| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.021809
ARTICLE
Neurodevelopmental in Relation to Breastfeeding–Experiences among Hungarian Preterm Infants at 12 Months of Corrected Age: Empirical Study
1Department of Pediatrics, Faculty of Medicine, Pediatric Psychology and Psychosomatic Unit, Kálmán Laki Doctoral School, University of Debrecen, Debrecen, 4032, Hungary
2Department of Pediatrics, Faculty of Medicine, Pediatric Psychology and Psychosomatic Unit, University of Debrecen, Debrecen, 4032, Hungary
*Corresponding Author: Anna Szabina Szele. Email: szele.anna@ped.unideb.hu
Received: 07 February 2022; Accepted: 10 May 2022
Abstract: Preterm and low birth weight infants are at higher risk of neurodevelopmental outcomes; breastfeeding offers several beneficial aspects for them. This study aimed to describe the average neurodevelopmental outcomes of preterm infants and examine the associations between neurodevelopment and breastfeeding among Hungarian preterm infants at 12 months of corrected age. 154 preterm infants with low birth weight (<2500 g) and their mothers were participated in this study. Bayley-III Screening Test (Bayley Scales of Infant and Toddler Development Screening Test, Third Edition) was administered to measure the cognitive, language and motor skills of infants; breastfeeding data was obtained through parental anamnesis. To analyze data, independent sample t-test or the Welch t-test, Mann-Whitney tests, Chi-square tests of independence and Spearman’s rank correlation test were used to. Concerning the risk of developmental delay, Receptive and Expressive language and Fine motor subscales were the lowest. Examination of the associations between breastfeeding and neurodevelopmental performance identified significantly higher cognitive (U = 2047.5; P = 0.023) and fine motor (U = 2096.0; P = 0.037) skills in infants who were breastfed. We found significant positive correlations between the duration of breastfeeding and cognitive, expressive language and fine motor skills. The study draws the attention to the importance of breastfeeding and early screening. Further research is required to examine the casual relationship between neurodevelopmental outcomes and breastfeeding.
Keywords: Preterm infants; low birth weight; breastfeeding; duration of breastfeeding; neurodevelopmental outcomes
According to the WHO (World Health Organization) definition, preterm birth means to be born before 37 completed weeks of gestation. Preterm birth is commonly associated with an overlapping perinatal risk, low birth weight. Each year approximately 15 million children are born preterm worldwide [1]. In Hungary, this proportion is 8% of the population (approximately 8.000 new-borns) [2]. Nutritional needs of preterm babies significantly differ from their full-term counterparts, as they need more of any nutrient on a per kilogram basis. This phenomenon is mainly due to the physical development of preterm infants, i.e., the development of newly formed tissues is faster than in full-term counterparts. As well as, intercurrent diseases that often associated with preterm birth can also affect nutritional needs [3].
Breast-milk is the primary and most valuable source of nutrition and the main natural immune booster of both healthy new-borns and preterm infants, making them resistant to acute diseases and reducing the risk of developing pathological conditions [3–5]. According to the policy statement of the American Academy of Pediatrics (AAP), receiving of human milk is recommended for all preterm babies [4] and it is significant that early years care providers encourage the mothers to breastfeeding [6].
Breastfeeding has beneficial effects on immunological, gastrointestinal, nutritional, and psychological aspects [7]. Regarding its components, the milk of mothers of preterm infants is different from mothers of full-term babies. It contains more protein, energy, fat and immunizing agents, less lactose and more mineral salts compared to milk of mothers of full-term infants [3,8]. Breast-milk protects the preterm baby from gastrointestinal and respiratory infections, reduces the risk of developing NEC (necrotizing enterocolitis), ottis media, bacterial meningitis, bacteremia and acute inflammatory bowel disease. In breast-milk fatty acids found to be easily digested for new-borns, protective enzymes and hormones are essential for the growth and maturation of the digestive system, while lipids and fatty acids are indispensable for the balanced development of nervous system [3,7,9]. As a result, breastfed preterm infants experience fewer infections, spend fewer days in NICUs (neonatal intensive care units), show lower readmission rate in the first 12 months compared to formula-fed counterparts [9].
Besides the physiological advantages of breast milk, it also has significant and extensive effects on cognitive performance, behaviour, and mental health [10]. According to the literature, in later life breastfed children have better results in tests of intellectual ability compared to the formula-fed children [9], and the greater breast milk intake also is associated with higher IQ scores, better working memory and arithmetic skills [11]. However, the mechanism of breast milk to neural growth is uncertain. According to the study of Isaacs et al. [12] impact of breastfeeding on IQ may be explained, by promoting the development of white matter. However, biochemical components of breast milk, like acids (long-chain polyunsaturated fatty acids, docosahexaenoic acid), hormones (e.g., thyroxin, oxytocin), growth factors, micronutrients (e.g., iron, folate, zinc) can play a role in brain development, cognitive benefit and infant attachment [12–15]. Research into the link between breastfeeding and attachment is abounding. Longitudinal study of Tharner et al. [16] found that the increased duration of breastfeeding was associated with greater attachment security and maternal sensitive responsiveness at the age of 14 months of infants. However, the incidence and duration of breastfeeding are usually lower among preterm infants compared to full-term babies. The lower incidence may be associated with breastfeeding challenges (e.g., maintaining milk supply), preterm delivery and immaturity of the new-born [17,18]. According to the AAP, the United Nations Children’s Fund (UNICEF) and the WHO, exclusive breastfeeding or giving breast milk is recommended for 6 months [4,9,19].
Despite of the benefits and protective factors of breastfeeding, preterm infants can be regarded as a vulnerable population, not only in terms of neurodevelopmental outcomes (apnoea, retinopathy of prematurity (ROP), bronchopulmonary dysplasia (BPD), pulmonary hypertension (PH)) but also in terms of intellectual development [20–22]. Therefore, in order to prevent future difficulties and developmental deficits, cognitive, motor and language screening of children at risk is especially significant as early as possible.
The objectives of this study are the description of neurodevelopmental outcomes on Bayley-III Screening Test subscales (cognitive, receptive and expressive language, fine and gross motor skills) and the examination of the association between neurodevelopmental outcomes, breastfeeding and the duration of breastfeeding adjusted for preterm and low birth weight children at 12 months of corrected age in a Hungarian sample.
2.1 Research Design and Sample
It is a historical cohort study, in which a cohort of 154 low birth weight (<2500 g) and preterm infants (<37 weeks) at 12 months of corrected age were assessed at the Pediatric Psychology and Psychosomatic Unit of the Department of Pediatrics of the University of Debrecen between December 2017 and January 2019. All of them were delivered at the Department of Obstetrics and Gynecology of the University of Debrecen. Only those infants were included in our study who underwent developmental assessment using the five distinct subscales of the Bayley-III Screening Test. Fig. 1 illustrates the dropout rate of the sample. Based on the Screening Test Manual, correction for prematurity was made. After the calculating of chronological age, adjusted age is needed in case of prematurity through 24 months of chronological age [23]. In compliance with the Ethical Principles of the World Medical Association Declaration of Helsinki, the study was approved by the Medical Research Council of Hungary (12053-2/2018/EKU). Written informed consent was obtained from the parents of subjects’.
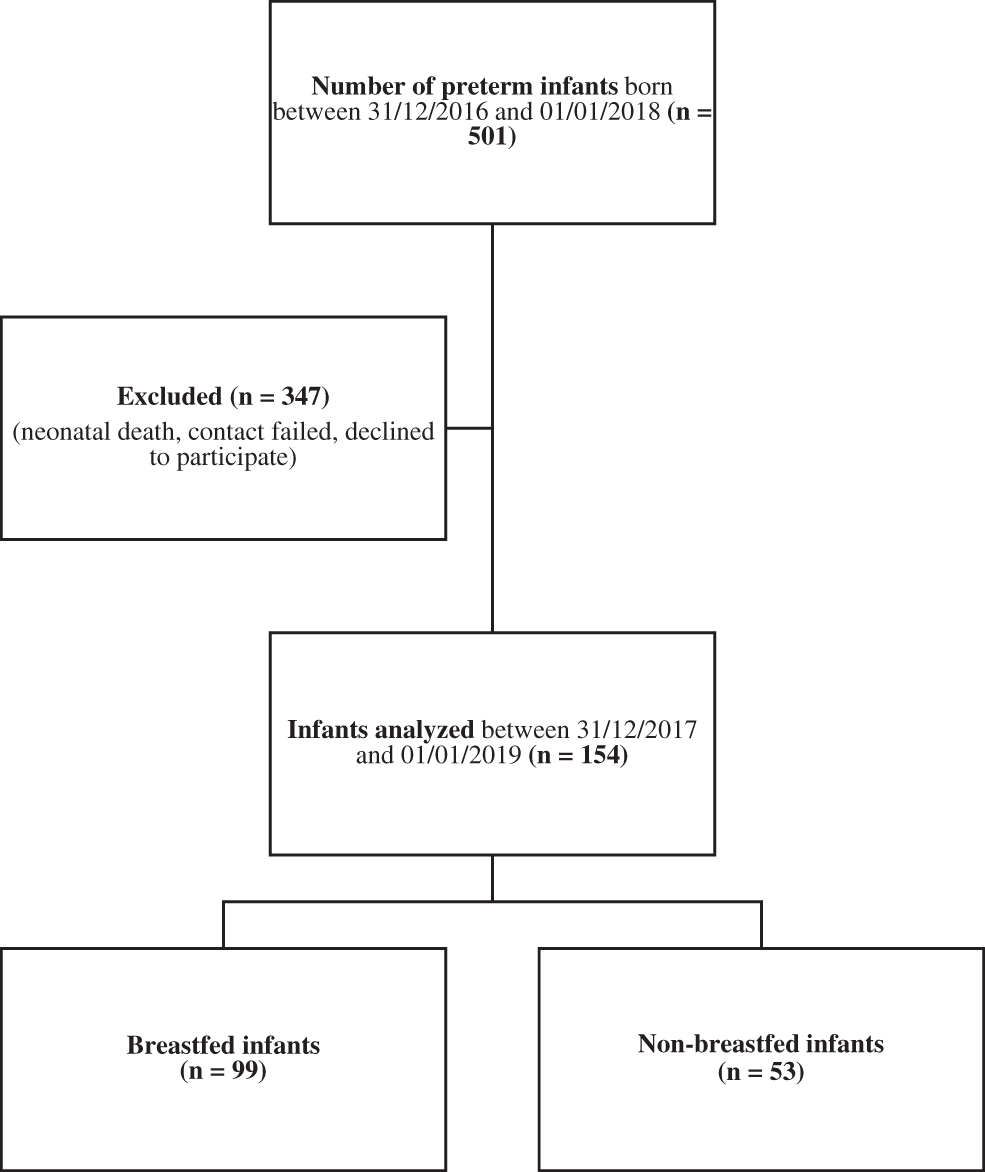
Figure 1: Flow chart of the sample selection
2.2.1 Bayley-III Screening Test (Bayley Scales of Infant and Toddler Development Screening Test, Third Edition) [23]
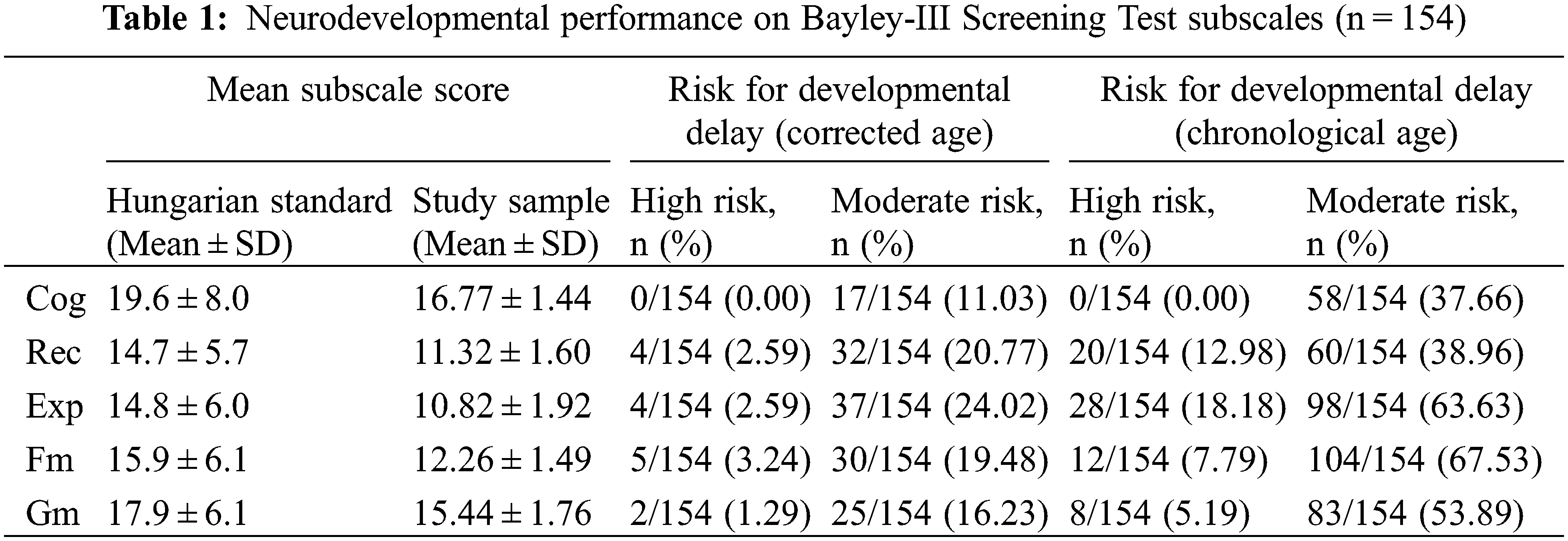
In the identification of developmental difficulties and delays, BSID-III (Bayley Scales of Infant and Toddler Development–Third Edition) is currently the most advanced developmental tool for early prevention [24]. Both the full BSID-III and its screening test version were adapted and standardized in 2017 in Hungary. To assess the early developmental performance, we used the Screening Test, which allows the quick investigation of cognitive, language and motor skills of infants and toddlers between 1 to 42 months. Within the Language Scale, the test distinguishes Receptive and Expressive language subscales, while within the Motor Scale differentiates Fine and Gross motor subscales. Its primary purpose is to determine that the development of child is appropriate or further diagnostically testing is needed. By administering the Screening Test, degree of risk for developmental delay can be determined: high, moderate and low risk can be distinguished. During the Hungarian standardization process of the Screening Test, 85 preterm and low birth weight children were examined (2 to 42 months of corrected age), and we have also mean scores and standard deviations from an adjusted control group [23] (see Table 1).
2.2.2 Developmental Characteristics and the Duration of Breastfeeding
Developmental characteristics of the child (neonatal and perinatal variables, e.g., gestational age, birth weight) were gathered retrospectively from the clinical database of the Department of Pediatrics of the University of Debrecen, from the neonatal final reports. Information about early feeding, the duration of breastfeeding, and the socio-demographic characteristics was obtained based on a maternal anamnesis.
IBM SPSS Statistics v25 was used for statistical analysis. The normality of the sample was calculated by one-sample Kolmogorov-Smirnov test. Most of our data did not follow a normal distribution, so non-parametric tests were used. Mann-Whitney tests were used for group comparisons, and Spearman’s rank correlation test was used to measure the correlation between neurodevelopmental outcomes and duration of breastfeeding. Independent sample t-test or the Welch t-test and the Mann-Whitney test were applied to compare the means and distribution of gestational age, birth weight and maternal age, and Chi-square tests of independence were used to examine the relationship of breastfeeding and childbirth, maternal education, marital status and subjective socioeconomic status in the breastfed and non-breastfed groups. P-values below 0.05 were considered statistically significant.
3.1 General Data (Means and Standard Deviations)
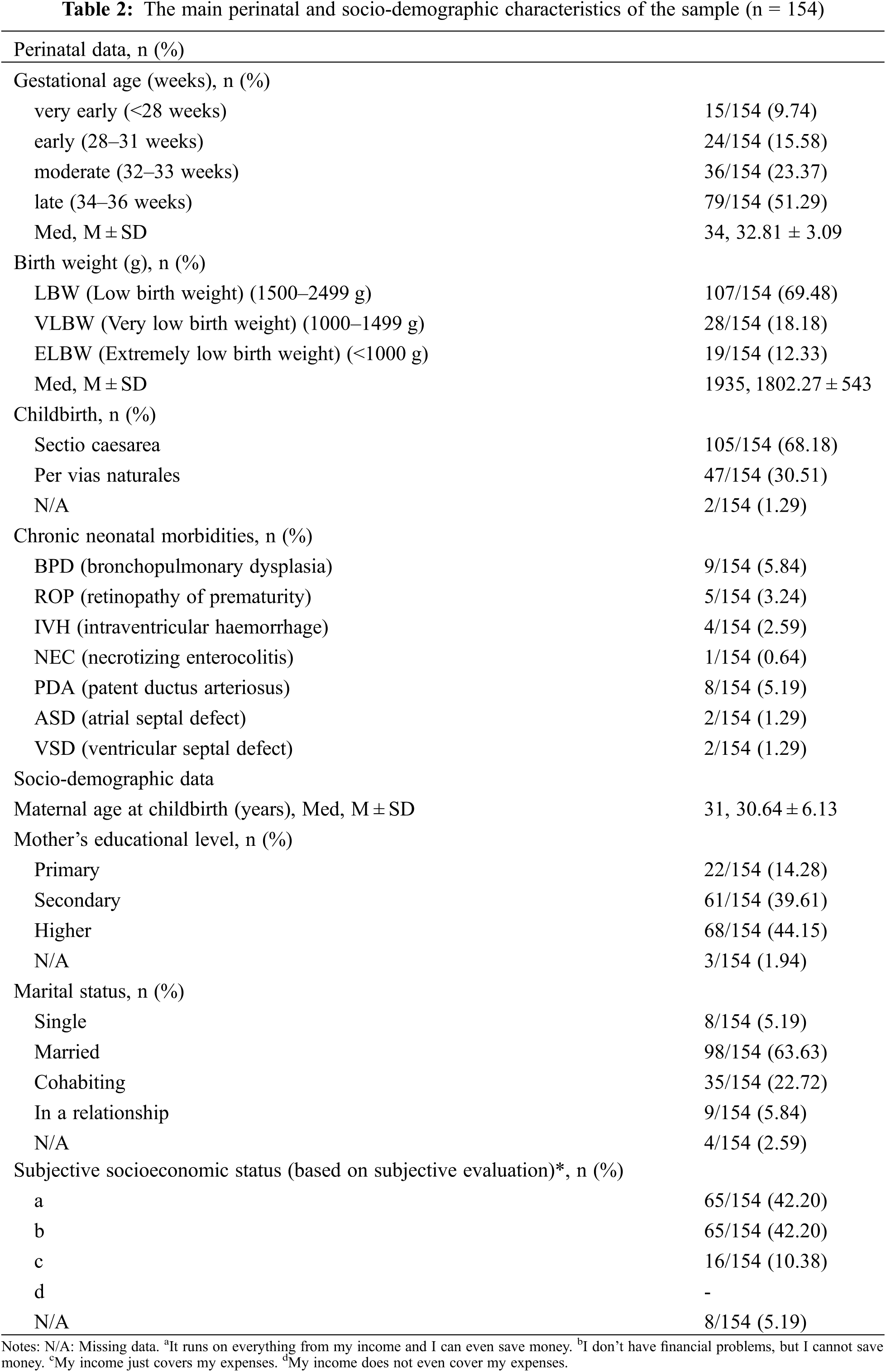
All infants involved in the study (n = 154) were Hungarian with valid health insurance, the gender ratio was nearly balanced (73 females, 81 males). The mean birth weight of the children was between 540 and 2490 g (M = 1802.27, SD = 543), and the mean gestational age of the children was between 24 and 36 weeks (M = 32.81, SD = 3.09). The main perinatal and socio-demographic characteristics of the sample are summarized in Table 2.
3.2 Neurodevelopment on Bayley-III Screening Test Subscales
In our sample, the proportion of ‘high risk for developmental delay’ was negligible, ranging from 0% (Cognitive subscale) to 3.24% (Fine motor subscale). The proportion of ‘moderate risk for developmental delay’ was higher, ranging from 11.03% (Cognitive subscale) to 24.02% (Expressive language subscale). Compared to the Hungarian standard full-term counterparts’ values, our sample showed lower points for all subscales (see Table 1). Correction for prematurity only has a role in determining the risk for developmental delays, as the Screening Test works with the same Total Raw Scores both at corrected and chronological ages. For illustrative purposes only, Table 1 shows the risk for developmental delay of infants at chronological age. In case of unadjusted results, considerably higher risk for developmental delay is identified, especially in the Language and Fine motor subscales.
3.3 Comparison of Breastfed and Non-Breastfed Groups
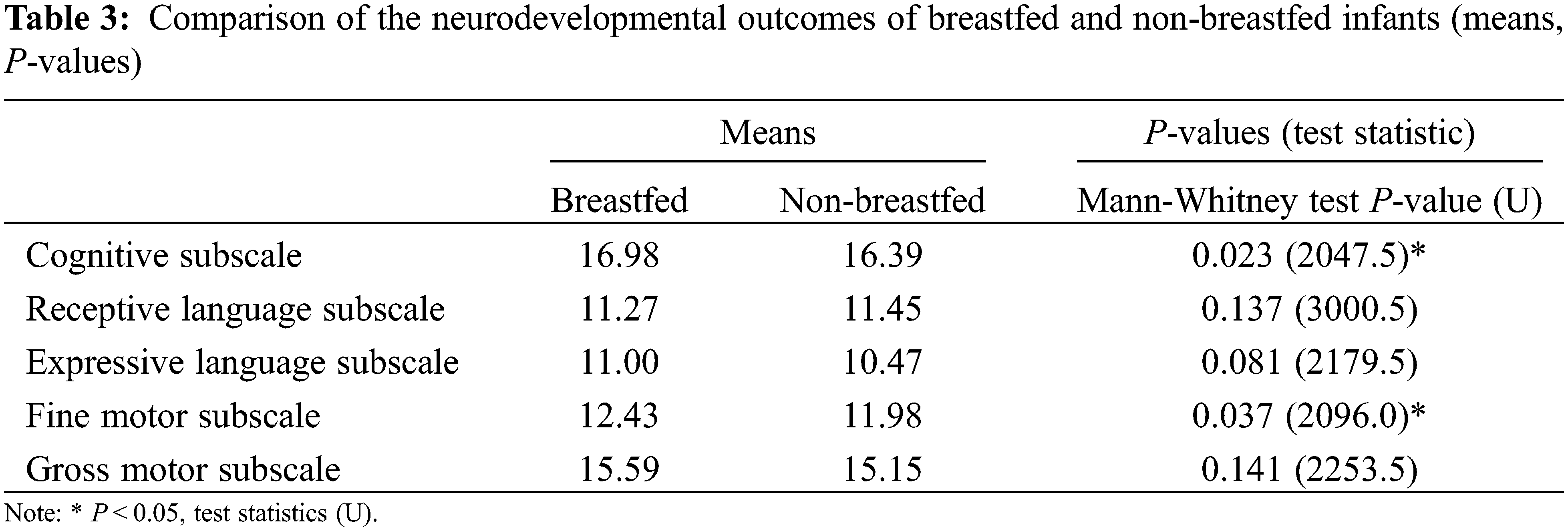
In our sample, 99 (64.28%) mothers were able to breastfeed their new-borns, while 53 (34.41%) mothers failed to start breastfeeding (they feed their babies with donor milk or preterm formula). In 2 cases we had no information about breastfeeding. Examining the relationship between breastfeeding and neurodevelopment, we found a higher average performance on the Cognitive, Expressive language and Motor subcales. For the Cognitive (U = 2047.5; P = 0.023) and Fine motor subscales (U = 2096.0; P = 0.037), the differences were found to be significant between breastfed and non-breastfed children (see Table 3). We also examined the association of duration of breastfeeding period and developmental performance. In our sample, breastfeeding period ranged from 2 weeks to 14 months. Using the Spearman’s rank correlation test, we identified significant positive correlations between the duration of breastfeeding and the Cognitive (r = 0.218; P = 0.07), Expressive language (r = 0.209; P = 0.01), and Fine motor (r = 0.181, P = 0.026) skills. However, the value of the coefficient of determination (r2) is low for all three subscale variables (rcog2: 0.04; rexp2: 0.04; rfin2: 0.03).
Examining the perinatal and socio-demographic characteristics of breastfed and non-breastfed groups, along similar aspects that the Table 2 does, no major differences were found to be between the two groups by either descriptive statistics or statistical tests, except for a few variables (gestational age and birth weight). Both independent sample t-test or the Welch t-test (depending on the equality of variances) as well as the Mann-Whitney test were applied to compare the means and distribution of gestational age, birth weight and maternal age in the breastfed and non-breastfed groups. The two groups showed significant differences in mean value for gestational age (M ± SDbreastfed = 33.70 ± 2.37 weeks; M ± SDnon-breastfed = 31.00 ± 3.63 weeks) and birth weight (M ± SDbreastfed = 1967.88 ± 451.01 g; M ± SDnon-breastfed = 1487.92 ± 581.44 g) (P-value < 0.001), but no difference for the mean maternal age (M ± SDbreastfed = 30.52 ± 6.48 years; M ± SDnon-breastfed = 30.89 ± 5.45 years; P = 0.723). The Mann-Whitney results do coincide with it, giving P-values < 0.001 for gestational age, birth weight, and P-value = 0.761 for maternal age. At the level of distribution of childbirth, maternal education, marital status, and subjective socioeconomic status, the two groups were similar. Chi-square test of independence were applied to see the relationship of breastfeeding and the childbirth (P = 0.089; χ² = 2.885), maternal education (P = 0.394; χ² = 1.861), marital status (P = 0.175; χ² = 4.962), and subjective socioeconomic status (P = 0.913; χ² = 0.181). Based on 5% significance level we can conclude that in none of the cases we found significant relationships, hence, the subsamples of the two groups showed no significant (conditional) distribution regarding the childbirth, maternal education, marital status and subjective socioeconomic status.
4.1 Neurodevelopmental Outcomes on Bayley-III Screening Test
The Bayley-III Screening Test, in addition to providing a comprehensive picture of cognitive, language and motor developmental characteristics in early childhood, is able to screen for children at risk for delayed development, thus differentiating children at high, moderate, or low risk for developmental delays. However, based on its results, no child can be considered to be delayed in neurodevelopment [23]. Regarding the neurodevelopmental results of our sample, the lowest performance was identified on the Receptive, Expressive language and Fine motor subscales. This result is consistent with the most literature findings. It is well known, preterm infants have significantly lower neurodevelopmental skills in early ages compared to their full-term counterparts. Difficulties in the motor skills may negatively affect the communication skills, such as joint attention and face-to-face interaction (complicating the process of language acquisition) [25,26].
4.2 The Connection between Neurodevelopment, Breastfeeding and the Duration of Breastfeeding
According to the results of Mann-Whitney tests, breastfed children had better cognitive and fine motor skills at 12 months of corrected age. The more the duration of breastfeeding was the better performance measured on Cognitive, Expressive and Fine motor subscales. We compared the means and distribution of gestational age, birth weight and maternal age in the breastfed and non-breastfed groups, and examined the relationship of breastfeeding and childbirth, maternal education, marital status and subjective socioeconomic status also. We identified significant difference only in gestational age and birth weight; nevertheless, we do not claim that there is a casual relationship between our variables.
Our results are consistent with literature findings that emphasize both the short- and long-term positive effects of breastfeeding on the child’s psychological and intellectual development. Nagy et al. [27] identified breastfeeding as predictor variable of adaptive behaviour characteristic of low birth weight and preterm children at the age of 2. Jardí et al. [28] found that exclusive breastfeeding for at least 4 months results in a higher neurodevelopmental index at 6 and 12 months of age. The meta-analytical study of Horta et al. [29] focused on the investigation of long-term effects, their results emphasized that children who were breastfed in infancy, significantly performed better on intelligence tests (mean difference 3.44 points) in childhood and adolescence compared to non-breastfed counterparts. Breastfed preterm infants with ELBW are characterized by higher mental, motor and behavioural performance at 18 and 30 months of age [4].
Among preterm infants, examining the effects of exclusive breastfeeding and formula feeding, differences can be identified also. According to the study of Li et al. [30], among children with a gestational age of 28 and 30 weeks, breastfeeding played an important role in weight gain, reduced feeding intolerance, the incidence of NEC, and length of hospital stay. No correlations were found among formula milk feeding group. Lucas et al. [31] found that breastfed preterm infants perform better on intelligence tests later in life compared their formula-fed counterparts. Overall, we can conclude that breastfeeding for preterm infants is beneficial not only from a nutritional, gastrointestinal, immunological point of view, but developmental and psychological also. In the first year of life, the brain undergoes rapid development, which is intensely influenced by nutritional aspects. The beneficial effects of breastfeeding on the early brain development can be explicable by the nutrients in breast milk, which are missing from the formula [11]. The study of Isaacs et al. [12] found breast milk contribute to the white matter growth. In addition, important factor can be that maternal care becomes longer and more intensive with breastfeeding. The environmental factors can have a great impact on the brain development, especially mother-baby interactions. According to the study of Smith et al. [14], those mothers, who exclusively breastfeed their infants, provide the greatest amount of emotional care, while exclusively formula group the least. The lactation hormones also can increase the proximity seeking behaviour of mothers thereby affect mother-child relationship [32]. In summary, the breastfeeding can be beneficial to the brain development not just through nutritional aspects, but also due to the mother-baby interactions [11].
In our results, the low coefficients of determination (r2) indicate that other factors and variables may contribute to the neurodevelopmental performance. A potential confounding factor can be, for example, the birth weight, duration of pregnancy, sex, length of hospital stay, family socioeconomic condition just to mention a few. Thus, we cannot conclude that the increase in neurodevelopment is due to breastfeeding unequivocally. With breastfeeding, mothers provide a cognitively more stimulating environment for their babies, so not only the components of breast-milk but the family environment and the mother-child interaction also contribute to the development of the child.
One of the potential limitations of our study is the absence of adjusted control group. Description of the neurodevelopmental outcomes we used the Hungarian standard values as a reference, but the comparison with it should be treated with caution, as children were included in standardization process from 2 to 42 months of age. Another limitation of our research is that potential confounding factors that may affect neurodevelopmental performance were not statistically controlled. With our statistical analysis, we cannot conclude that breastfeeding had the main effect on the neurodevelopment of participants; we can only identify a positive association between variables, not causal relationship. However, this study is part of a piece of a larger follow-up PhD study, e.g., [27], in which we take into consideration other variables when evaluate the development.
Due to the consequences of prematurity, preterm babies regarded as a vulnerable population [33], who begins the early life with a neurodevelopmental disadvantage. Breastfeeding can help them redressing this disadvantage. For public health, it is essential to draw the attention to the importance of breastfeeding, to inform mothers about its extensive positive effects on the child and mother, and to involve preterm babies in psychological screening as soon as possible. In summary breastfed infants have shown significantly better cognitive and fine motor skills in the Bayley-III Screening Test at 12 months of corrected age. However, these findings should be treated with caution, because of the potential confounding factors. The importance of the reported study is increased by that it is one of the first pieces of research with Bayley-III Screening Test in Hungary.
Disclosure Statement of Preprints: Our work has been posted as a preprint on Research Square Platform through the In Review preprint service offered by Springer Nature. Research Square, https://www.researchsquare.com/article/rs-140432/v1; DOI: 10.21203/rs.3.rs-140432/v1.
Acknowledgement:The authors would like to thank all the children and parents for their participation. We are grateful to Prof. György Balla and Prof. Tamás Szabó, Directors of the Department of Pediatrics for supporting our research, and our colleagues at the Pediatric Psychology and Psychosomatic Unit of the Department of Pediatrics of the University of Debrecen.
Authorship: Study conception and design: BEN, ASZSZ; data collection: ASZSZ; analysis and interpretation of results: BEN, ASZSZ; draft manuscript preparation: ASZSZ; manuscript revision: BEN, ASZSZ. All authors reviewed the results and approved the final version of the manuscript.
Funding Statement: Open access funding provided by University of Debrecen.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. WHO (2018). Preterm birth. Key facts. https://www.who.int/news-room/fact-sheets/detail/preterm-birth/. [Google Scholar]
2. UNICEF Office of Research (2013). Child well-being in rich countries. A comparative overview. Innocenti Report Card 11, UNICEF Office of Research, Florence. https://www.unicef-irc.org/publications/pdf/rc11_eng.pdf. [Google Scholar]
3. Underwood, M. A. (2013). Human milk for the premature infant. Pediatric Clinics of North America, 60(1), 189–207. DOI 10.1016/j.pcl.2012.09.008. [Google Scholar] [CrossRef]
4. American Academy of Paediatrics (2012). Breastfeeding and use of human milk. Pediatrics, 129, 827–841. DOI 10.1542/peds.2011-3552. [Google Scholar] [CrossRef]
5. Brenner, M. G., Buescher, E. S. (2011). Breastfeeding: A clinical imperative. Journal of Women’s Health, 20(12), 1767–1773. DOI 10.1089/jwh.2010.2616. [Google Scholar] [CrossRef]
6. Dombrowski, L., Henderson, S., Leslie, J., Mohammed, K., Johnson, D. et al. (2020). The role of early years care providers in supporting continued breastfeeding and breast milk feeding. Early Years, 40(2), 205–220. DOI 10.1080/09575146.2018.1430123. [Google Scholar] [CrossRef]
7. EFCNI (2020). Breast milk for preterm babies. More than a mental. https://www.efcni.org/wp-content/uploads/2021/08/2021_08_25_EFCNI_Stillbroschure_englisch_Web.pdf. [Google Scholar]
8. Sahin, S., Ozdemir, T., Katipoglu, N., Akcan, A. B., Turkmen, M. K. (2020). Comparison of changes in breast milk macronutrient content during the first month in preterm and term infants. Breastfeeding Medicine, 15(1), 56–62. DOI 10.1089/bfm.2019.0141. [Google Scholar] [CrossRef]
9. Buchanan, A. O., Marquez, M. L. (2015). Pediatric nutrition and nutritional disorders. In: Marcdante, K., Kliegman, R. (Eds.Nelson essentials of pediatrics, pp. 86–106. Philadelphia, PA: Elsevier Saunders. [Google Scholar]
10. Krol, K. M., Grossmann, T. (2018). Psychological effects of breastfeeding on children and mothers. psychologische effekte des stillens auf kinder und mütter. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz, 61(8), 977–985. DOI 10.1007/s00103-018-2769-0. [Google Scholar] [CrossRef]
11. Brown, B. M. (2017). The science of breastfeeding and brain development. Breastfeeding Medicine, 12(8), 459–461. DOI 10.1089/bfm.2017.0122. [Google Scholar] [CrossRef]
12. Isaacs, E. B., Fischl, B. R., Quinn, B. T., Chong, W. K., Gadian, D. G. et al. (2010). Impact of breast milk on intelligence quotient, brain size, and white matter development. Pediatric Research, 67(4), 357–362. DOI 10.1203/PDR.0b013e3181d026da. [Google Scholar] [CrossRef]
13. Chiurazzi, M., Cozzolino, M., Reinelt, T., Nguyen, T. D., Elke Chie, S. et al. (2021). Human milk and brain development in infants. Reproductive Medicine, 2, 107–117. DOI 10.3390/reprodmed2020011. [Google Scholar] [CrossRef]
14. Smith, J. P., Ellwood, M. (2011). Feeding patterns and emotional care in breastfed infants. Social Indicators Research, 101(2), 227–231. DOI 10.1007/s11205-010-9657-9. [Google Scholar] [CrossRef]
15. Oddy, W. H. (2006). Fatty acid nutrition, immune and mental health development from infancy through childhood. In: Huang, J. D. (Ed.Frontiers in nutrition research, pp. 177–211. New York: Nova Science Publishers. [Google Scholar]
16. Tharner, A., Luijk, M. P. C. M., Raat, H., Ijzendoorn, M. H., Bakermans-Kranenburg, M. J. et al. (2012). Breastfeeding and its relation to maternal sensitivity and infant attachment. Journal of Developmental and Behavioral Pediatrics, 33(5), 396–404. DOI 10.1097/DBP.0b013e318257fac3. [Google Scholar] [CrossRef]
17. Callen, J., Pinelli, J. (2005). A review of the literature examining the benefits and challenges, incidence and duration, and barriers to breastfeeding in preterm infants. Advances in Neonatal Care, 5(2), 72–88. DOI 10.1016/j.adnc.2004.12.003. [Google Scholar] [CrossRef]
18. Perrella, S. L., Williams, J., Nathan, E. A., Fenwick, J., Hartmann, P. E. et al. (2012). Influences on breastfeeding outcomes for healthy term and preterm/sick infants. Breastfeeding Medicine, 7(4), 255–261. DOI 10.1089/bfm.2011.0118. [Google Scholar] [CrossRef]
19. Behzadifar, M., Saki, M., Behzadifar, M., Mardani, M., Yari, F. et al. (2019). Prevalence of exclusive breastfeeding practice in the first six months of life and its determinants in Iran: A systematic review and meta-analysis. BMC Pediatrics, 19(384), 1–10. DOI 10.1186/s12887-019-1776-0. [Google Scholar] [CrossRef]
20. Choi, E. K., Shin, S. H., Kim, E. K., Kim, H. S. (2019). Developmental outcomes of preterm infants with bronchopulmonary dysplasia-associated pulmonary hypertension at 18–24 months of corrected age. BMC Pediatrics, 19(26), 1–8. DOI 10.1186/s12887-019-1400-3. [Google Scholar] [CrossRef]
21. Potijk, M. R., de Winter, A. F., Bos, A. F., Kerstjens, J. M., Reijneveld, S. A. (2012). Higher rates of behavioural and emotional problems at preschool age in children born moderately preterm. Archives of Disease in Childhood, 97, 112–117. DOI 10.1136/adc.2011.300131. [Google Scholar] [CrossRef]
22. Woythaler, M. A., McCormick, M. C., Smith, V. C. (2011). Late preterm infants have worse 24-month neurodevelopmental outcomes than term infants. Pediatrics, 127(3), 622–629. DOI 10.1542/peds.2009-3598. [Google Scholar] [CrossRef]
23. Bayley, N. (2005). Bayley scales of infant and toddler development. In: Screening test manual, 3rd ed San Antonio, TX: NCS Pearson Inc. [Google Scholar]
24. Bayley, N. (2006). Bayley scales of infant and toddler development. In: Administration manual, 3rd ed, San Antonio, TX: Harcourt Assessment. [Google Scholar]
25. Benassi, E., Savini, S., Iverson, J. M., Guarini, A., Caselli, M. C. et al. (2016). Early communicative behaviors and their relationship to motor skills in extremely preterm infants. Research in Developmental Disabilities, 48, 132–144. DOI 10.1016/j.ridd.2015.10.017. [Google Scholar] [CrossRef]
26. Sansavini, A., Pentimonti, J., Justice, L., Guarini, A., Savini, S. et al. (2014). Language, motor and cognitive development of extremely preterm children: Modeling individual growth trajectories over the first three years of life. Journal of Communication Disorders, 49, 55–68. DOI 10.1016/j.jcomdis.2014.02.005. [Google Scholar] [CrossRef]
27. Nagy, B. E., Gáll, J. M., Szele, A. S. (2021). Predictor variables of neurodevelopmental characteristics at 2 years among low birth weight and preterm children: A 2-year follow-up study. Early Child Development and Care, 1–16. DOI 10.1080/03004430.2021.2012173. [Google Scholar] [CrossRef]
28. Jardí, C., Hernández-Martínez, C., Canals, J., Arija, V., Bedmar, C. et al. (2018). Influence of breastfeeding and iron status on mental and psychomotor development during the first year of life. Infant Behavior and Development, 50, 300–310. DOI 10.1016/j.infbeh.2017.05.009. [Google Scholar] [CrossRef]
29. Horta, B. L., de Mola, C. L., Victoria, C. G. (2015). Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatrica, 104, 14–19. DOI 10.1111/apa.13139. [Google Scholar] [CrossRef]
30. Li, Y. W., Yang, C. Y., Yang, L., Han, Z. L. (2017). Effect of breastfeeding versus formula milk feeding on preterm infants in the neonatal intensive care unit. Chinese Journal of Contemporary Pediatrics, 19(5), 572–575. [Google Scholar]
31. Lucas, A., Morley, R., Cole, T. J., Lister, G., Leeson-Payne, C. (2009). Breast-milk and subsequent intelligence quotient in children born preterm. Lancet, 339(8788), 261–264. DOI 10.1016/0140-6736(92)91329-7. [Google Scholar] [CrossRef]
32. Uvnas-Moberg, K., Petersson, M. (2005). Oxytocin, a mediator of anti-stress, well-being, social inter-action, growth and healing. Zeitschrift fur Psychosomatische Medizin und Psychotherapie, 51(1), 57–80. DOI 10.13109/zptm.2005.51.1.57. [Google Scholar] [CrossRef]
33. Aarnoudse-Moens, C. S. H., Weisglas-Kuperus, N., van Goudoever, J. B., Oosterlaan, J. (2009). Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics, 124(2), 717–728. DOI 10.1542/peds.2008-2816. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |