
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Validity and Reliability of the Preference for and Tolerance of the Intensity of Exercise Questionnaire among Chinese College Students
1
Body-Brain-Mind Laboratory, Shenzhen Humanities & Social Sciences Key Research Bases of the Center for Mental Health,
School of Psychology, Shenzhen University, Shenzhen, 518060, China
2
Research Group Degenerative and Chronic Diseases, Movement, Faculty of Health Sciences, University of Potsdam, Potsdam, 14476, Germany
3
School of Rehabilitation, Sport and Psychology, AECC University College, Bournemouth, BH5 2DF, UK
4
Department of Sport, Exercise and Health, University of Basel, Basel, 4052, Switzerland
5
Center for Cognitive and Brain Health, Northeastern University, Boston, MA 02115, USA
6
Beckman Institute, University of Illinois at Urbana-Champaign, Champaign, IL 61801, USA
* Corresponding Author: Liye Zou. Email:
# These authors contributed equally to this work
International Journal of Mental Health Promotion 2023, 25(1), 127-138. https://doi.org/10.32604/ijmhp.2022.022504
Received 08 March 2022; Accepted 18 April 2022; Issue published 29 November 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
The rising prevalence of physical inactivity is in all age groups (e.g., in college students) a major public health issue as not meeting the recommended minimum amount of regular physical activity is linked to adverse health events. Vice versa, there is mounting evidence that achieving the recommended amount of regular physical activity is a vital element to prevent chronic diseases, but there is often an insufficient adherence to planned and structured forms of physical activity (i.e., physical exercises). In this context, there is a large body of evidence indicating that exercise adherence is, among other factors, influenced by exercise-related affective responses. The Preference for and Tolerance of the Intensity of Exercise Questionnaire (PRETIE-Q) has been developed to measure these affective responses (e.g., to specific exercise intensities). So far, no validated Chinese version of the PRETIE-Q has been available in the literature. To address this gap in literature, the present study developed and validated a Chinese version of the PRETIE-Q in a large sample of Chinese college students. Data from a total of 1117 college students were collected for analyses concerning factorial validity and construct validity. The re-test reliability was established using a sample of 150 randomly selected participants. In addition, the level of regular physical activity (PA), cardiorespiratory fitness (CRF), and resilience were used to examine possible links with two domains (preference and tolerance) of the PRETIE-Q. Our results showed that a Chinese version of the PRETIE-Q has a good fit and reliability (Cronbach’s α of 0.72 to 0.85 for preference and tolerance, respectively; ICC: r = 0.72 of preference and r = 0.67 of tolerance; fit indices: χ2 = 21.612, df = 19, p > 0.05, TLI = 0.997, CFI = 0.998, RMSEA = 0.016, SRMR = 0.024). Secondly, positive associations of intensity-tolerance with PA, CRF, and resilience were observed. In summary, this study indicates that the Chinese version of the PRETIE-Q has sound psychometric properties and can be used in Chinese college students. The adapted version of the PRETIE-Q paves the way for further research on exercise-related affective responses in Chinese-speaking samples, although the generalizability of our findings needs to be established for other cohorts such as adolescents and older people with and without chronic diseases.Keywords
The rising level of physical inactivity in the general population is a major challenge for the global health care system [1]. This is because insufficient physical activity plays a role in the increasing prevalence of chronic diseases including hypertension, diabetes mellitus, and psychiatric disorders [2–6]. Physical inactivity is defined as not meeting the amount of regular physical activity that is recommended in established guidelines (i.e., less than 150-min moderate-intensity or less than 75-min vigorous-intensity activities in a week) [7]. Even in adolescents and emerging adults (e.g., college students), the increasing amount of physical inactivity has become a public health issue, for example, approximately 84% of school-age adolescents and 40%–50% of college students do not meet the recommended minimum amount of regular physical activity [8,9]. Therefore, the World Health Organization has taken action to promote physical activity (PA) across all age groups with both healthy people and those with clinical conditions [7]. However, such initiatives have not been very successful because the majority of individuals have difficulty adhering to physical exercise interventions on a regular basis or drop out after rather short time intervals (e.g., 6 months) [10–13]. Thus, finding a way to reduce attrition among individuals who start an exercise program might improve this public health situation.
Over the past decades, researchers have attempted to understand why some people participate in regular exercise while others do not [14–16]. In particular, the low adherence to exercise interventions has prompted researchers to investigate the psychological processes associated with this phenomenon. A number of theories have been proposed by exercise scientists to explain physical inactivity, among which the cognitivism paradigm has been the most prominent one in the past [17]. However, given the fact that the cognitive approach did not satisfactorily explain to explain individual differences in behavior as well as the gap between exercise plans and actions, researchers have started to consider determinants of behavior other than cognitive domains. In recent years, affective mechanisms in particular have taken a prominent role. These mechanisms mainly refer to affective constructs (i.e., affective response), such as pleasure/displeasure and enjoyment [18,19]. In this context, the hedonic theory of exercise motivation has been developed. Ekkekakis et al. undertook research on this basis and found evidence of individual variability and dose-response patterns in the relationship between exercise and affective responses, and proposed a new theoretical framework called the dual-mode model [20]. The dual-mode model proposes that affective responses to exercise are determined by the ongoing interaction between two factors [17]: i) top-down cognitive parameters (i.e., cognitive determinants), for instance self-efficacy, self regulation and self-expression attention to the body; ii) bottom-up interoceptive cues (i.e., physiological sensations), for example signals from chemoreceptors, baroreceptors, and various visceroceptors. This model predicts that the contribution of both factors varies with exercise intensity, thus providing an explanation for heterogeneous affective responses at moderate intensity and more homogenous affective responses at high intensity [21].
Importantly, evidence suggests that personal traits are unstable across individuals, which influences decisions about selecting or tolerating a specific exercise intensity [22]. Thus, two new constructs closely linked to affective responses to exercise were proposed, namely, preference for exercise intensity (or intensity-preference) and tolerance of exercise intensity (or intensity-tolerance) [22]. These concepts are intensity-preference and intensity-tolerance were mainly related to interoceptive stimuli from exercise, as opposed to exteroceptive stimuli and behavioral tendencies (primarily social). Specifically, the items in the standard self-administered questionnaires emphasized responses to exteroceptive stimuli (e.g., visual, auditory, tactile) and corresponding social behavior (e.g., sociability) [23].
To measure these two psychological characteristics of exercise (i.e., intensity-preference and intensity-tolerance), an English-language instrument called the Preference for and Tolerance of the Intensity of Exercise Questionnaire (PRETIE-Q) was developed and introduced by Ekkekakis and colleagues [22] and attracted great attention from researchers around the world. This questionnaire was designed to help researchers to understand the psychological processes leading to exercise attrition [22] and was based on the affect-based exercise prescriptions [24,25] to help improve exercise adherence and population health. Based on the affect-based exercise prescriptions [24,25]. The PRETIE-Q has already been translated into other languages, including the European-Portuguese and Brazilian-Portuguese versions [26,27], but a validated Chinese version currently does not exist. Given that nearly 300 million individuals with chronic diseases who are highly susceptible to physical inactivity are living in China, a tool that would enhance research and practical implementation of physical exercise programs based on information about preference for and tolerance of exercise intensity (such as the PRETIE-Q) is urgently needed. Thus, the primary aim of the current study was to develop and validate a Chinese version of the PRETIE-Q.
The second aim of the study relates to evidence that the level of physical activity plays a critical role in overall well-being and is associated with exercise-intensity tolerance and preference. Evidence for this was found in a study by Hall and colleagues [28] which indicated that the level of physical activity (as measured by a self-administered instrument) was positively linked to tolerance and preference, both with values of r = 0.29. In another study, a sample of 146 adolescents, the maximum oxygen uptake (VO2max) as an objective indicator of cardiorespiratory fitness was linked to intensity-tolerance and intensity-preference [29]. While the above-mentioned evidence suggests that level of physical activity and cardiorespiratory fitness are related to tolerance and preference of exercise intensity, it still remains unclear whether tolerance and preference of exercise intensity are linked to resilience as a mental skill. In this context, resilience refers to the capability to psychologically or emotionally deal with difficulties like a life-threatening change. Typically, individuals with prolonged exercise experience (high level of regular physical activity) have stronger tolerance to withstand physical fatigue and exercise-induced pain. Such increased physical capacity (tolerance is thought to involve bottom-up processing) seems to be associated with resilience (top-down processing) level, but investigations providing empirical evidence are currently scant. Taking the above-presented evidence into account, an investigation into associations of tolerance and preference of exercise intensity with the level of physical activity, VO2max, and resilience was examined in the present study.
Taken together, the aims of the present study were twofold: i) to develop and validate a Chinese version of the PRETIE-Q; ii) to investigate associations of the Chinese version of the PRETIE-Q (intensity-tolerance and intensity-preference) with the regular level physical activity (i.e., operationalized by use of the International Physical Activity Questionnaire), cardiorespiratory fitness (i.e., indicated by VO2max), and resilience (i.e., operationalized by the Connor-Davidson resilience scale). According to the available literature, we hypothesized that a higher preference for low-intensity exercise would be associated with lower levels of physical activity, of cardiorespiratory fitness, and of resilience, whereas greater tolerance of vigorous-intensity exercise would be positively associated with higher levels of the above-mentioned factors. Furthermore, our study will add new knowledge to the literature by evaluating the validity and reliability of the Chinese version of the PRETIE-Q in a Chinese cohort of college students who show a relatively high amount of physical inactivity due to academic studies.
In Study 1, 1245 college students were initially enrolled from different universities across China. These college students were asked to anonymously complete an online questionnaire which is described in the following section in more detail through the Questionnaire-Star platform. Of note, after removing participants who responded with a very short duration (researchers had several tests and were informed about how long the survey should take to complete), 128 participants with invalid responses (e.g., time spent on exercise participation of >16 h or not passed the lie detector quiz) were excluded, resulting in 1117 eligible participants for data analysis (563 women, 554 men, M = 18.90 years, SD = 1.25). In addition to the first 1245 students, another 150 participants were enrolled to examine test-retest reliability. In Study 2, to further validate the PRETIE-Q, 45 college students were recruited to carry out an aerobic fitness test (i.e., VO2max) in the Body-Brain-Mind (BBM) lab situated at Shenzhen University. Prior to starting the questionnaire and lab test in both of the studies, participants were asked to provide informed consent and they were compensated 10 Yuan. This study protocol (ChiCTR2100051475) was approved by the ethical committee of Shenzhen University.
To assess preference for exercise intensity and tolerance-intensity, the PRETIE-Q [22] was used in this study. The PRETIE-Q contains sixteen items and covers two dimensions (eight items per dimension). The preference dimension is assessed via eight items (e.g., I would rather go slow during my workout, even if that means taking more time; items 2, 4, 6, 8, 10, 12, 14, 16 in the questionnaire). The tolerance dimension is assessed via eight items (e.g., While exercising, I try to keep going even after I feel exhausted; items 1, 3, 5, 7, 9, 11, 13, 15 in the questionnaire). Each response to an item was made on a 6-point Likert scale, ranging from 0 (I totally disagree) to 5 (I totally agree). Of note, half of the preference-related items (2, 4, 8, 12) measure low preference and half of the tolerance-related items (1, 3, 9, 13) measure low tolerance, and thus the scores of these items were reversed during analysis. A higher total score indicates a greater perceived level in terms of preference and tolerance of exercise intensity. The English version of the questionnaire has a good internal consistency indicated by a Cronbach’s Alpha of 0.73 to 0.89 for the preference-related dimension and of 0.82 to 0.87 for the tolerance-related dimension [22].
The level of physical activity was assessed by the International Physical Activity Questionnaire-7 (IPAQ-7) [30]. This questionnaire consists of seven questions, which assess the amount of time spent in performing physical activities at specific intensities (e.g., at a light intensity, at moderate intensity, and at vigorous intensity) in the last seven days. Participants indicate whether they had performed a specific activity (e.g., walking) and if so for how often (measured in days per week) and how long (average duration per day) they performed this activity in the last seven days. Their level of physical activity was measured by weighting each type of activity following the energy requirements defined in METs (METs are multiples of resting metabolic rate) and expressed as MET-min per week (MET level*minutes of activity*events per week) [31]. A study on the Chinese version of IPAQ-7 reported the test-retest reliability coefficients of 0.93 for mild, 0.85 for moderate (includes walking), and 0.75 for vigorous exercise [32].
The Connor-Davidson resilience scale (CD-RISC) [33] was used to measure the level of resilience (i.e., the ability to adapt positively, or to maintain or regain mental health, despite experiencing adversity [34]). The Chinese version of the CD-RISC which comprises 25 items, has good validity and reliability [35]. The response to an item is provided on a 5-point Likert scale, ranging from 0 (rarely true) to 4 (true nearly all of the time). The total score ranges between 0 to 100, and a higher score indicates greater resilience. A previous study with college students reported Cronbach’s α of 0.76 (stress resistance), 0.72 (self-control), 0.72 (goal orientation) and 0.60 (social adaptation), respectively [36].
In addition to measurements of these two characteristics (i.e., physical activity level and resilience) in Study 1, maximal oxygen uptake (VO2max) of participants was measured in Study 2. VO2max is considered as the gold standard indicator of cardiorespiratory fitness and was determined by conducting a graded exercise test on a bicycle ergometer (Ergoselect 200 K). The bike was adjusted to each participants’ anthropometric properties by ensuring that the height of the seat and pedals were suitable for each participant. Afterwards, the graded exercise test was started. The first two minutes were a warm-up phase, followed by the requirement of stable pedal rotations (ranging from 55 to 60 per min) regardless of a gradual elevation of 20 W per minute (i.e., starting workload: 0 W, incremental workload: 20 W, additional charge: 1 min by 20 W, cadence: 55–60 rpm). In other words, the participants were asked to keep the cadence (i.e., revolutions per minute) of the bicycle ergometer constant while the workload (resistance) was gradually increased. if one of the following criteria was fulfilled: revolutions lower than 50 r/min, a platform of VO2max, respiratory quotient (RQ) > 1.10 or the heart rate greater than 180 beats/min, the test was terminated. Importantly, all participants were asked to achieve the peak value of oxygen uptake until volitional exhaustion as measured by rating of perceived exertion (i.e., participants had exhausted their strength and asked to interrupt the test). Heart rate was monitored (Polar-H10 chest belt) throughout the fitness test.
Firstly, a researcher from the Body-Brain-Mind Laboratory contacted the author who developed PRETIE-Q and asked for his permission to develop a Chinese version. After this permission was granted, two English-Chinese bilingual researchers who specialized in psychology translated the original questionnaire into the Chinese language (forward translation). Meanwhile, a discussion meeting was set with the original author of the PRETIE-Q to confirm the meaning of items in English. Secondly, the first version of the translated questionnaire was sent to four exercise psychologists who reviewed and provided feedback on this version. This feedback was used to revise the first version of the questionnaire. Thirdly, this Chinese version of the PRETIE-Q was sent to two individuals who are fluent in English and Chinese who were blinded to the aims of this study to independently carry out a back-translation. Of note, given that the meaning of items within the Chinese-to-English version remained unchanged, back translation was successful. Fourthly, the Chinese version was distributed to 21 college students with exercise experience to determine whether items are readable and understandable, in which they felt that several items in the Chinese version were duplicated and suggested deleting them (i.e., items 1, 6, 8, 13, 16 of the original scale). To this end, a discussion was conducted, resulting in the Chinese version of the 11-item PRETIE-Q. To validate this Chinese-language version, a large-scale study was carried out among college students (Study 1), followed by a lab-based data collection on the PRETIE-Q and VO2max (Study 2). For Study 1, several universities were targeted to collect data through the Questionnaire-Star platform, where professors as collaborators helped to provide access to the e-survey for their students. A total of 150 participants were randomly selected to conduct a re-test within 3 weeks.
Data analyses were carried out in SPSS 26.0 (Statistical Package for social science, Version 22, Chicago, IL, USA). Demographic information (i.e., age, gender) were analyzed, and mean (M) and standard deviation (SD) were determined (see Table 1). A total of 1117 college students were randomly separated into two samples in Study 1: i) KMO (Kaiser-Meyer-Olkin) and Bartlett’s test were measured as explanatory factor analysis (EFA) based on Sample 1 with 566 participants; ii) to test the internal consistency, Cronbach’s α was analyzed in Sample 2 with 551 participants; iii) Sample 2 was also used to perform CFA using Mplus software, including the Average Variance Extracted (AVE) value and Construct Reliability (CR) of variables. To measure model fit, the Tucker-Lewis Index (TLI) and other parameters were considered, such as Comparative Fit Index (CFI), Standardized Root Mean Square Residual (SRMR), and Root Mean Square Error of Approximation (RMSEA), with a 90% Confidence Interval (90% CI). For these indices, the following cutoffs were recommended: CFI and TLI ≥ 0.90; SRMR and RMSEA ≤ 0.08. In addition, test-retest reliability was tested among 150 selected participants. With respect to concurrent validity, possible associations between the dimensions of exercise intensity tolerance and preference assessed by the PRETIE-Q and the level of regular physical activity level (subjective measure) and resilience were tested in Sample 2. Likewise, a possible correlation between cardiorespiratory fitness (i.e, operationalized by VO2max) and the tolerance and preference dimension of the PRETIE-Q were examined.
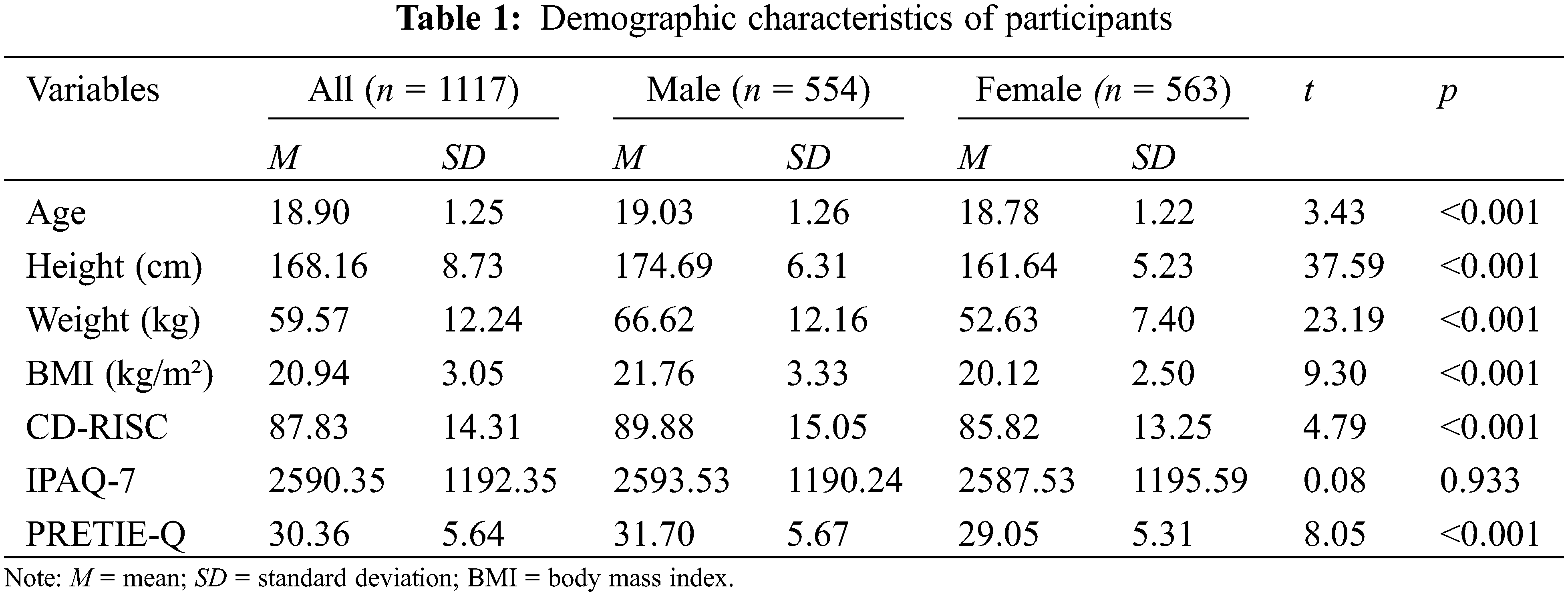
The demographic characteristics of the participants are displayed in Table 1. Men demonstrated significantly higher scores on age (t= 3.43, p< 0.001), BMI (calculated by kg/m2, t= 9.30, p< 0.001), resilience (t= 4.79, p< 0.001), and PRETIE-Q total score (t= 8.05, p< 0.001) as compared with women, whereas a non-significant difference on physial activity level was observed.
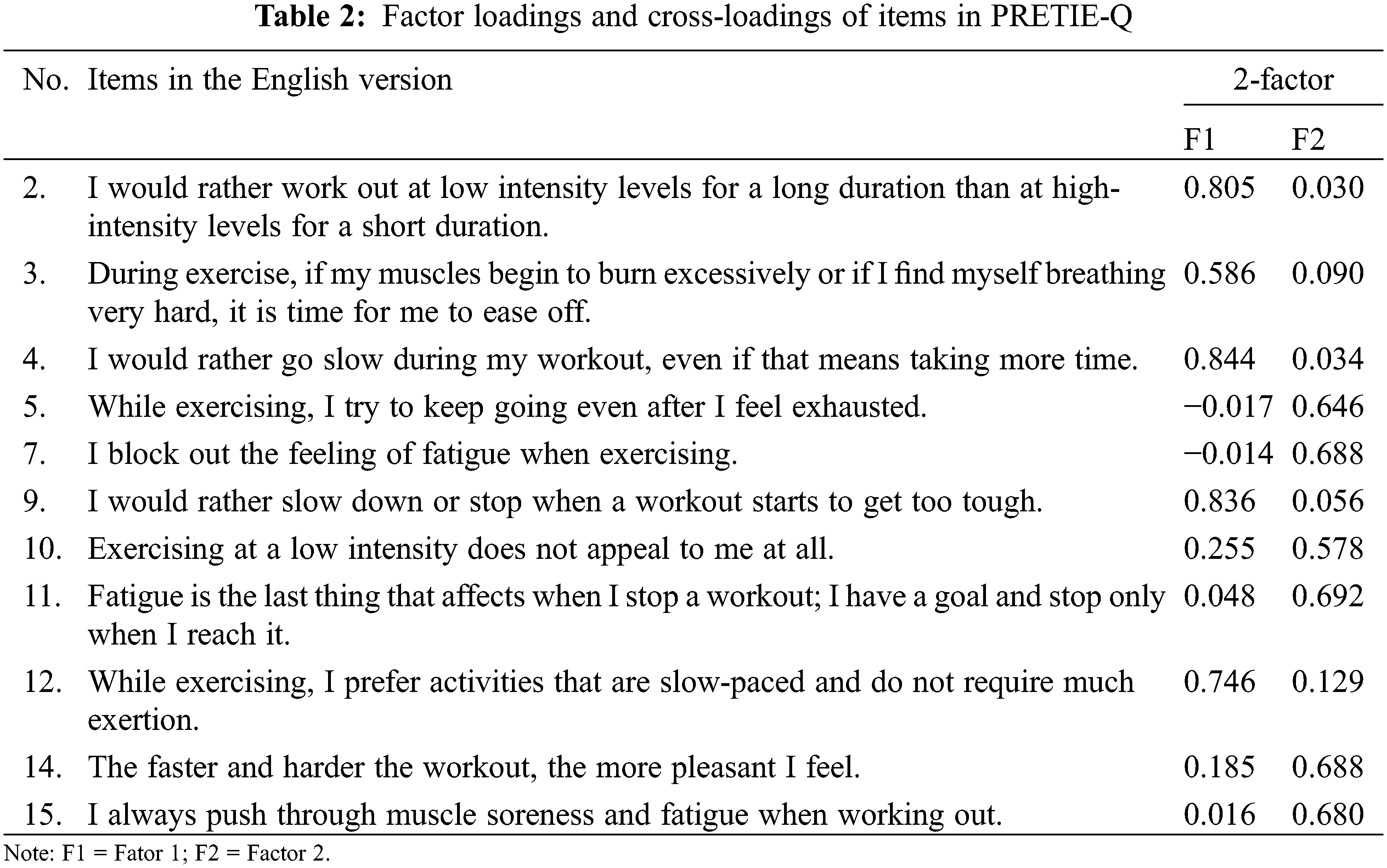
Exploratory factor analysis (Study 1 presented in Table 2): Results from Sample 1 (n= 566) indicated that it is suitable for factor analysis (KMO = 0.806 > 0.80, p< 0.001). Based on the criteria of factor loadings (<0.60) and cross-loadings (>0.15) [37], three items (3, 10, 14) were removed. As a result, a fit model with 8 items (2 factors) was finalized, which was used for subsequent analyses.
Internal consistency (Study 1 with Sample 2 = 551): As shown in Table 3, Cronbach’s α coefficients are presented with 0.85 (Factor 1) and 0.72 (Factor 2), respectively, which indicated a good internal consistency among Chinese college students. In addition, these two factors are significantly correlated with each other (r = −0.15).

Results from the CFA indicated good model fit indices in Table 4 (χ² = 21.612, df= 19, p > 0.05, TLI = 0.997, CFI = 0.998, RMSEA = 0.016, SRMR = 0.024). Finally, an 8-item Chinese-language PRETIE-Q was established with preference (items 2, 4, 9, and 12) and tolerance-related (items 5, 7, 11, and 15) factors. Detailed information is presented in Appendix 1. Test-retest reliability of the Chinese version of the PRETIE-Q was conducted, with intra-class correlation coefficients (ICC) of r= 0.72 (preference, p< 0.01) and r= 0.67 (tolerance, p< 0.01).

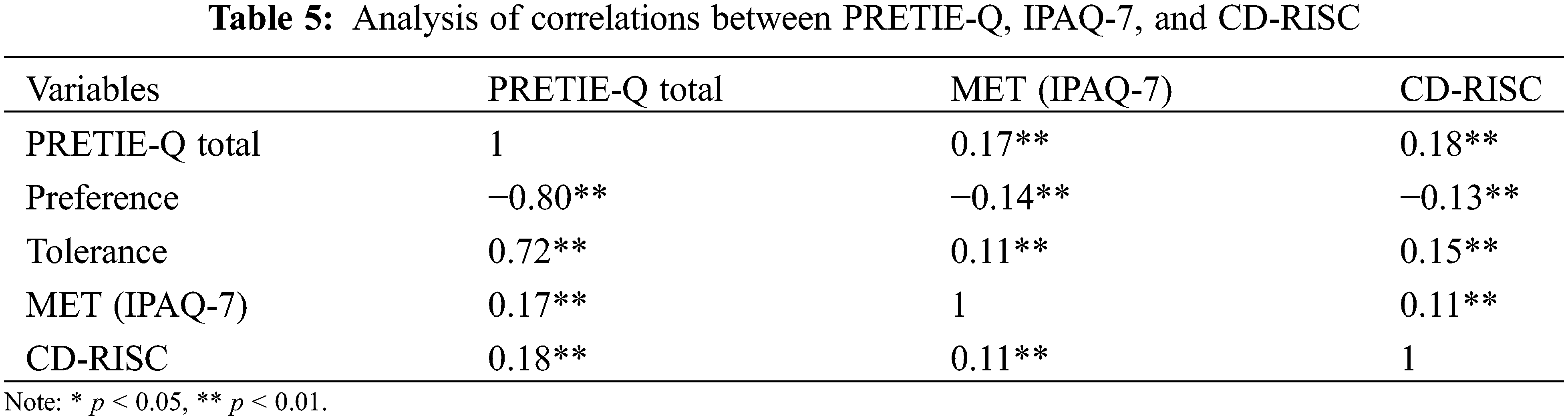
As presented in Table 5, the preference for low exercise intensity was significantly negatively associated with physial activity level expressed by MET (r = −0.14, p< 0.01) and resilience (r = −0.13, p< 0.01). The tolerance of high exercise intensity was positively correlated with physial activity level (r= 0.11, p< 0.01) and resilience (r= 0.15, p< 0.01). Cardiorespiratory fitness was significantly negatively correlated with preference (r = −0.36, p< 0.05) and positively correlated with tolerance (r= 0.34, p< 0.05) in Study 2.
The Preference for and Tolerance of the Intensity of Exercise Questionnaire (PRETIE-Q) has been developed to quantify preference for and tolerance of exercise intensity. Following the translation of the original PRETIE-Q into Chinese, this study determined whether this culturally adapted instrument is valid and reliable among college students who typically spent 10–15 h physically inactive each day (e.g., sitting). Our results indicate that the Chinese version of the PRETIE-Q has good psychometric properties which are indicated by: i) a good internal consistency of the Chinese version of the PRETIE-Q; ii) a good construct validity of the two-factor model from the CFA; iii) good test-retest reliability with ICC in randomly selected 150 participants. In the following, we will discuss our findings in more detail.
Eight items were kept in the Chinese version of the PRETIE-Q, which is different from the original PRETIE-Q consisting of 16 items [22] and other culturally adapted instruments consisting of 10/16 items [26,27]. The removal of five items (1, 6, 8, 13, 16) of the original instrument was due to a shared meaning with other items (evaluated by college students during preliminary data collection and exercise psychologists). The other three items of the original version were removed during EFA because of low factor loadings (Items 3 and 10) or cross-loadings (Item 14). Recently, a validation study [27] was conducted among Portuguese health club exercises, suggesting that the 10-item model had good fit indices, with 5 items in each dimension (preference and tolerance). The removal of a different number of items (in comparison to the original version) may be attributable to cultural differences or other factors such as exercise experience. Particularly, college students being recruited in the present study may have less experience in leisure sports activities as compared with habitual exercisers. Thus, future validation studies in China should consider other cohorts than college students (e.g., habitual exercises, older adults with and without chronic diseases).
Importantly, positive associations between the scores of the dimension tolerance of high-intensity exercise with physial activity level and cardiorespiratory fitness were observed in the current study, which is consistent with the results of previous studies [28,38,39]. Several reasons might explain this observation. First, it is widely accepted that physiologic changes (e.g., in exercise-induced muscle fatigue, lactate accumulation, pain, and cardiovascular and respiratory systems) in the human body swiftly emerge in response to any physical challenge (e.g., hiking, jogging, and exercise training), especially for physically inactive individuals [40]. However, those physiological changes might vary as a function of physial activity level due to adaptations of the organism. For instance, adaptions have been observed to be associated with reduced pain sensitivity [41], and an increased pain threshold (tolerance) [42] allowing individuals to sustain their active movement behavior (physial activity engagement) over extended periods, with more frequent training sessions and greater load. Second, exercisers with relatively high levels of regular physial activity have reported suffering from an over-activation of the reward system and deficient inhibition when they were asked to watch sport-related stimuli, so they are more likely to pursue elevated exercise intensity (tolerance) for perception of pleasure and enjoyment [43].
In addition to the above-mentioned physiological measures (i.e., cardiorespiratory fitness), we also assessed the relationship between the dimensions of the Chinese version of the PRETIE-Q and resilience. Resilience emphasizes an individual’s ability to withstand and recover in the face of stressors and is attributable to top-down processes [44]. In the present study, a positive association between resilience and tolerance of exercise intensity was observed. This finding can be explained as follows: When individuals are physically active (e.g., exercising), the physical activity acts as a stressor that elicits a certain level of physiological changes (e.g., the activation of the hypothalamic–pituitary–adrenal axis leading to the rising cortisol levels) [45] that, in turn, can trigger psychological alterations being related to volatility (e.g., negative emotions such as fatigue). Prolonged physical training results in a higher a higher tolerance against higher exercise intensities due to strengthened emotional regulation and/or improved coping skills [44]. As a result, individuals are able to effectively inhibit the negative emotions occurring at higher exercise intensity as shown by studies that used assessments of brain function (e.g., functional near-infrared spectroscopy (fNIRS)) [46–49].
The present study has several strengths that highlight its contribution to the current literature. Firstly, the validation of a Chinese version of PRETIE-Q addresses the lack of a tool to assess exercise tolerance and preference in this population. Secondly, the sample size used in the current validation study was large and even surpassed the sample size (n= 471) of the validation study of the original scale [22]. Thirdly, the criteria-related validity of the Chinese version of the PRETIE-Q was established using both objective and subjective measures. However, some limitations of the present study still need to be acknowledged. Firstly, as this study focuses on emerging adults, the generalizability of our findings is limited. Further studies are encouraged to address the validity of the PRETIE-Q in other age groups and across different health conditions. Secondly, other psychological variables such as personality, fatigue, self-efficacy, and sleep quality may confound the correlations between two dimensions of the Chinese version of the PRETIE-Q with the regular level of PA, cardiorespiratory fitness, and resilience. As these psychological variables were not measured in the present study, further studies should investigate their (mediating or moderating) influence on the observed relationships.
The findings of the current study which revealed that the Chinese version of the PRETIE-Q has good psychometric properties suggest that our culturally adopted version of the PRETIE-Q is an appropriate tool. assess exercise intensity tolerance and preference in Chinese college students. Furthermore, it was observed that exercise tolerance and preference are associated with the level of regular physical activity, the level of cardiorespiratory fitness, and the level of resilience. Based on our findings suggesting that our Chinese version of the PRETIE-Q is valid and reliable, this study opens a new direction for future studies on exercise-related affective responses in Chinese individuals, although further studies are needed to confirm our findings in other cohorts (e.g., older adults with and without chronic diseases).
Acknowledgement: We would like to thank all volunteers who have participated in this study.
Authors’ Contributions: TW, JK, and LYZ participated in the design of the study, manuscript drafting, data reduction/analysis and the manuscript editing; WT and JK contributed to data collection; ZHZ, FH, AT, SL, AK, LYZ contributed to data reduction/analysis and manuscript editing; SL, LYZ and AK contributed to the interpretation of results and manuscript editing. All authors have approved the final version of the manuscript and agreed with the order of presentation of the authors.
Funding Statement: This study is supported by Start-Up Research Grant of Shenzhen University (20200807163056003) and Start-Up Research Grant (Peacock Plan: 20191105534C).
Conflicts of Interest: All authors declare that they have no conflicts of interest.
References
1. Blair, S. N. (2009). Physical inactivity: The biggest public health problem of the 21st century. British Journal of Sports Medicine, 43, 1–2. DOI 10.1136/bjsm.2009.059360. [Google Scholar] [CrossRef]
2. Anderson, E., Durstine, J. L. (2019). Physical activity, exercise, and chronic diseases: A brief review. Sports Medicine and Health Science, 1, 3–10. DOI 10.1016/j.smhs.2019.08.006. [Google Scholar] [CrossRef]
3. De la Rosa, A., Olaso-Gonzalez, G., Arc-Chagnaud, C., Millan, F., Salvador-Pascual, A. et al. (2020). Physical exercise in the prevention and treatment of Alzheimer’s disease. Journal of Sport and Health Science, 9, 394–404. DOI 10.1016/j.jshs.2020.01.004. [Google Scholar] [CrossRef]
4. Jung, M., Zou, L., Yu, J. J., Ryu, S., Kong, Z. (2020). Does exercise have a protective effect on cognitive function under hypoxia? A systematic review with meta-analysis. Journal of Sport and Health Science, 9, 562–577. DOI 10.1016/j.jshs.2020.04.004. [Google Scholar] [CrossRef]
5. Simper, T. N., Morris, C., Lynn, A., O’Hagan, C., Kilner, K. (2020). Responses to oral glucose challenge differ by physical activity volume and intensity: A pilot study. Journal of Sport and Health Science, 9, 645–650. DOI 10.1016/j.jshs.2017.04.010. [Google Scholar] [CrossRef]
6. Rodriguez-Ayllon, M., Acosta-Manzano, P., Coll-Risco, I., Romero-Gallardo, L., Borges-Cosic, M., et al. (2021). Associations of physical activity, sedentary time, and physical fitness with mental health during pregnancy: The GESTAFIT project. Journal of Sport and Health Science, 10, 379–386. DOI 10.1016/j.jshs.2019.04.003. [Google Scholar] [CrossRef]
7. Cayon, A. (2016). PAHO WHO Global recommendations on physical activity for health. [Google Scholar]
8. Keating, X. D., Guan, J., Bridges, D. M. (2005). A meta-analysis of college students’ physical activity behaviors. Journal of American College Health, 54, 116–126. DOI 10.3200/JACH.54.2.116-126. [Google Scholar] [CrossRef]
9. Brand, R., Ekkekakis, P. (2018). Affective–reflective theory of physical inactivity and exercise. German Journal of Exercise and Sport Research, 48, 48–58. DOI 10.1007/s12662-017-0477-9. [Google Scholar] [CrossRef]
10. O’Connor, P., Buckworth, J., Dishman, R., Tomporowski, P. (2014). Exercise psychology, 2nd Edition. In: Medicine & science in sports & exercise, 46, 2037. DOI 10.1249/MSS.0000000000000454. [Google Scholar] [CrossRef]
11. Radel, R., Pelletier, L., Pjevac, D., Cheval, B. (2017). The links between self-determined motivations and behavioral automaticity in a variety of real-life behaviors. Motivation and Emotion, 41, 443–454. DOI 10.1007/s11031-017-9618-6. [Google Scholar] [CrossRef]
12. Sperandei, S., Vieira, M. C., Reis, A. C. (2016). Adherence to physical activity in an unsupervised setting: Explanatory variables for high attrition rates among fitness center members. Journal of Science & Medicine in Sport, 19, 916–920. DOI 10.1016/j.jsams.2015.12.522. [Google Scholar] [CrossRef]
13. Kikuga, N., Fukushima, N., Sawada, S., Matsushita, M., Gando et al. (2021). Associations between psychological attitudes toward exercise and fitness club membership resignation among new members: A cohort study. Japanese Journal of Public Health, 68, 230–240. DOI 10.11236/jph.20-053. [Google Scholar] [CrossRef]
14. Richardson, D. L., Duncan, M. J., Jimenez, A., Juris, P. M., Clarke, N. D. (2020). Affective responses to supervised 10-week programs of resistance exercise in older adults. Journal of Sport and Health Science, 9, 604–613. DOI 10.1016/j.jshs.2019.01.006. [Google Scholar] [CrossRef]
15. Ekkekakis, P. (2013). Redrawing the model of the exercising human in exercise prescriptions. In: Lifestyle medicine, Second EditionAbingdon, England: Talor & Francis. DOI 10.1201/b13781-141. [Google Scholar] [CrossRef]
16. de Geus, E. J. C., de Moor, M. H. M. (2008). A genetic perspective on the association between exercise and mental health. Mental Health and Physical Activity, 1, 53–61. DOI 10.1016/j.mhpa.2008.09.005. [Google Scholar] [CrossRef]
17. Dafermos, P. E. M. (2012). Exercise is a Many-splendored thing, but for some it does not feel so splendid: Staging a resurgence of hedonistic ideas in the quest to understand exercise behavior. The Oxford Handbook of Exercise Psychology. [Google Scholar]
18. Teques, P., Calmeiro, L., Silva, C., Borrego, C. (2020). Validation and adaptation of the Physical Activity Enjoyment Scale (PACES) in fitness group exercisers. Journal of Sport and Health Science, 9 (4), 352–357. DOI 10.1016/j.jshs.2017.09.010. [Google Scholar] [CrossRef]
19. Ekkekakis, P., Hargreaves, E. A., Parfitt, G. (2013). Invited guest editorial: Envisioning the next fifty years of research on the exercise–affect relationship. Psychology of Sport and Exercise, 14, 751–758. DOI 10.1016/j.psychsport.2013.04.007. [Google Scholar] [CrossRef]
20. Ekkekakis, P. (2003). Pleasure and displeasure from the body: Perspectives from exercise. Cognition and Emotion, 17, 213–239. DOI 10.1080/02699930302292. [Google Scholar] [CrossRef]
21. Ekkekakis, P., Parfitt, G., Petruzzello, S. J. (2001). The pleasure and displeasure people feel when they exercise at different intensities: Decennial update and progress towards a tripartite rationale for exercise intensity prescription. Sports Medicine, 41, 641–671. DOI 10.2165/11590680-000000000-00000. [Google Scholar] [CrossRef]
22. Ekkekakis, P., Hall, E. E., Petruzzello, S. J. (2005). Some like it vigorous: Measuring individual differences in the preference for and tolerance of exercise intensity. Journal of Sport and Exercise Psychology, 27, 350–374. DOI 10.1123/jsep.27.3.350. [Google Scholar] [CrossRef]
23. Ekkekakis, P., Hall, E. E., Petruzzello, S. J. (2005). Variation and homogeneity in affective responses to physical activity of varying intensities: An alternative perspective on dose–response based on evolutionary considerations. Journal of Sports Sciences, 23, 477–500. DOI 10.1080/02640410400021492. [Google Scholar] [CrossRef]
24. Williams, D. M. (2008). Exercise, affect, and adherence: An integrated model and a case for self-paced exercise. Journal of Sport & Exercise Psychology, 30, 471–496. DOI 10.1123/jsep.30.5.471. [Google Scholar] [CrossRef]
25. Ladwig, M. A., Hartman, M. E., Ekkekakis, P. (2017). Affect-based exercise prescription: An idea whose time has come? ACSM’s Health & Fitness Journal, 21, 10–15. DOI 10.1249/FIT.0000000000000332. [Google Scholar] [CrossRef]
26. Smirmaul, B. P. C., Ekkekakis, P., Teixeira, I. P., Nakamura, P. M., Kokubun, E. (2015). Preference for and tolerance of the intensity of exercise questionnaire: Brazilian Portuguese version. Revista Brasileira de Cineantropometria & Desempenho Humano, 17(5). [Google Scholar]
27. Teixeira, D. S., Ekkekakis, P., Andrade, A., Rodrigues, F., Evmenenko, A. et al. (2021). Preference for and tolerance of the intensity of exercise questionnaire (PRETIE-QValidity, reliability and gender invariance in Portuguese health club exercisers. Current Psychology. DOI 10.1007/s12144-021-01718-3. [Google Scholar] [CrossRef]
28. Hall, E. E., Petruzzello, S. J., Ekkekakis, P., Miller, P. C., Bixby, W. R. (2014). Role of self-reported individual differences in preference for and tolerance of exercise intensity in fitness testing performance. The Journal of Strength & Conditioning Research, 28, 2443–2451. DOI 10.1519/JSC.0000000000000420. [Google Scholar] [CrossRef]
29. Schneider, M. L., Graham, D. J. (2009). Personality, physical fitness, and affective response to exercise among adolescents. Medicine & Science in Sports & Exercise, 41, 947–955. DOI 10.1249/MSS.0b013e31818de009. [Google Scholar] [CrossRef]
30. Craig, C. L., Marshall, A. L., Sjstrm, M., Bauman, A. E., Booth, M. L. et al. (2003). International physical activity questionnaire: 12-country reliability and validity. Medicine & Science in Sports & Exercise, 35, 1381–1395. DOI 10.1249/01.MSS.0000078924.61453.FB. [Google Scholar] [CrossRef]
31. Patterson, E. (2005). Guidelines for data processing and analysis of the international physical activity questionnaire (IPAQ)-short and long forms. http://www.ipaq.ki.se/scoring.pdf. [Google Scholar]
32. Macfarlane, D. J., Lee, C. C., Ho, E. Y., Chan, K. L., Chan, D. T. (2007). Reliability and validity of the Chinese version of IPAQ (short, last 7 days). Journal of Science and Medicine in Sport, 10, 45–51. DOI 10.1016/j.jsams.2006.05.003. [Google Scholar] [CrossRef]
33. Connor, K. M., Davidson, J. (2003). Development of a new resilience scale: The connor-davidson resilience scale (CD-RISC). Depression and Anxiety, 18, 76–82. DOI 10.1002/(ISSN)1520-6394. [Google Scholar] [CrossRef]
34. Herrman, H., Stewart, D. E., Diaz-Granados, N., Berger, E. L., Jackson, B. et al. (2001). What is resilience? Canadian Journal of Psychiatry, 56, 258–265. DOI 10.1177/070674371105600504. [Google Scholar] [CrossRef]
35. Yu, N. X., Zhang, J. (2007). Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Social Behavior and Personality: An International Journal, 35, 19–30. DOI 10.2224/sbp.2007.35.1.19. [Google Scholar] [CrossRef]
36. Xu, Y., Zhou, R., Fu, C. (2016). Reliability and validity of the Connor-Davidson Resilience Scale (CD-RISC) in Chinese college students. China Journal of Health Psychology, 4. DOI 10.13342/j.cnki.cjhp.2016.06.026. [Google Scholar] [CrossRef]
37. Jr, J., Black, W. C., Babin, B. J., An de Rson, R. E. (2009). Multivariate data analysis (Global Edition). Switzerland: Pearson Schweiz Ag. [Google Scholar]
38. Ekkekakis, P., Thome, J., Petruzzello, S. J., Hall, E. E. (2008). The preference for and tolerance of the intensity of exercise questionnaire: A psychometric evaluation among college women. Journal of Sports Sciences, 26, 499–510. DOI 10.1080/02640410701624523. [Google Scholar] [CrossRef]
39. Ekkekakis, P., Lind, E., Hall, E. E., Petruzzello, S. J. (2007). Can self-reported tolerance of exercise intensity play a role in exercise testing? Medicine & Science in Sports & Exercise, 39, 1193–1199. DOI 10.1249/mss.0b013e318058a5ea. [Google Scholar] [CrossRef]
40. Mendonca, G. (2008). Physiological responses and long-term adaptations to exercise: Exercise training, functional capacity, body composition, maximum dynamic strength, exercise economy, electrodermal activity, energy expenditure and anthropometric measurements in individuals with down syndrome. [Google Scholar]
41. Zheng, K., Chen, C., Yang, S., Wang, X. (2021). Aerobic exercise attenuates pain sensitivity: An event-related potential study. Frontiers in Neuroscience, 15, 735470. DOI 10.3389/fnins.2021.735470. [Google Scholar] [CrossRef]
42. Jones, M. D., Booth, J., Taylor, J. L., Barry, B. K. (2014). Aerobic training increases pain tolerance in healthy individuals. Medicine & Science in Sports & Exercise, 46, 1640–1647. DOI 10.1249/mss.0000000000000273. [Google Scholar] [CrossRef]
43. Huang, Q., Huang, J., Chen, Y., Lin, D., Xu, S. (2019). Overactivation of the reward system and deficient inhibition in exercise addiction. Medicine and Science in Sports and Exercise, 51, 1918–1927. DOI 10.1249/MSS.0000000000001988. [Google Scholar] [CrossRef]
44. Belcher, B. R., Zink, J., Azad, A., Campbell, C. E., Chakravartti, S. P. (2021). The roles of physical activity, exercise, and fitness in promoting resilience during adolescence: Effects on mental well-being and brain development. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 6(2), 225–237. DOI 10.1016/j.bpsc.2020.08.005. [Google Scholar] [CrossRef]
45. Caplin, A., Chen, F. S., Beauchamp, M. R., Puterman, E. (2021). The effects of exercise intensity on the cortisol response to a subsequent acute psychosocial stressor. Psychoneuroendocrinology, 131, 105336. DOI 10.1016/j.psyneuen.2021.105336. [Google Scholar] [CrossRef]
46. Tempest, G. D., Eston, R. G., Parfitt, G. (2014). Prefrontal cortex haemodynamics and affective responses during exercise: A multi-channel near infrared spectroscopy study. PLoS One, 9, e95924. DOI 10.1371/journal.pone.0095924. [Google Scholar] [CrossRef]
47. Tempest, G., Parfitt, G. (2016). Self-reported tolerance influences prefrontal cortex hemodynamics and affective responses. Cognitive, Affective, & Behavioral Neuroscience, 16, 63–71. DOI 10.3758/s13415-015-0374-3. [Google Scholar] [CrossRef]
48. Tempest, G., Parfitt, G. (2013). Imagery use and affective responses during exercise: An examination of cerebral hemodynamics using near-infrared spectroscopy. Journal of Sport and Exercise Psychology, 35, 503–513. DOI 10.1123/jsep.35.5.503. [Google Scholar] [CrossRef]
49. Jones, L., Ekkekakis, P. (2019). Affect and prefrontal hemodynamics during exercise under immersive audiovisual stimulation: Improving the experience of exercise for overweight adults. Journal of Sport and Health Science, 8, 325–338. DOI 10.1016/j.jshs.2019.03.003. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools