to empower and value digital workers’ mental health and well-being by proposing policy recommendations to guide healthcare leaders and health systems. The exploration is adhering to the recent policy brief of the United Nations on the COVID-19 pandemic, specifically the imperative for mental health implementation through systemic actions [59].
Certain companies implemented health and well-being programmes which could connect to the community, such as on-site health centres, financial counselling, and other pertinent interventions [7]. The implementation could be further assessed as additional community service research on a larger scale by involving the entire digital employee community. Health awareness activities, such as cancer screenings, health awareness talks, workshops on employing health applications, and understanding mental health literacy, could be strategised as a community programme for digital workers. Concurrently, a tracking system which records mental health literacy, workplace wellness awareness, the EMH utilization rate, and other indicators could also be designed to facilitate the MHL and WW in the future. As such, enhanced workplace policies or guidelines to govern a better occupational work environment would support the digital industry and the future of work, which address the appeal of the United Nations on the importance of tackling mental health issues, including (1) applying a whole-of-society approach to promote, protect, and care for mental health, (2) ensuring widespread availability of emergency mental health and psychosocial support, and (3) supporting recovery from COVID-19 by building mental health services for the future [17], particularly during the COVID-19 pandemic.
Acknowledgement: The authors would like to express appreciation to the anonymous reviewers for their highly constructive comments on the draft of the paper. Appreciation also goes the six reviewers in reviewing the survey instrument. Lastly, acknowledgement goes to the Funder, the Ministry of Higher Education (MOHE) for approving FRGS Grant to this project.
Authorship: The authors confirm contribution to the paper as follows: Study conception and design: KAC, TCH, HR, SWF, CWO-A, EAS; data collection: All Authors; analysis and interpretation of results: TCH, KAC; draft manuscript preparation: TCH, KAC; All authors reviewed the papers and the results and approved the final version of the manuscript.
Funding Statement: This research is supported by the Malaysia Ministry of Higher Education’s Fundamental Research Grant Scheme (FRGS) [FRGS/1/2019/SS09/MMU/02/3] or MMUE/190073 led by the second author. The url of the sponsor’s website is http://mygrants.gov.my/main.php?Content=articles&ArticleID=1&IID=.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Pendit, U. C., Koo, A. C. (2020). Openness towards mental illness in Malaysia. e-BANGI, 17(3), 46–56. [Google Scholar]
2. Chan, M. H. C., Ng, S. L., In, S., Wee, L. H., Siau, C. S. (2021). Predictors of psychological distress and mental health resource utilization among employees in Malaysia. International Journal Environmental Research Public Health, 18(1), 314. DOI 10.3390/ijerph18010314. [Google Scholar] [CrossRef]
3. Peters, S. E., Dennerlein, J. T., Wagner, G. R., Sorensen, G. (2022). Work and worker health in the post-pandemic world: A public health perspective. The Lancet Public Health, 7(2), e188–e194. DOI 10.1016/S2468-2667(21)00259-0. [Google Scholar] [CrossRef]
4. Tamers, S. L., Streit, J., Pana-Cryan, R., Ray, T., Syron, L. (2020). Envisioning the future of work to safeguard the safety, health, and well-being of the workforce: A perspective from the CDC’s national institute for occupational safety and health. American Journal of Industrial Medicine, 63(12), 1065–1084. DOI 10.1002/ajim.23183. [Google Scholar] [CrossRef]
5. Sorensen, G., Dennerlein, J. T., Peters, S. E., Sabbath, E. L., Kelly, E. L. (2021). The future of research on work, safety, health and wellbeing: A guiding conceptual framework. Social Science and Medicine, 269, 113593. DOI 10.1016/J.SOCSCIMED.2020.113593. [Google Scholar] [CrossRef]
6. Ministry of Human Resources Malaysia (2018). Safety and health policy. NIOSH Malaysia. http://www.niosh.com.my/corporate-info/niosh-policy/safety-and-health-policy. [Google Scholar]
7. Adams, J. M. (2019). The value of worker well-being. Public Health Reports, 134(6), 583–586. DOI 10.1177/0033354919878434. [Google Scholar] [CrossRef]
8. Chastney, R. (2020). Explore: The digital industry. https://www.futurelearn.com/info/blog/explore-the-digital-industry. [Google Scholar]
9. Zorzenon, R., Lizarelli, F. L., Daniel, D. B. A. (2022). What is the potential impact of Industry 4.0 on health and safety at work? Safety Science. DOI 10.1016/J.SSCI.2022.105802. [Google Scholar] [CrossRef]
10. Boucher, E. M., Harake, N. R., Ward, H. E., Stoeckl, S. E., Vargas, J. (2021). Artificially intelligent chatbots in digital mental health interventions: A review. Expert Review of Medical Devices, 18(sup1), 37–49. DOI 10.1080/17434440.2021.2013200. [Google Scholar] [CrossRef]
11. Goetz, C., Bavaresco, R., Kunst, R., Barbosa, J. (2022). Industrial intelligence in the care of workers’ mental health: A review of status and challenges. International Journal of Industrial Ergonomics, 87, 103234. DOI 10.1016/j.ergon.2021.103234. [Google Scholar] [CrossRef]
12. Lattie, E. G., Stiles-Shields, C., Graham, A. K. (2022). An overview of and recommendations for more accessible digital mental health services. Nature Reviews Psychology, 1(2), 87–100. DOI 10.1038/s44159-021-00003-1. [Google Scholar] [CrossRef]
13. Wang, Y., Li, B., Liu, L. (2020). Telemedicine experience in China: Our response to the pandemic and current challenges. Frontiers in Public Health, 8, 549669. DOI 10.3389/fpubh.2020.549669. [Google Scholar] [CrossRef]
14. Shaw, T., Mcgregor, D., Sci, B. A., Path, S., Care, M. H. (2017). What is eHealth (6)? Development of a conceptual model for eHealth: Qualitative study with key informants. Journal of Medical Internet Research, 19(10), 1–12. DOI 10.2196/jmir.8106. [Google Scholar] [CrossRef]
15. Søvold, L. E., Naslund, J. A., Kousoulis, A. A., Saxena, S., Qoronfleh, M. W. (2021). Prioritizing the mental health and well-being of healthcare workers: An urgent global public health priority. Frontiers in Public Health, 9, 514. DOI 10.3389/FPUBH.2021.679397/BIBTEX. [Google Scholar] [CrossRef]
16. Ghobakhloo, M. (2020). Industry 4.0, digitization, and opportunities for sustainability. Journal of Cleaner Production, 252, 119869. DOI 10.1016/J.JCLEPRO.2019.119869. [Google Scholar] [CrossRef]
17. Schwab, K. (2017). The fourth industrial revolution. New York: Crown Business. [Google Scholar]
18. Lasi, H., Fettke, P., Kemper, H. G., Feld, T., Hoffmann, M. (2014). Industry 4.0. Business and Information Systems Engineering, 6(4), 239–242. DOI 10.1007/S12599-014-0334-4. [Google Scholar] [CrossRef]
19. Economic Planning Unit of Prime Minister’s Department Malaysia (2021). National fourth industrial revolution (4IR) policy. EPU Prime Minister’s Department. https://www.youtube.com/watch?v=iD00dOYHvlU. [Google Scholar]
20. MDEC Corporate Affairs Division (2022). Malaysia digital is set to accelerate growth of digital economy. https://mdec.my/news/malaysia-digital-is-set-to-accelerate-growth-of-digital-economy/. [Google Scholar]
21. Kadir, B. A., Broberg, O. (2020). Human well-being and system performance in the transition to Industry 4.0. International Journal of Industrial Ergonomics, 76, 102936. DOI 10.1016/j.ergon.2020.102936. [Google Scholar] [CrossRef]
22. Sparrow, D. E., Kruger, K., Basson, A. H. (2021). An architecture to facilitate the integration of human workers in Industry 4.0 environments. International Journal of Production Research, 60(15), 1–19. DOI 10.1080/00207543.2021.1937747. [Google Scholar] [CrossRef]
23. Russell, E., Grant, C. (2020). Introduction to agile working and well-being in the digital age. In: Grant, C., Russell, E. (Eds.Agile working and well-being in the digital age. Cham: Palgrave Macmillan. DOI 10.1007/978-3-030-60283-3_1. [Google Scholar] [CrossRef]
24. MDEC (2020). Digital workforce COVID impact survey 2020: Digital talent development. https://mdec.my/wp-content/uploads/Digital-Workforce-Covid-Talent-Impact-Survey-2020.pdf. [Google Scholar]
25. Florsheim, L. (2022). Google CEO sundar pichai’s vision for return to work. The Wall Street Journal. https://www.wsj.com/articles/google-ceo-sundar-pichais-vision-for-return-to-work-11646055640. [Google Scholar]
26. IBM Cloud Education. (2021). What is a digital worker? IBM Cloud Learn Hub. https://www.ibm.com/cloud/learn/digital-worker#toc-challenges-VCOky9f-. [Google Scholar]
27. PricewaterhouseCoopers (2020). Digital resilience in a new world: PwC Malaysia’s survey on technology, jobs and skills. https://www.pwc.com/my/en/publications/2020/digital-resilience-in-a-new-world.html. [Google Scholar]
28. Marimuthu, P., Vasudevan, H. (2020). The psychological impact of working from home during coronavirus (COVID-19) pandemic: A case study. CnR’s International Journal of Social & Scientific Research, 6(1), 18–29. [Google Scholar]
29. PricewaterhouseCoopers (2021). PwC’s hopes and fears survey 2021: Malaysia report. https://www.pwc.com/my/newworldnewskills. [Google Scholar]
30. Leiter, M. P., Wintle, J. (2021). Burnout in organizations. In: Oxford research encyclopedia of psychology. Oxford: Oxford University Press. DOI 10.1093/acrefore/9780190236557.013.874. [Google Scholar] [CrossRef]
31. Vargas-Llave, O., Mandl, I., Weber, T., Wilkens, M. (2020). Telework and ICT-based mobile work: Flexible working in the digital age. Luxembourg: Publications Office of the European Union. DOI 10.2806/70118. [Google Scholar] [CrossRef]
32. Syed Jaafar, S. (2019). Malaysia’s healthiest workplace survey back for third year. Petaling Jaya, Malaysia: The Edge Market. https://www.theedgemarkets.com/content/advertise/malaysias-healthiest-workplace-survey-back-third-year. [Google Scholar]
33. Xiao, Y., Becerik-Gerber, B., Lucas, G., Roll, S. C. (2021). Impacts of working from home during COVID-19 pandemic on physical and mental well-being of office workstation users. Journal of Occupational and Environmental Medicine, 63(3), 181–190. DOI 10.1097/JOM.0000000000002097. [Google Scholar] [CrossRef]
34. Ministry of Human Resource (2021). Inisiatif KSM menangani pandemik COVID-19 [Initiative of KSM for combating COVID-19 pandemic]. https://www.mohr.gov.my/images/flipbook/inisiatifKSM/mobile/index.html#p=18. [Google Scholar]
35. Department of statistics Malaysia (DoSM) (2022). Welfare service statistics, interactive visualisation, DoSM. https://www.dosm.gov.my/v1/index.php?r=column/cthree&menu_id=K3k2VmMrQ3hwQzdYWDVDeDFRdVFDUT09. [Google Scholar]
36. National Institute of Health (NIH) (2020). National health and morbidity survey 2019 non-communicable diseases, healthcare demand, and health literacy: Key findings. http://bit.ly/NHMS2019. [Google Scholar]
37. Institute for Public Health (IPH) (2018). National health and morbidity survey (NHMS) 2017: Key findings from the adolescent health and nutrition surveys-infographic booklet. https://www.iku.gov.my. [Google Scholar]
38. Department of Statistics Malaysia (2021). Labour force Malaysia November 2021. https://www.dosm.gov.my/v1/uploads/files/1_Articles_By_Themes/Labour_Force/Monthly/2021/Nov%202021/LABOUR%20FORCE%20REPORT%20(NOVEMBER%202021).pdf. [Google Scholar]
39. Alimun, R., Ismail, Z., Ab. Shokor, S. S. (2020). Mental health indicators among generation Y. Global Business & Management Research, 10(3), 589–597. [Google Scholar]
40. Azuddin, A. (2020). MCO and mental well-being: Home sweet home ? In: Part 1: Housing and crowding during the MCO, pp. 1–42. https://www.centre.my/post/mco-and-mental-health-living. [Google Scholar]
41. Whaibeh, E., Mahmoud, H., Naal, H. (2020). Telemental health in the context of a pandemic: The COVID-19 experience. Current Treatment Options in Psychiatry, 1–5. DOI 10.1007/s40501-020-00210-2. [Google Scholar] [CrossRef]
42. Robbins, T., Hudson, S., Ray, P., Sankar, S., Patel, K. (2020). COVID-19: A new digital dawn? Digital Health. DOI 10.1177/2055207620920083. [Google Scholar] [CrossRef]
43. Lal, S. (2019). E-mental health: Promising advancements in policy, research, and practice. Healthcare Management Forum, 32(2), 56–62. DOI 10.1177/0840470418818583. [Google Scholar] [CrossRef]
44. Lal, S., Adair, C. E. (2014). E-mental health: A rapid review of the literature. Psychiatric Services, 65(1), 24–32. DOI 10.1176/appi.ps.201300009. [Google Scholar] [CrossRef]
45. Fu, Z., Burger, H., Arjadi, R., Bockting, C. L. H. (2020). Effectiveness of digital psychological interventions for mental health problems in low-income and middle-income countries: A systematic review and meta-analysis. The Lancet Psychiatry, 7(10), 851–864. DOI 10.1016/S2215-0366(20)30256-X. [Google Scholar] [CrossRef]
46. Braun, P., Drüge, M., Hennemann, S., Nitsch, F. J., Staeck, R. (2022). Acceptance of e-mental health services for different application purposes among psychotherapists in clinical training in Germany and Switzerland: Secondary analysis of a cross-sectional survey. Frontiers in Digital Health, 4, 1–15. DOI 10.3389/fdgth.2022.840869. [Google Scholar] [CrossRef]
47. Webelhorst, C., Jepsen, L., Rummel-Kluge, C. (2020). Utilization of e-mental-health and online self-management interventions of patients with mental disorders–A cross-sectional analysis. PLoS One, 15(4), 1–15. DOI 10.1371/journal.pone.0231373. [Google Scholar] [CrossRef]
48. Apolinário-Hagen, J., Hennemann, S., Kück, C. et al. (2020). Exploring user-related drivers of the early acceptance of certified digital stress prevention programs in Germany. Health Services Insights, 13. DOI 10.1177/1178632920911061. [Google Scholar] [CrossRef]
49. Hennemann, S., Witthöft, M., Bethge, M., Spanier, K., Beutel, M. E. (2018). Acceptance and barriers to access of occupational e-mental health: Cross-sectional findings from a health-risk population of employees. International Archives of Occupational and Environmental Health, 91(3), 305–316. DOI 10.1007/s00420-017-1280-5. [Google Scholar] [CrossRef]
50. Eichenberg, C., Wolters, C., Brähler, E. (2013). The internet as a mental health advisor in Germany-results of a national survey. PLoS One, 8(11), 24278121. DOI 10.1371/journal.pone.0079206. [Google Scholar] [CrossRef]
51. Apolinário-Hagen, J., Hennemann, S., Fritsche, L. (2019). Determinant factors of public acceptance of stress management apps: Survey study. JMIR Mental Health, 6(11), e15373. DOI 10.2196/15373. [Google Scholar] [CrossRef]
52. Schaufeli, W. B., Bakker, A. B., Salanova, M. (2006). The measurement of work engagement with a short questionnaire: A cross-national study. Educational and Psychological Measurement, 66(4), 701–716. DOI 10.1177/0013164405282471. [Google Scholar] [CrossRef]
53. Venkatesh, V. (2006). User acceptance of information technology: Toward a unified view. MIS Quarterly, 27(3), 425–478. DOI 10.1201/9780849375477.ch230. [Google Scholar] [CrossRef]
54. Lee, H. Y., Hwang, J., Ball, J. G., Lee, J., Yu, Y. (2020). Mental health literacy affects mental health attitude: Is there a gender difference? American Journal of Health Behavior, 44(3), 283–291. DOI 10.5993/AJHB.44.3.1. [Google Scholar] [CrossRef]
55. Kurki, M., Gilbert, S., Mishina, K., Lempinen, L., Luntamo, T. (2021). Digital mental health literacy-program for the first-year medical students’ wellbeing: A one group quasi-experimental study. BMC Medical Education, 1–11. DOI 10.1186/s12909-021-02990-4. [Google Scholar] [CrossRef]
56. Apolinário-Hagen, J., Fritsche, L., Bierhals, C., Salewski, C. (2018). Improving attitudes toward e-mental health services in the general population via psychoeducational information material: A randomized controlled trial. Internet Interventions, 12, 141–149. DOI 10.1016/j.invent.2017.12.002. [Google Scholar] [CrossRef]
57. Topooco, N., Riper, H., Araya, R., Berking, M., Brunn, M. (2017). Attitudes towards digital treatment for depression: A european stakeholder survey. Internet Interventions, 8, 1–9. DOI 10.1016/j.invent.2017.01.001. [Google Scholar] [CrossRef]
58. Mackert, M., Champlin, S. E., Holton, A., Munoz, I. I., Damásio, M. J. (2014). E-health and health literacy: A research methodology review. Journal of Computer-Mediated Communication, 19(3), 516–528. DOI 10.1111/jcc4.12044. [Google Scholar] [CrossRef]
59. World Health Organization (2020). COVID-19 and the need for action on mental health policy brief. Geneva (CHWHO. [Google Scholar]
Appendix A–Research Instrument
Mental Health Literacy (MHL)
1. I know how to look for helpful mental health resources on the internet/social media.
2. I know how to use the internet/social media to get answers to my questions about mental health.
3. I know what mental health resources are available on the internet/social media.
4. I know where to look for support groups if I face with mental health challenges.
5. I have the skills to evaluate the mental health resources that I received.
Workplace Wellness (WW)
1. I have felt cheerful and in good spirits in my workplace over the past 2 weeks.
2. I have felt calm and relaxed in my workplace over the past 2 weeks.
3. I have felt active and vigorous when I am working over the past 2 weeks.
4. I woke up feeling fresh and rested, and feel like going to work over the past 2 weeks.
5. I find that the work I do is filled with things that interest me over the past 2 weeks.
Intention to Use “health in our hands” (ITU-HIOH)
1. Using “health in our hands” is appropriate for supporting mental health.
2. Using “health in our hands” is appropriate for supporting mental health.
3. I would want to use “health in our hands” technologies to help me manage my mental wellness.
Intention to Use “interacting for health” (ITU-IFH)
1. Using “interacting for health” is appropriate for supporting mental health.
2. Using “interacting for health” would be interesting.
3. I would want to use “interacting for health” technologies to help me manage my mental wellness.
Intention to Use “data enabling health” (ITU-DEH)
1. Using “data enabling health” is appropriate for supporting mental health.
2. Using “data enabling health” would be interesting.
3. I would want to use “data enabling health” methods to help me manage my mental wellness.
Usage of E-Mental Health (UO-EMH)
If you have used the following e-mental health services/applications/devices before, please state the frequency of usage. Please select “Never” if you have never used before.
1. Mindfulness/Motivational/Stress management mobile app (e.g., Shine, Mindfi).
2. Breathing guide mobile app (e.g., Breathe, iBreathe).
3. Meditation/Spiritual mobile app for relaxation (e.g., Calm, Stop Breathe & Think, Simply Being).
4. Wearable device (e.g., Apple watch, Samsung Galaxy watch to track stress level, sleep pattern).
5. Online counselling that give social support to help individuals cope with stress (e.g., Befrienders, SOLS 24/7, Facebook page).
6. Online consultation with doctor (e.g., Doc2Us, Bookdoc, Pulse Prudential).
7. Online webinars of mental health experts giving educational talks regarding mental health (e.g., Facebook Live, Google Meet, Zoom meeting).
8. Self-help e-therapy (e.g., BetterHelp, RELATE, There is Hope).
9. Mood tracker/Mood monitoring mobile app that help to keep track your mood (e.g., MoodPanda, MoodKit).
10. Medication reminder mobile app/devices.
11. Collateral history, thought recorder that can help with mental health diagnostic/management.
12. Calorie counter/diet tracker.
13. Fitness and exercise related mobile app.
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools