
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE
Age-trends in Cognitive Function and Quality of Life: Sex Differences in a Community Population in Taiwan
1 Department of Psychiatry, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, 000800, Taiwan
2 Department of Post-Baccalaureate Medicine, National Sun Yat-Sen University, Kaohsiung, Taiwan
3 College of Humanities and Social Sciences, National Pintung University of Science and Technology, Pingtung, Taiwan
4 Department of Child and Adolescent Psychiatry, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, 000800, Taiwan
* Corresponding Author: Liang-Jen Wang. Email:
International Journal of Mental Health Promotion 2022, 24(6), 989-998. https://doi.org/10.32604/ijmhp.2022.022784
Received 25 March 2022; Accepted 06 July 2022; Issue published 28 September 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Population aging has developed into a significant area of concern in developed countries, especially in relation to the preservation of functional independence and the quality of life (QoL). However, information on the contribution of sex differences in quality of life and cognitive function is scarce. Therefore, this study aimed to investigate potential differences in cognitive function and QoL between males and females. For this study, we recruited 382 healthy subjects aged 19–79 years from communities in Southern Taiwan. Cognitive function and QoL were assessed using the UCSD Performance-based Skills Assessment, Brief Version (UPSA-B) and World Health Organization Quality of Life Instruments (WHOQOL-BREF), respectively. The effects of sex, age groups, and interaction of sex and age on the UPSA-B and WHOQOL-BREF scores were examined. We found that the financial and communication domains of the UPSA-B showed declining trends with age in both sexes, although these trends were more obvious in females than in males. In the domain of Physical Capacity, QoL showed an age-increased trend in males, while QoL in the Environment domain showed an age-increased trend in females. Regarding the relationships between cognitive function and QoL, we found that the financial skill and communication skill of UPSA-B was positively correlated to the psychological well-being domain of WHOQOL-BREF, in males of age <40 years. In conclusion, our findings demonstrate differential relationships between cognitive function and QoL between males and females, which could serve as a basis for further study between cognitive function and quality of life in communities.Keywords
Nomenclature
| QoL | Quality of life |
| UPSA-B | UCSD Performance-based Skills Assessment, Brief Version |
| WHOQOL-BREF | World Health Organization Quality of Life Instruments |
| WHO | World Health Organization |
| DSM-IV | Diagnostic and Statistical Manual of Mental Disorders, fourth edition |
| MINI | Mini International Neuropsychiatric Interview |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, fifth edition |
Over the past few decades, population aging has become a global phenomenon, with several countries having already become super-aged societies (with individuals aged 65 and above representing more than 20% of the population) [1]. Taiwan became an aged society in 2018 and is expected to become a super-aged society in 2025 [2]. As life expectancy increases, the preservation of functional independence will play an important role in quality of late-life and medical expenditures [3]. During the aging process, the severity of cognitive impairment may affect one’s capacity to accomplish daily routines and to live independently [4]. Therefore, a growing number of studies have been focusing on the relationship between cognitive function and biological and psychosocial factors [5–7].
Compelling evidence has shown that females are at a higher risk of cognitive disorders (e.g., Alzheimer’s disease) than males [8], which may be due to the longer life expectancy of females [9]. A large-scale cohort study in the U.S. suggested that women may have greater cognitive reserve but faster cognitive decline than men, which may contribute to sex differences in late-life dementia [10]. Our previous study, it demonstrated that the correlation between neurosteroids and cognitive function and psychological well-being may differ with sex [11]. Therefore, the uncertain mechanisms of the sex-specific effect on cognition and quality of life warrant further clarification. To collect more data about how cognitive function affects the performance of human beings, we chose the UCSD Performance-based Skills Assessment, Brief Version (UPSA-B) as our assessment tool [12]. This modified brief version of UPSA, which was developed to assess daily functioning in individuals with mental disorders.
In addition to cognitive function, we adopted QoL scales to measure quality of life in later life. The World Health Organization (WHO) defines quality of life as an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns [13]. Previous research has shown differences between QoL and sex, as well as ages, and these results are supposed to reflect the discrepancy between each group of people [13–15]. We herein chose World Health Organization Quality of Life Instruments (WHOQOL-BREF) assessment, which divides QoL into physical, psychological, social, and environmental domains [13], to evaluate the biological factors, behavioral factors, and socioeconomic inequities existing between populations.
Therefore, we hypothesize that cognitive function and QoL exhibit differential trends between males and females along with age. The aims of this study were to examine trends of cognitive function and QoL trends along with age between sex; as well as to investigate whether there are differential relationships exist between cognitive function and QoL between males and females.
This cross-sectional study was conducted in Chang Gung Memorial Hospital, and was approved by the respective Institutional Review Board (IRB No: 103-6849C). The participants consisted of healthy individuals recruited from the staff of Kaohsiung Chang Gung Memorial Hospital and Keelung Chang Gung Memorial Hospital, and from community volunteers in Kaohsiung City and Keelung City, Taiwan. The recruitment criteria were: (1) age ≥18 years; (2) without a history of major psychiatric disorders (e.g., psychosis, bipolar disorder, major depressive disorder, organic mental disorders, and substance use disorder) confirmed using the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria and the Chinese Version of the Mini International Neuropsychiatric Interview (MINI) [16,17]; (3) without any known systemic or neurological diseases that would influence cognitive performance; and (4) capacity to speak Mandarin read Chinese and give informed consent. In total, we recruited 382 healthy subjects aged 19–79 years (mean age: 48.0 ± 16.7 years; 47.6% male; education level: 52.6% were college or above).
The UPSA-B, a brief modified brief version of UPSA, was developed to assess daily functioning in individuals with mental disorders [12]. The UPSA-B is made up of two subtests: the financial portion and the communication domain. In the financial portion, participants are required to count out specific amounts of real currency, make change, and request a bank check to pay a bill. Meanwhile, the communication domain asks participants to correctly call directory assistance to obtain a telephone number to reschedule an appointment in a hospital. Three sub-scores are derived from the UPSA-B: financial skill 1 (counting money and making change), financial skill 2 (paying a bill), and communication skill (dialing a telephone number and calling to reschedule an appointment) [18]. The validity of the Chinese version of the UPSA-B has been established in Mandarin-speaking patients with mental illnesses [19,20].
2.3 Quality of Life Assessment
The WHOQOL-BREF, a self-administered questionnaire by respondents, is a 26-item version of the WHOQOL-100 assessment tool. All items were rated on a 5-point scale with a higher score indicating a higher quality of life. The WHOQOL-BREF has proven useful in surveys of general and specific populations, as well as in differentiating the health benefits produced by a wide range of different treatments [21]. It was scored over four domains: Physical Capacity (7 items), Psychological Well-being (6 items), Social Relationship (4 items), and Environment (9 items). The Physical Capacity domain consists of such items as energy, pain, sleep, mobility, and daily functional activities. The Psychological Well-being domain covers self-image, self-esteem and attitudes, memory concentration, learning ability, religion, and mental status. The Social Relationship domain measures questions related to personal relationships, social support, and sex life. The Environment domain includes issues related to safety, health and social services, living physical environment, opportunities to acquire new skills and knowledge, financial resources, recreation, and transportation [22]. The WHOQOL-BREF has been reported to have good test-retest reliability and content validity in Taiwan [23].
Data were analyzed using the statistical software package SPSS (Version 21.0; SPSS Inc., Chicago, IL, USA). The variables are shown as either mean (±SD) or frequency (%). Categorical variables among age groups were compared using the chi-square test. In a two-tailed test, a p-value < 0.05 was considered statistically significant.
We then stratified our normative sample was stratified into three age groups (<40 years; 40–59 years; and ≥60 years) [24] and sex groups. Two-way analysis of covariance (ANCOVA) was adopted to evaluate the potential effects of sex and age group on UPSA-B and WHOQOL scores, controlling for education levels (covariate). The raw scores from UPSA-B (two domains) and WHOQOL (four domains) were set as dependent variables in each model. We used post-hoc tests with LSD to examine the differences in UPSA-B or WHOQOL between specific age groups. Effect sizes were demonstrated using the partial eta-squared (η2). Finally, partial correlation was used to examine the relationships between UPSA-B and WHOQOL variables, controlling for the effects of education levels.
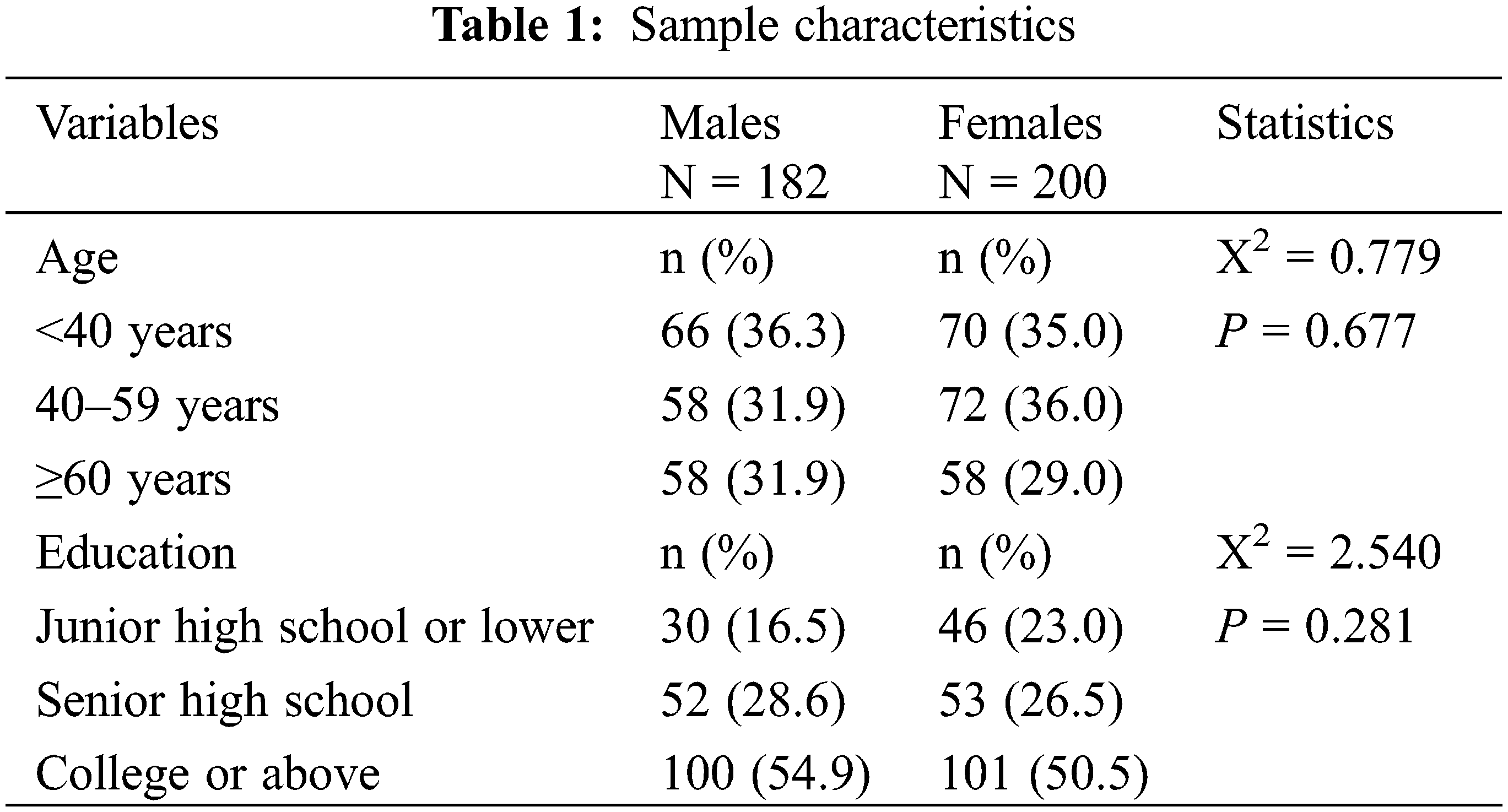
A total of 182 male (mean age: 47.8 ± 16.9 years) and 200 female (mean age: 48.0 ± 16.5 years) participants were recruited in this study. The distributions of sex, age groups, and educational levels of the participants are summarized in Table 1. Of males, 36.3%, 31.9% and 31.9% were aged <40 years, 40–59 years, and ≥60 years, respectively. Of females, 35%, 36%, and 29% were aged <40 years, 40–59 years, and ≥60 years, respectively. We found no significant differences in distribution of age groups and educational levels between males and females were found.
The UPSA-B performance of the three age groups in males and females are demonstrated in Fig. 1. We found that the financial domain of the UPSA-B (Fig. 1A) showed age-declined trends both in males (F(2, 182) = 4.638, η2 = 0.050, p = 0.011) and females (F(2, 200) = 14.463, η2 = 0.13, p < 0.001). The age-declining trends were more obvious in females than in males. The post-hoc tests showed that in males, the financial skills among those aged ≥60 years were significantly lower than those aged <40 years (mean difference = −1.58, p < 0.001) or 40–59 years (mean difference = −1.60, p < 0.001), respectively. In females, the same skills among those aged ≥60 years were significantly lower than those aged <40 years (mean difference = −2.92, p < 0.001) or 40–59 years (mean difference = −2.39, p < 0.001), respectively. Furthermore, the financial skills among those aged 40–59 years were significantly lower than those aged <40 years (mean difference = −0.53, p = 0.031).
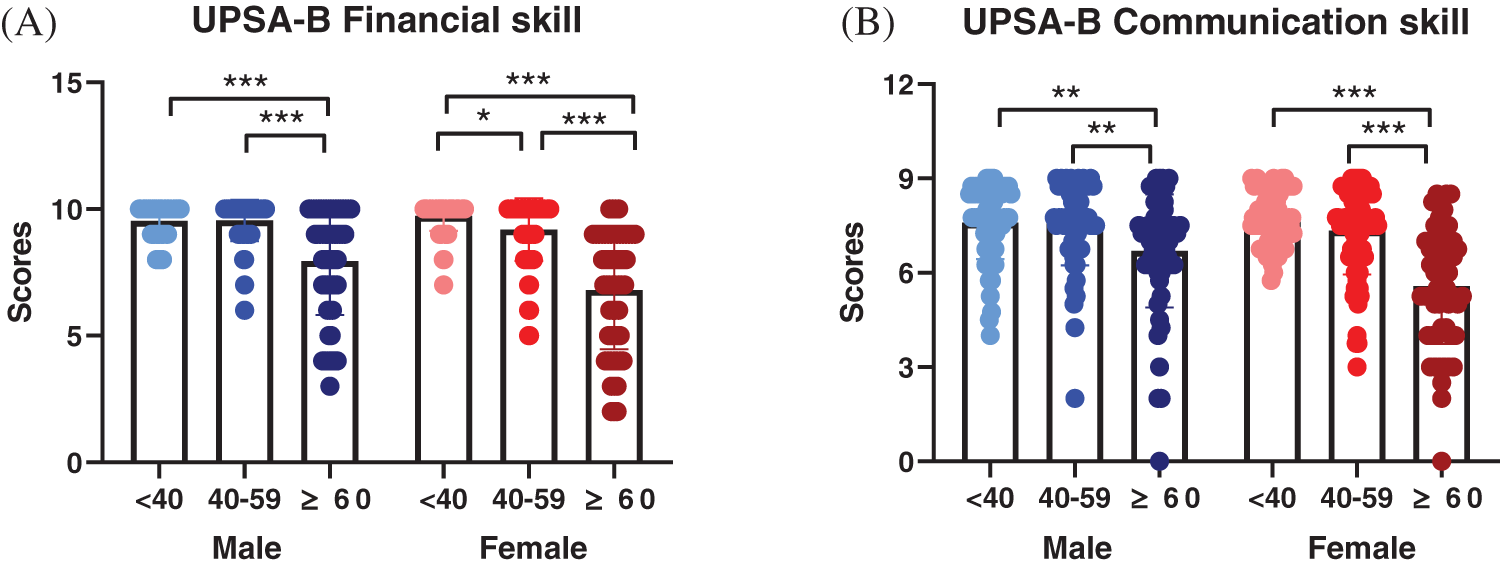
Figure 1: The two domains (financial skill and communication skill) of the UCSD Performance-based Skills Assessment, Brief Version (UPSA-B) across three age groups (<40 years; 40–59 years; and ≥60 years) in males and females. (A) UPSA-B financial skill: assessing daily functioning in individuals’ financial skill; the higher scores represent better performance (B) UPSA-B communication skill: assessing daily functioning in individuals’ communication skill; the higher scores represent better performance. *p < 0.05, **p < 0.01, ***p < 0.001 of between group comparisons
For the communication domain of the UPSA-B (Fig. 1B), females (F(2, 200) = 8.503, η2 = 0.080, p < 0.001) exhibited age-declined trends. No significant age-declining trend was observed in males (F(2, 182) = 2.017, η2 = 0.022, p = 0.136). In males, the communication skills among those aged ≥60 years were significantly lower than those aged <40 years (mean difference = −0.90, p = 0.001) or 40–59 years (mean difference = −0.87, p = 0.001), respectively. In females, the communication skills among those aged ≥60 years were significantly lower than those aged <40 years (mean difference = −2.14, p < 0.001) or 40–59 years (mean difference = −1.77, p < 0.001), respectively.
The distribution of WHOQOL (Physical Capacity, Psychological Well-being, Social Relationship, and Environment) across the three age groups in males and females are illustrated in Fig. 2. We found that the QoL in Physical Capacity (Fig. 2A) showed an age-increased trend in males only (F(2, 182) = 4.034, η2 = 0.044, p = 0.019). In males, the Physical Capacity among those aged <40 years were significantly lower than those aged 40–59 years (mean difference = −1.25, p = 0.010) and aged ≥60 years (mean difference = −1.28, p = 0.008), respectively. No significant age-changed trends were observed in the Psychological Well-being (Fig. 2B) domain among males. For the Social Relationship domain (Fig. 2C), those aged <40 years were significantly lower than those aged 40–59 years (mean difference = −0.76, p = 0.043). For the Environment domain (Fig. 2D), those aged <40 years were significantly lower than those aged ≥60 years (mean difference = −1.70, p = 0.027).
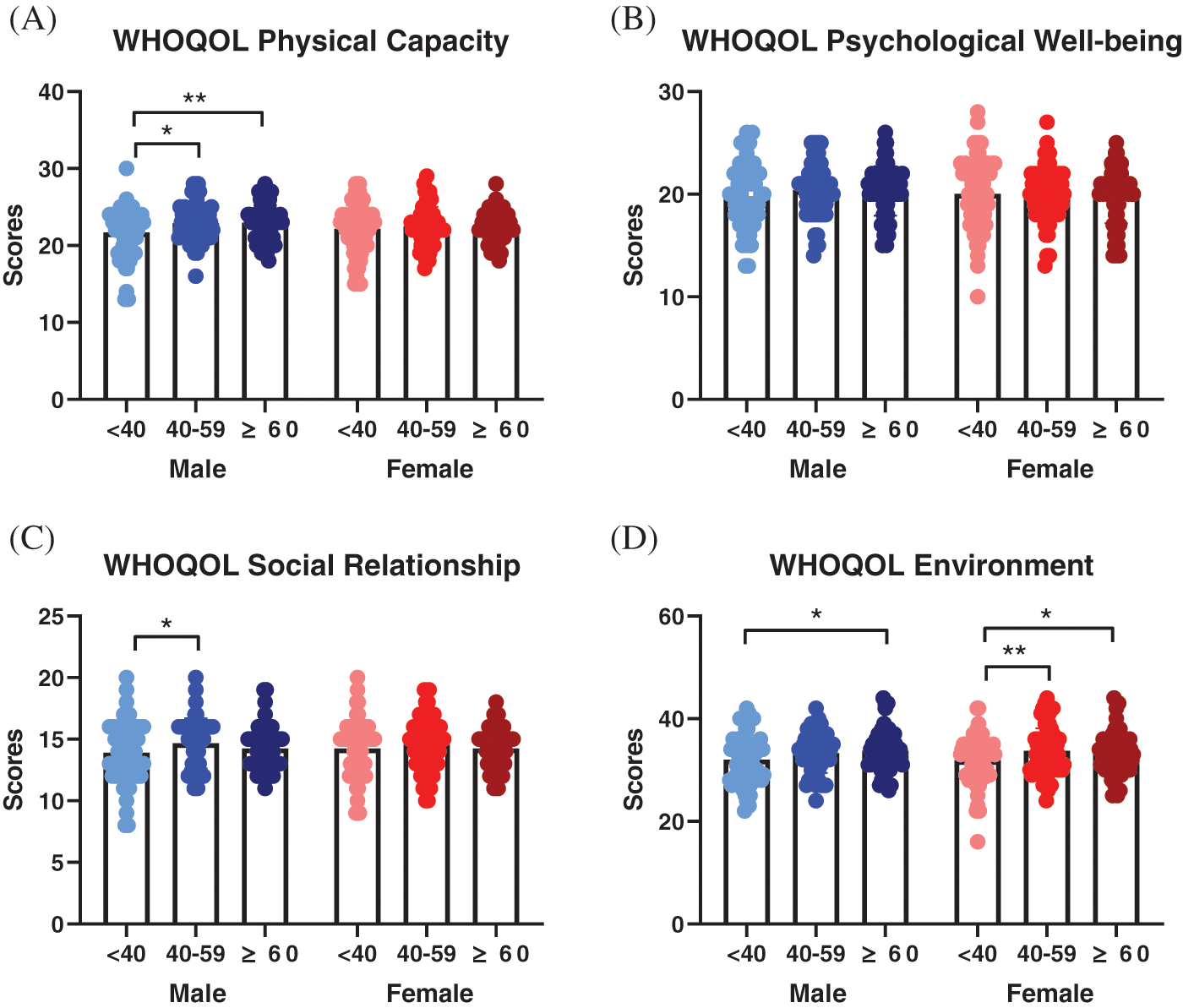
Figure 2: The four domains of WHOQOL (Physical Capacity, Psychological Well-being, Social Relationship, and Environment) across three age groups (<40 years; 40–59 years; and ≥60 years) in males and females. (A) The Physical Capacity domain contains items on energy, pain, sleep, mobility, and daily functional activities. (B) The Psychological Well-being domain covers includes self-image, self-esteem and attitudes, memory concentration, learning ability, religion, and the mental status. (C) The Social Relationship domain measures questions on personal relationships, social support, and sex life. (D) The Environment domain includes covers issues related to safety, health and social services, living physical environment, opportunities to acquire new skills and knowledge, financial resources, recreation, and transportation. The higher scores represent better quality of life. *p < 0.05, **p < 0.01 of between group comparisons
In females, the QoL in the Environment domain (Fig. 2D) showed an age-increased trend in females only (F(2, 200) = 4.333, η2 = 0.043, p = 0.014). The Environment scores among those aged <40 years were significantly lower than those aged 40–59 years (mean difference = −2.25, p = 0.006) and aged ≥60 years (mean difference = −1.85, p = 0.032) in females, respectively. No significant age-changed trends were observed in Physical Capacity, Psychological Well-being, or Social Relationship domains among females.
For the relationships between cognitive function and QoL, we found the financial skills (r = 0.251, p = 0.044) and communication skills (r = 0.350, p = 0.004) of UPSA-B were positively correlated to Psychological Well-being of WHOQOL in males with age <40 years. However, we observed no significant correlation between the performance of UPSA-B and any domains of WHOQOL (Physical Capacity, Psychological Well-being, Social Relationship, and Environment) in females or in the other age groups of males.
The main findings in this study are listed below. First, the age-declining trends of both the financial and the communication domain of the UPSA-B were more obvious in females than in males. Second, the QoL in Physical Capacity showed age-increased trend in males only, while the QoL in the Environment domain showed age-increased trend in only females. Third, for the relationships between cognitive function and QoL, we found that the financial skills and communication skills of UPSA-B were positively correlated to Psychological Well-being of WHOQOL in males with age <40 years, while the financial skills of UPSA-B were positively correlated to only the Environment domain of WHOQOL in females.
The finding of declining scores of financial and communication domains of the UPSA-B related to aging is not surprising, as it confirms what previous researchers have discovered about normal aging [5,6]. Nevertheless, our results showed that both of the age-declining trends were more obvious in females than in males. We supposed that educational level might play a role in cognitive function. In previous research, compared to patients of dementia without formal education, patients with formal education seem to have less frequent disability status [25]. In Taiwan, women have traditionally had fewer educational opportunities than men during the past several decades, that is, until the implementation of nine-year compulsory education in 1968. The historical disparities in access to education between men and women may produce cohort effects [26]. Therefore, we adjusted for education levels in the analyses. Nevertheless, sex-different age-declining trends in cognition were still observed among our study population. With regard to the biological aspect, a previous study revealed that the serum levels of preg–nenolone levels were positively correlated with cognitive function among men [11]. In women, cognitive alterations in a number of domains after menopause, including attention and processing speed [27], as well as decline of estradiol after menopause, represented a significant factor along with age in women [28,29].
The QoL in Physical Capacity showed an age-increased trend in males only, and the QoL in the Environment domain showed an age-increased trend in females. Generally, in Chinese culture, people are more reluctant to express or discuss their feelings than those in Western countries [30]. Instead, expression of multiple medically unexplained somatic symptoms, including fatigue, insomnia, loss of appetite and gastro-intestinal problems, is more acceptable in Chinese culture [30,31], and these presentations are corresponded to the questionnaire within the QoL in Physical Capacity. Therefore, any of the above reasons may lead to responder bias and may ultimately influence our results.
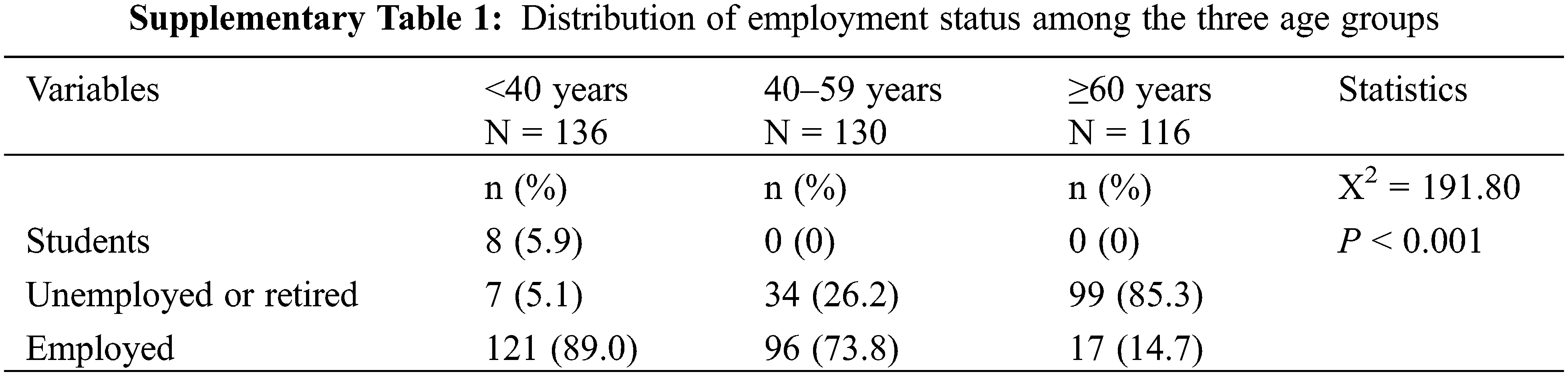
Regarding employment distribution, the rates of being employed among the three age groups (<40 years, 40–59 years and ≥60 years) among our study population were 89%, 73.8%, and 14.7%, respectively (Table S1). Furthermore, the groups aged <40 years and 40–59 years were still the breadwinners of their families, while the group aged >60 years had started to enjoy retirement. During the 1960s to the 1980s, Taiwan experienced economic development, followed by the Feminism movement. Women with age >60 years may have had more chances to notice the improvements to their environment in their later lives.
Both the financial skills and communication skills of UPSA-B were positively correlated to Psychological Well-being of WHOQOL in males with age <40 years. Since the opportunity to receive education and improve circumstances may be unequal between different age and sex groups, education levels were adjusted in our analyses. In most research, cognitive function is now considered to have a positive correlation with quality of life in most of the research [32,33] and many more studies are also trying to determine the relationship between quality of life and diseases with cognitive dysfunction, as well as normal aging [33–35]. However, cognitive function may still decline during aging [36], which may explain why the financial skills and communication skills of UPSA-B had no correlation with Psychological Well-being of WHOQOL in the participants in the other two groups.
Our approach has several limitations of our approach. First, this study was conducted with a cross-sectional design. The age-trends of cognition and QoL were not verified through prospective observation. Second, the diagnosis of minor neurocognitive disorders was included in DSM-5, but screening through DSM-IV may not distinguish people with minor neurocognitive disorders from our sample. Third, the economic status and social environment in Taiwan has progressed rapidly in recent decades [37]. The opportunity to receive an education and improve circumstance might be unequal among different age and sex groups. Fourth, cognitive function was only assessed using the UPSA-B, which is designed for evaluating financial and communication function for individuals with mental disorders [12], and it may be not sensitive enough to detect tiny differences in functional capacity among healthy subjects. Therefore, this study may not have captured comprehensive cognitive profiles among healthy populations in the real world.
Despite its limitations, the results of this study demonstrate differential relationships between cognitive function and QoL between males and females. The findings of our study can serve as a reference for the relationship between cognitive function and quality of life. In the future, sex specific strategies should be considered to enhance psychological wellbeing for sex-specific groups in community populations.
Acknowledgement: The authors express their deepest gratitude to Dr. Jin Fan for granting us the use of the Chinese version of the UPSA-B. We also thank Joanne Lo for helping participant recruitment, and thank all of the individuals who participated in this study.
Authorship: The authors confirm contribution to the paper as follows: conceptualization: YCH, LJW; Methodology: YCH, CFH; Project administration: YCH, LJW, CFH; Formal analysis: YCH, LJW; Investigation: SYW; Resources: YCH, LJW; Writing—Original Draft: SYW; Writing—Review & Editing: LJW; Supervision: CFH. SYW and YCH are cofirst authors and contributed equally to this manuscript. CFH and LJW are co-corresponding authors. All authors reviewed the results and approved the final version of the manuscript.
Ethical Approval: The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Internal Review Board of Chang Gung Memorial Hospital.
Consent to Participate: Written informed consent was obtained from all participants.
Consent for Publication: Not applicable.
Data Availability: The data of the current study are available from the corresponding author on reasonable request.
Funding Statement: This study was funded by Chang Gung Memorial Hospital, Taiwan (CMRPG8C1051, CMRPG8C1291 and CMRPG8E1351). The funding sources had no involvement in the study design, collection, analysis and interpretation of data, writing of the report or the decision to submit the article for publication.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Liao, Y., McGee, D. L., Cao, G., Cooper, R. S. (2000). Quality of the last year of life of older adults: 1986 vs 1993. The Journal of the American Medical Association, 283(4), 512–518. DOI 10.1001/jama.283.4.512. [Google Scholar] [CrossRef]
2. Population Projections for Republic of China (Taiwan2020–2070. https://www.ndc.gov.tw/en/cp.aspx?n=2e5dcb04c64512cc. [Google Scholar]
3. Lin, Y. Y., Huang, C. S. (2016). Aging in Taiwan: Building a society for active aging and aging in place. Gerontologist, 56(2), 176–183. DOI 10.1093/geront/gnv107. [Google Scholar] [CrossRef]
4. Harada, C. N., Natelson Love, M. C., Triebel, K. L. (2013). Normal cognitive aging. Clinics in Geriatric Medicine, 29(4), 737–752. DOI 10.1016/j.cger.2013.07.002. [Google Scholar] [CrossRef]
5. Salthouse, T. A. (2019). Trajectories of normal cognitive aging. Psychology and Aging, 34(1), 17–24. DOI 10.1037/pag0000288. [Google Scholar] [CrossRef]
6. Herrmann, F. R., Montandon, M. L., Garibotto, V., Rodriguez, C., Haller, S. et al. (2021). Determinants of cognitive trajectories in normal aging: A longitudinal PET-MRI study in a community-based cohort. Current Alzheimer Research, 18(6), 482–491. DOI 10.2174/1567205018666210930111806. [Google Scholar] [CrossRef]
7. Constantinidou, F., Prokopiou, J., Nikou, M., Papacostas, S. (2015). Cognitive-linguistic performance and quality of life in healthy aging. Folia Phoniatrica et Logopaedica, 67(3), 145–155. DOI 10.1159/000440835. [Google Scholar] [CrossRef]
8. Li, R., Singh, M. (2014). Sex differences in cognitive impairment and Alzheimer’s disease. Frontiers in Neuroendocrinology, 35(3), 385–403. DOI 10.1016/j.yfrne.2014.01.002. [Google Scholar] [CrossRef]
9. Au, B., Dale-McGrath, S., Tierney, M. C. (2017). Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Research Reviews, 35(Suppl. 2), 176–199. DOI 10.1016/j.arr.2016.09.005. [Google Scholar] [CrossRef]
10. Levine, D. A., Gross, A. L., Briceno, E. M., Tilton, N., Giordani, B. J. et al. (2021). Sex differences in cognitive decline among US adults. JAMA Network Open, 4(2), e210169. DOI 10.1001/jamanetworkopen.2021.0169. [Google Scholar] [CrossRef]
11. Chen, C. Y., Wu, C. C., Huang, Y. C., Hung, C. F., Wang, L. J. (2018). Gender differences in the relationships among neurosteroid serum levels, cognitive function, and quality of life. Neuropsychiatric Disease and Treatment, 14, 2389–2399. DOI 10.2147/NDT.S176047. [Google Scholar] [CrossRef]
12. Patterson, T. L., Goldman, S., McKibbin, C. L., Hughs, T., Jeste, D. V. (2001). UCSD performance-based skills assessment: Development of a new measure of everyday functioning for severely mentally ill adults. Schizophrenia Bulletin, 27(2), 235–245. DOI 10.1093/oxfordjournals.schbul.a006870. [Google Scholar] [CrossRef]
13. World Health Organization (2012). WHOQOL-BREF: Introduction, administration, scoring and generic version of the assessment: Field trial version, December 1996. https://apps.who.int/iris/handle/10665/63529. [Google Scholar]
14. Griffiths, S., Hay, P., Mitchison, D., Mond, J. M., McLean, S. A. et al. (2016). Sex differences in the relationships between body dissatisfaction, quality of life and psychological distress. Australian and New Zealand Journal of Public Health, 40(6), 518–522. DOI 10.1111/1753-6405.12538. [Google Scholar] [CrossRef]
15. Kazandjian, C., Militello, L. K., Doumit, R. (2020). Sex differences on quality of life and mental health outcomes when using a brief cognitive-behavioral skill building intervention with adolescent syrian refugees: A secondary analysis. Community Mental Health Journal, 56(1), 157–164. DOI 10.1007/s10597-019-00453-1. [Google Scholar] [CrossRef]
16. Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J. et al. (1998). The mini-international neuropsychiatric interview (M.I.N.I.The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59(Suppl. 20), 22–33, quiz 34–57. [Google Scholar]
17. Kuo, C. J., Tang, H. S., Tsay, C. J., Lin, S. K., Hu, W. H. et al. (2003). Prevalence of psychiatric disorders among bereaved survivors of a disastrous earthquake in Taiwan. Psychiatric Services, 54(2), 249–251. DOI 10.1176/appi.ps.54.2.249. [Google Scholar] [CrossRef]
18. Mausbach, B. T., Harvey, P. D., Goldman, S. R., Jeste, D. V., Patterson, T. L. (2007). Development of a brief scale of everyday functioning in persons with serious mental illness. Schizophrenia Bulletin, 33(6), 1364–1372. DOI 10.1093/schbul/sbm014. [Google Scholar] [CrossRef]
19. McIntosh, B. J., Zhang, X. Y., Kosten, T., Tan, S. P., Xiu, M. H. et al. (2011). Performance-based assessment of functional skills in severe mental illness: Results of a large-scale study in China. Journal of Psychiatric Research, 45(8), 1089–1094. DOI 10.1016/j.jpsychires.2011.01.012. [Google Scholar] [CrossRef]
20. Huang, Y. C., Lee, Y., Lee, C. Y., Lin, P. Y., Hung, C. F. et al. (2020). Defining cognitive and functional profiles in schizophrenia and affective disorders. BMC Psychiatry, 20(1), 39. DOI 10.1186/s12888-020-2459-y. [Google Scholar] [CrossRef]
21. The WHOQOL Group (1998). Development of the world health organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551–558. DOI 10.1017/S0033291798006667. [Google Scholar] [CrossRef]
22. Vahedi, S. (2010). World health organization quality-of-life scale (WHOQOL-BREFAnalyses of their item response theory properties based on the graded responses model. Iranian Journal of Psychiatry, 5(4), 140–153. [Google Scholar]
23. Yao, G., Chung, C. W., Yu, C. F., Wang, J. D. (2002). Development and verification of validity and reliability of the WHOQOL-BREF Taiwan version. Journal of the Formosan Medical Association, 101(5), 342–351. [Google Scholar]
24. Noh, J. W., Kim, J., Park, J., Kim, H. J., Kwon, Y. D. (2015). Gender difference in relationship between health-related quality of life and work status. PLoS One, 10(12), e0143579. DOI 10.1371/journal.pone.0143579. [Google Scholar] [CrossRef]
25. Huang, S. W., Chi, W. C., Yen, C. F., Chang, K. H., Liao, H. F. et al. (2017). Does more education mean less disability in people with dementia? A large cross-sectional study in Taiwan. BMJ Open, 7(4), e013841. DOI 10.1136/bmjopen-2016-013841. [Google Scholar] [CrossRef]
26. Lovden, M., Fratiglioni, L., Glymour, M. M., Lindenberger, U., Tucker-Drob, E. M. (2020). Education and cognitive functioning across the life span. Psychological Science in the Public Interest, 21(1), 6–41. DOI 10.1177/1529100620920576. [Google Scholar] [CrossRef]
27. Halbreich, U., Lumley, L. A., Palter, S., Manning, C., Gengo, F. et al. (1995). Possible acceleration of age effects on cognition following menopause. Journal of Psychiatric Research, 29(3), 153–163. DOI 10.1016/0022-3956(95)00005-P. [Google Scholar] [CrossRef]
28. Maki, P. M., Dumas, J. (2009). Mechanisms of action of estrogen in the brain: Insights from human neuroimaging and psychopharmacologic studies. Seminars in Reproductive Medicine, 27(3), 250–259. DOI 10.1055/s-0029-1216278. [Google Scholar] [CrossRef]
29. Newhouse, P., Dumas, J. (2015). Estrogen-cholinergic interactions: Implications for cognitive aging. Hormones and Behavior, 74, 173–185. DOI 10.1016/j.yhbeh.2015.06.022. [Google Scholar] [CrossRef]
30. Lin, T. Y. (1983). Psychiatry and Chinese culture. Western Journal of Medicine, 139(6), 862–867. [Google Scholar]
31. Yu, D. S., Lee, D. T. (2012). Do medically unexplained somatic symptoms predict depression in older Chinese? International Journal of Geriatric Psychiatry, 27(2), 119–126. DOI 10.1002/gps.2692. [Google Scholar] [CrossRef]
32. Lara, E., Koyanagi, A., Caballero, F., Domenech-Abella, J., Miret, M. et al. (2017). Cognitive reserve is associated with quality of life: A population-based study. Experimental Gerontology, 87(Pt A), 67–73. DOI 10.1016/j.exger.2016.10.012. [Google Scholar] [CrossRef]
33. Ezzati, A., Zammit, A. R., Katz, M. J., Derby, C. A., Zimmerman, M. E. et al. (2019). Health-related quality of life, cognitive performance, and incident dementia in a community-based elderly cohort. Alzheimer Disease and Associated Disorders, 33(3), 240–245. DOI 10.1097/WAD.0000000000000324. [Google Scholar] [CrossRef]
34. Pettemeridou, E., Kennedy, M. R. T., Constantinidou, F. (2020). Executive functions, self-awareness and quality of life in chronic moderate-to-severe TBI. NeuroRehabilitation, 46(1), 109–118. DOI 10.3233/NRE-192963. [Google Scholar] [CrossRef]
35. Logsdon, R. G., Gibbons, L. E., McCurry, S. M., Teri, L. (2002). Assessing quality of life in older adults with cognitive impairment. Psychosomatic Medicine, 64(3), 510–519. DOI 10.1097/00006842-200205000-00016. [Google Scholar] [CrossRef]
36. Chae, W., Park, E. C., Jang, S. I. (2020). The association between the changes in general, family, and financial aspects of quality of life and their effects on cognitive function in an elderly population: The Korean longitudinal study of aging, 2008–2016. International Journal of Environmental Research and Public Health, 17(3), 1106. DOI 10.3390/ijerph17031106. [Google Scholar] [CrossRef]
37. Beckett, M., Goldman, N., Weinstein, M., Lin, I. F., Chuang, Y. L. (2002). Social environment, life challenge, and health among the elderly in Taiwan. Social Science & Medicine, 55(2), 191–209. DOI 10.1016/S0277-9536(01)00161-7. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2022 The Author(s). Published by Tech Science Press.
Copyright © 2022 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools