Mental Health Promotion
| International Journal of Mental Health Promotion |
DOI: 10.32604/IJMHP.2021.016408
ARTICLE
Determinants of Positive Mental Health in Adolescents–A Cross-Sectional Study on Relationships between Positive Mental Health, Self-Esteem, Character Strengths and Social Inclusion
1The Finnish Medical Society, Helsinki, 00100, Finland
2Finnish Institute for Health and Welfare, Mental Health Unit, Helsinki, 00271, Finland
3Faculty of Social Sciences, Health Sciences Unit, Tampere University, Tampere, 33520, Finland
*Corresponding Author: Hanna Ahrnberg. Email: hanna.auramo@helsinki.fi
Received: 03 March 2021; Accepted: 01 May 2021
Abstract: Adolescence is a crucial time period with especial vulnerability for development of mental health problems. Growing interest is focusing on the determinants of positive mental health in order to find the key concepts that could be influenced in the promotion of mental well-being of adolescents. In this study we aim to explore the relations between self-esteem, character strengths and experience of social inclusion as determinants of adolescents’ positive mental health controlled for selected sociodemographic background factors. The study population (n = 195) consisted of comprehensive school students who filled in an electronic questionnaire of adolescent’s mental well-being in Fall 2019. The questionnaire included measures of Warwick-Edinburgh Mental Well-being Scale (WEMWBS), VIA Youth-measure 96, Rosenberg Self-Esteem Scale and Experience of Social Inclusion Scale. The methods included group comparisons and General Linear Model computed by SPSS 24.0. The strongest association was found between positive mental health and self-esteem (β = 0.789, p < 0.001), followed by character strengths of hope and kindness and experience of social inclusion. Interestingly, family’s socioeconomic factors did not associate significantly with positive mental health in the final statistical model. In terms of our results, it seems that self-esteem, character strengths and experience of social inclusion might have stronger association with adolescents’ mental well-being than family’s socioeconomic determinants. Therefore, it should be discussed whether psychological determinants overcome the individual effect of poor socioeconomic status as factors that influence positive mental health. Further studies are needed to establish these results more firmly.
Keywords: Positive mental health; mental well-being; character strengths; self-esteem; social inclusion; adolescence
Adolescence is a crucial time period marked with many changes. It is the time for developing social and emotional habits and interpersonal skills. In addition, adolescence is the time for planning for future educational and occupational paths and learning to live independent from parents. During this challenging time, adolescents are especially vulnerable to mental health problems, and thus social exclusion, educational problems and stigma [1]. Mental health problems of young people are declared as a global concern that should be addressed by researchers and policy makers [2] and to date, there is convincing evidence that promoting adolescent mental health is effective in reducing mental health problems among youth [3–6]. Furthermore, growing evidence underlines the importance of promoting adolescent’s mental health, not only by focusing on clinical pathologies, but also by addressing those factors that maintain and promote positive mental health [7].
Positive mental health, often referred to mental well-being, is something beyond just absence of mental illness. It is described as a state where individual has positive but realistic view of self-concept and his/her own abilities, capability to cope with normal stressors in life and being able to contribute to the surrounding community. It is considered to include two parts: the hedonic perspective referring to subjective experience of happiness and satisfaction in life and eudaimonic perspective referring to good psychological functioning [8]. Positive mental health is a multidimensional and context dependent phenomenon, including various concepts of well-being related to self and others, e.g., positive emotions, self-esteem, presence of strengths, resilience and successful socioemotional interaction [9]. Higher positive mental health has been associated with better learning outcomes, productivity and creativity, good relationships, prosocial behaviour, and general good health and life expectancy [10]. Additionally, among adolescents it has been shown protective for suicidal ideation and academic impairment [11].
Growing interest is focusing on the determinants of positive mental health in order to find the key concepts that could be influenced and enhanced in the promotion of mental well-being, and furthermore, positive development of adolescents in a larger scale [12]. In a population-based Finnish sample, positive mental health is reported to be higher among students in secondary school compared with students in primary schools [13]. In addition, results from previous studies suggest that also subjective well-being declines in early adolescence, especially for girls [14]. It seems, that the crucial time period for changes in positive mental health is during 12 to 15 years. This, and acknowledging the fact that positive mental health is reported to fluctuate during adolescence [12,15] has increased the need to study and to better understand the underlying mechanisms that could be influenced already in early adolescence.
To date, positive mental health has been shown to associate with both sociodemographic and psychological factors. Guo et al. [12] reported that e.g., better family’s financial situation, female gender, experienced social trust and higher level of satisfaction on self-appearance were associated with higher positive mental health. Similarly, better financial situation of the family, higher parental educational level and intact family background was associated with higher positive mental health, ‘flourishing’, in a population-based study of Finnish adolescents [13]. Beyond sociodemographic factors, higher self-esteem, character strengths and experience of social participation have all been reported to associate with both hedonic and eudaimonic perspectives of positive mental health, as better well-being and functioning in individual level but also as part of social environment by prosocial behavior [16–20].
Self-esteem, referring to person’s sense of self-worth, is a well-reported determinant of subjective well-being. High self-esteem is associated with better subjective well-being [21], higher life satisfaction, positive affect, meaning in life and subjective vitality [16] and it predicts success and well-being in life domains such as relationships, work, and health [22]. Self-esteem is considered as relatively stable but definitely not immutable trait. Within life trajectory it typically increases within age, already seen in the transition from adolescence to adulthood [22,23]. It can be strengthened through personal traits but also by healthy interpersonal relationships as well as collective social experiences within larger groups of people, e.g., in school and society [23].
Social inclusion is a well-recognized determinant of health and especially of mental well-being [24] and it fits well in the arising paradigm of well-being beyond just lack of illness [25]. Social inclusion constitutes from interpersonal relations, community participation as well as sense of being able to influence on one’s own life course and social environment. In the research on adolescence, especially participation has been the focus of interest. Participation in constructive, non-academic activities in school and community has been reported to enhance school engagement and academic achievements, but also other aspects of positive youth development. [26,27] Participation is thought to provide sense of accomplishments and enjoyment, and it has been shown to associate with better general health and well-being in cross-cultural study designs [20]. Previous research report that adolescents involving regularly in after school activities tend to report better health, have healthier lifestyles and less risk-taking behaviour [20] and better mental well-being also in later life [28]. Interestingly, social participation is even shown to have a positive effect on health after controlling for social background suggesting that participation potentially effects across the social spectrum and may even contribute to a reduction in health inequalities [20]. In addition, findings from longitudinal studies indicate that participation in extracurricular activities is associated with better academic engagement in early adulthood. It also provides opportunities for advancing adolescent interpersonal competence. The key mechanism is suggested to be the chance to form positive relationships with peers and adults outside the classroom and inspiring to build positive constructive life plans thus leading to reaching for life goals [27]. In addition, interventions promoting social inclusion in adolescents have been reported successful in reducing health risk behaviors in a longitudinal study design [29].
Hope, kindness and gratitude are character strengths that have been associated with better psychosocial well-being [30,31]. Not only being associated with mental well-being, hope and gratitude have been shown as protective factors against adolescent’s depressive and anxiety symptoms in various studies with both cross-sectional and longitudinal study designs [17]. Further, higher levels of kindness have predicted fewer depressive symptoms even when controlled for other strengths [30]. Character strengths have been described as crucial for optimal growth and development within adolescence, but also for life-long development. Similarly to personality traits, character strengths are considered as relatively stable. However, they are flexible to change and could be practiced and enhanced [32]. Strengthening one’s virtues enables young people to seek for greater, societal good [18]. Interventions that help people to identify their signature strengths can decrease depressive symptoms and increase happiness and life satisfaction [33]. Even brief character strength-based exercises in school have been reported to associate with increased life satisfaction among adolescents [19] and e.g., interventions promoting gratitude has been shown to increase satisfaction in life and school [34].
It is well acknowledged that positive mental health associates strongly to positive youth development. However, more evidence is needed on determinants and underlying mechanisms contributing to positive mental health and how they play a role in this complex set of features. Many studies have indicated the socioeconomic and demograhic factors’ effects on positive mental health. However, possibilities of adolescents to influence on these factors are scarce. Therefore, information is needed on those determinants of positive mental health that actually can be enhanced and promoted both in individual and societal level. More concretely, knowledge on youth positive mental health is needed for creating and implementing effective interventions enhancing positive mental health.
This study aims at exploring the associations between certain psychological and social determinants and self-reported positive mental health among adolescents, controlled for sociodemographic factors. More closely, this study explores the relations between positive mental health and self-esteem, character strengths of gratitude, hope and kindness, and experience of social inclusion, determinants that are each reported to associate with positive mental health and/or subjective well-being in different study designs and within different age groups, adolescents included. However, to our knowledge, these determinants of positive mental health have not been studied together in one study sample among adolescents. Thus, this study aims to explore the possible strength of these determinants compared to each other in regards of positive mental health as a larger concept. We hypothesize that, besides socioeconomic determinants as parental educational level and financial situation of the family, all these determinants, would associate positively with positive mental health.
Our explicit research questions were: 1) Is there an association between positive mental health and self-esteem, character strengths of gratitude, hope and kindness, and experience of social inclusion in a study sample of Finnish adolescents? 2) Which of these determinants have the strongest association with positive mental health, and 3) Does the association of psychological and social determinants overcome the strength of socioeconomic determinants of positive mental health–determinants that are commonly considered as strong predictors of positive mental health among adolescents?
2.1 Procedure and Participants
The study population (n = 195) consisted of comprehensive school students, 92 girls (47%) and 103 boys (53%) with mean age of 14.4 (SD 0.88). Students were recruited to the study within a Finnish Gutsy go-program that took place in November 2019 in two Finnish cities. The Gutsy go-program is an action media and training method for youth, designed to reshape how people think of peace and one’s ability to create an impact on society (www.gutsygo.fi). This study is based on baseline data collection prior to Gutsy go programme. Altogether 150 8th grade students from a southern city and 230 9th grade students from a northern city in Finland were invited to the study. Of them, 74% (n = 111) of 8th graders and 37% (n = 84) of 9th graders participated in the study. More than half of the students (54%, n = 105) were 14 years old, 43% (n = 83) were 15 years old and the minority, 3% (n = 6) were 16 years old. For one participant information on age was lacking. Information on those invited students that did not participate is not available for this study. The ethical approval for the study was granted by the Ethics Committee of Youth and Childhood Studies in September 2019.
The participants were invited to fill in the web-based questionnaire through an open link to the questionnaire website, and the link was provided for the students by their schools in prior to the beginning of Gutsy go-program. The students could easily access the questionnaire with their mobile phones or laptop. Each participant was encouraged to answer the questions by themselves. Informed consent was given electronically in prior to getting access to the actual questionnaire. Before implementation, the questionnaire had been pretested ensuring that it could be filled within less than 15 min. Answers were required in each question in order to proceed from question to another. Participants were also asked to give their e-mail address, so that they could be contacted for possible follow-up study later on. The questionnaire was provided in both Finnish and Swedish languages because one of the participating cities was located in Swedish-speaking region. The majority of the participants (n = 144, 74%) filled in the Finnish questionnaire.
Data on positive mental health, self-esteem and the experience of social inclusion as well as background factors was available for all 195 participants. Data on character strengths of gratitude, hope and kindness was available only for 185 participants due to a technical problem within the electronic questionnaire.
Positive mental health was measured with the Warwick Edinburgh Mental Well-Being Scale (WEMWBS) which is designed especially for use within general population samples. It is a 14-item scale covering both subjective (hedonic perspective) and psychological (eudaimonic perspective) functioning with all the items addressing positive mental health [35]. The scale is scored by summing the response to each item answered on a 1 to 5 Likert scale with the total score ranging between 14 and 70 and higher score indicating better positive mental health. The measure was designed initially for individuals ages 16 and above but it has been used as a valid study measure also within early adolescence [36]. The English version of WEMWBS has shown good psychometric properties [37]. The psychometric properties of the Finnish and Swedish versions of WEMWBS has not yet been reported thoroughly, but the measure has been used in various population-based studies successfully. The English version of the scale was translated into Finnish according to back translation method [38].
The character strengths were measured by using the Finnish adaptation [39] of the VIA Youth Survey (VIA Youth-96) [18]. The VIA Youth-96 is designed for children and adolescents between ages 10 and 17. It assesses 24 different character strengths that are grouped into six virtues, each including three to five separate character strengths. The VIA Youth-96 have demonstrated good internal consistency with alpha’s ranging from 0.72 to 0.91 [18]. In this study, only statements regarding the character strengths of gratitude, hope and kindness were measured. Each of these character strengths was measured with four statements with possible answers on a Likert scale from 1 (“not like me at all”) to 5 (“very much like me”) with the total score ranging from 4 to 20 for each character strength, with increasing scores indicating higher character strength.
The Finnish translation of the Rosenberg Self-Esteem Scale (RSES) [40] was used to explore self-esteem among the participants. RSES is a widely used 10-item self-report scale of global self-esteem that was originally designed and tested especially for adolescents. It consists of five items reflecting for positive and five for negative feelings about oneself. All items are answered using a 4-point Likert scale ranging from strongly disagree (0) to strongly disagree (3) with the total score ranging between 0 and 30 with higher scores reflecting higher global self-esteem. The internal reliability and factor structure of the RSES has been reported as psychometrically sound across many languages and cultures [41].
2.2.4 Experience of Social Inclusion
Experienced social inclusion was measured with the Experiences of Social Inclusion Scale (ESIS) developed in Finland [42]. It is a 10-item scale that includes statements regarding social interaction, experienced meaningfulness in life and beliefs in one’s possibilities to act and influence. Each statement is answered with 5-point Likert scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). The sum score between 10–50 is further modified into a scale from 0 to 100. The reports of validation of this measure are currently under review. Higher score indicates higher level of social inclusion.
The participants were asked to report their year of birth, official gender and the city where they went to school. Regarding social circumstances, the participants were asked about the living arrangements whether they lived with both of their parents, only with one parent, altering from parent to another in a regular manner or if they lived with someone else than their parent. Socioeconomic background factors included questions regarding mother’s and father’s educational level (Low: comprehensive school or equivalent; Middle: upper secondary school, high school or vocational school; High: University or university of applied sciences; not known). In addition, the participants were asked to evaluate the financial situation of one’s family (very good, fairly good, moderate, fairly poor, very poor).
The normality of distribution of each variable was tested by Shapiro-Wilk test, in addition to visual evaluation of histograms and Q-Q plots as well as detection of the skewness and kurtosis of each variable. All of the continuous variables were non-normally distributed and slightly positively skewed. Internal consistencies of continuous variables were evaluated by Cronbach’s α. The internal consistency was very good for WEMWBS (α = 0.910) and good for RSES (α = 0.800) as well as for ESIS (α = 0.894). Among the measured character strengths, gratitude (α = 0.683) and kindness (α = 0.721) showed acceptable internal consistencies, and the character strength of hope had good internal consistency (α = 0.848).
To compare differences between categorical background factors and WEMWBS total score (PMH), Mann-Whitney U-test was used for dichotomous variables (language, gender, grade) and Kruskal-Wallis test for variables including more than two groups (age, living arrangements, parental educational level and family’s financial situation).
Spearman’s correlations were explored between the total score of WEMWBS and the total scores of each character strength, RSES and ESIS. In addition, there was no multicollinearity between continuous predictor variables as evaluated by variance inflation factor (VIF) and the data showed homoscedasticity, evaluated by scatterplots.
Further on, General Linear Model (univariate) was applied to explore and control for the individual effects of each determinant associated with positive mental health. Building the GLM model proceeded stepwise with reduction of variables without a statistically significance association in the model. Within all the analyses, two significance levels were considered (p < 0.001 and p < 0.05). To ensure that the GLM was appropriate method to use with non-normally distributed variables, the normality of distribution of the residuals of each model were explored, and no violations against assumptions were detected. The analyses were conducted using SPSS 24.0.
3.1 Characteristics of the Study Population
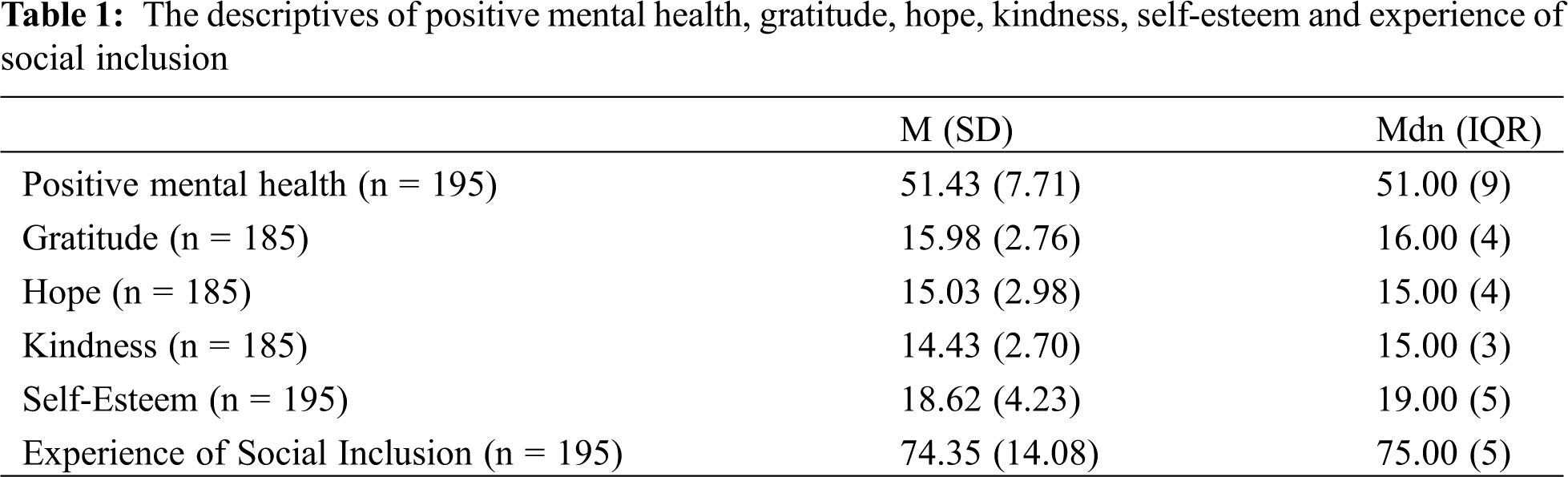
The descriptives of positive mental health, character strengths, self-esteem and experience of social inclusion are presented in Tab. 1.
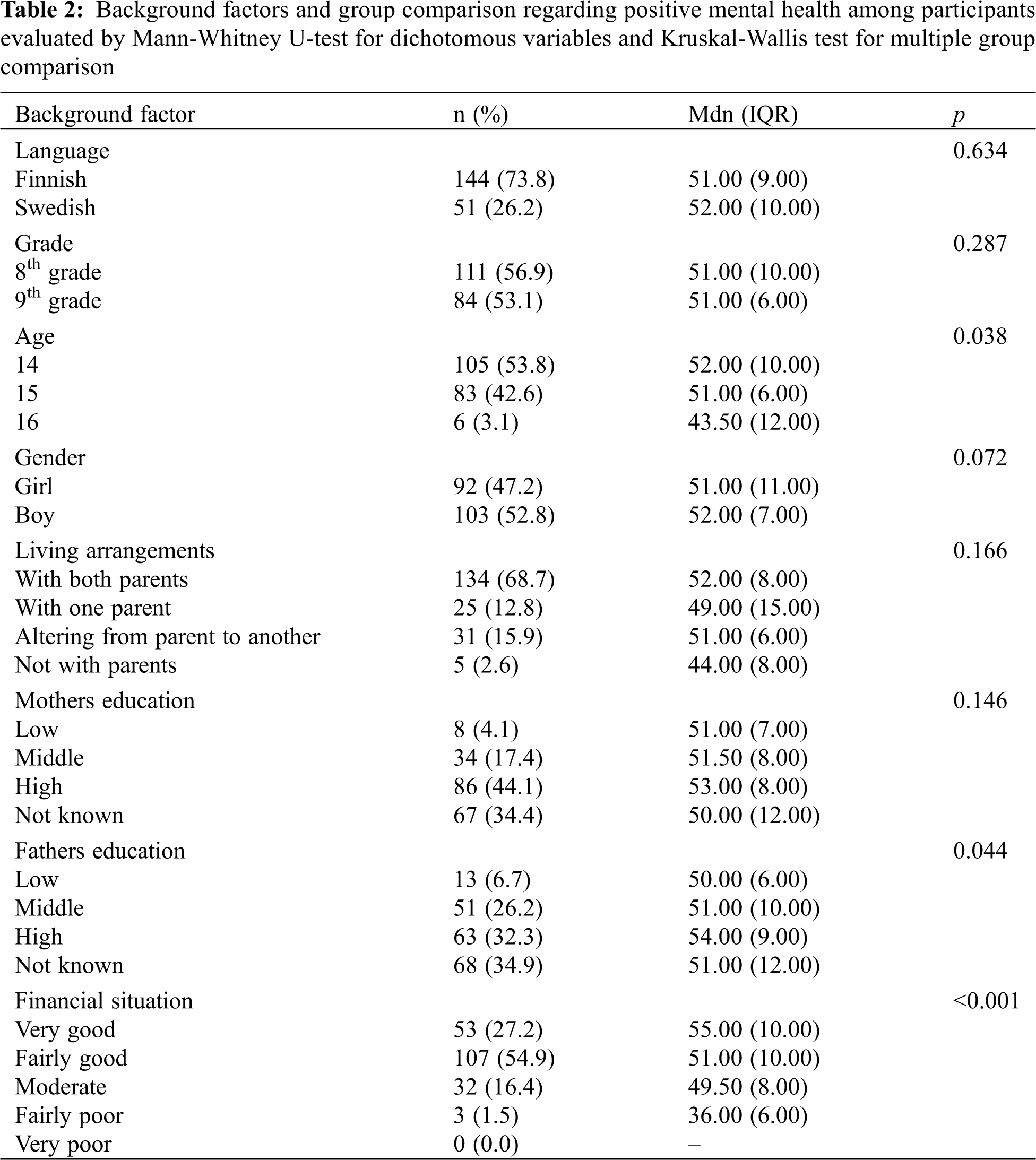
The associations of demographic characteristics, character strengths, self-esteem and experience of social inclusion with positive mental health are presented in Tab. 2. The level of positive mental health was consistently higher in concordance to better family’s financial situation (H(3) = 22.292, p < 0.001). Higher positive mental health was also associated with younger age of the student (H(3) = 8.411, p = 0.038) and higher level of father’s education (H(3) = 8.112, p = 0.044). There were no significant group differences found for language, grade, gender, living arrangements and mother’s education. For closer details see Tab. 2.
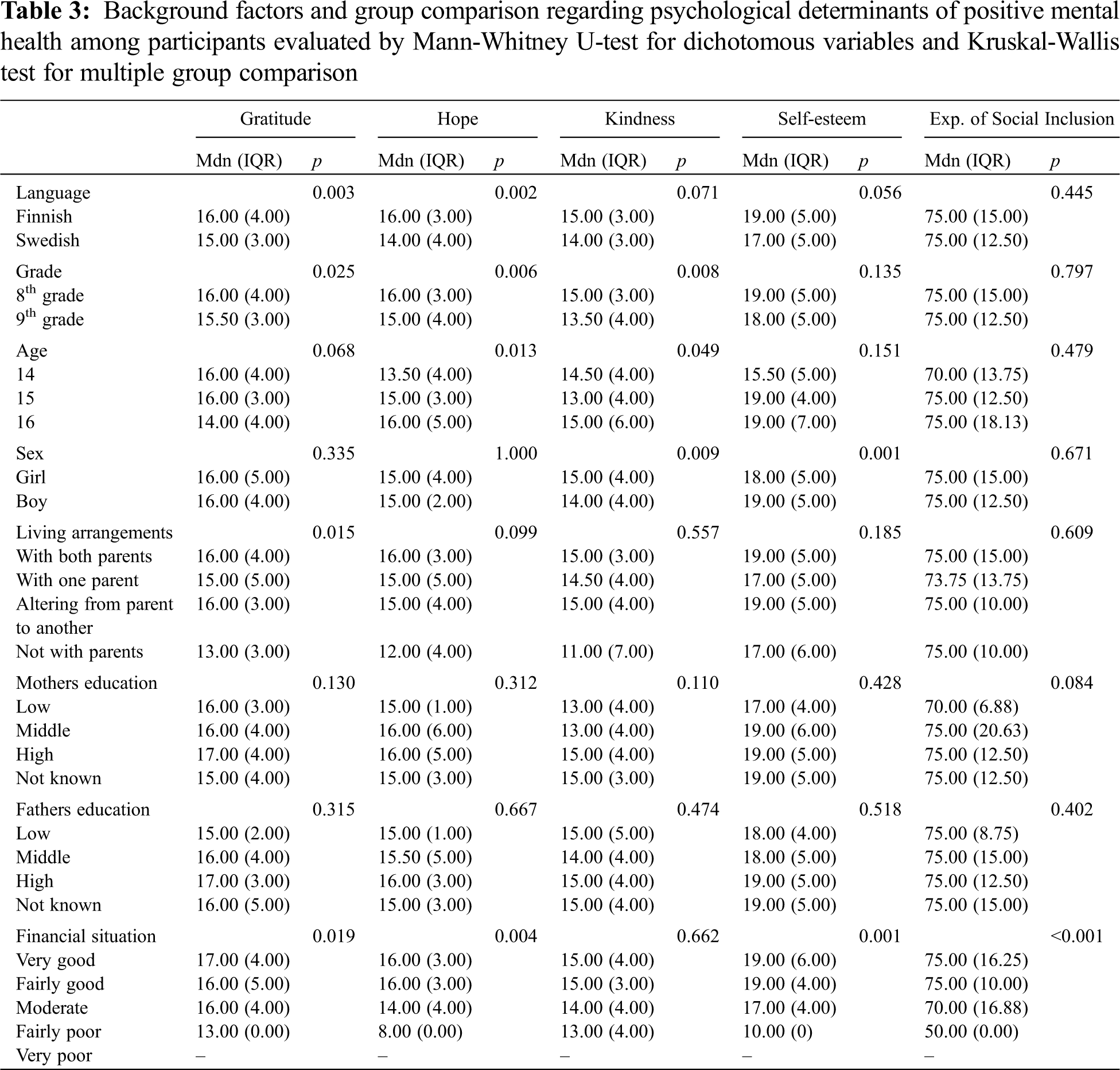
Differences for each psychological determinant of positive mental health were explored regarding the background factors and the results are presented in Tab. 3. Better family’s financial situation was also consistently associated with higher level of gratitude (H(3) = 9.992, p = 0.019), hope (H(3) = 13.303, p = 0.004), self-esteem (H(3) = 16.119, p = 0.001) as well as the experience of social inclusion (H(3) = 26.367, p < 0.001). Living arrangements were significantly associated with gratitude (H(3) = 10.528, p = 0.015) with those living with both parents all the time or altering from one parent to another having higher level of gratitude compared to those living with only one parent or not with parents at all. In addition, the younger the participant was, the higher was the level of hope (H(3) = 10.758, p = 0.013) and kindness (H(3) = 7.872, p = 0.049).
Interestingly, all the measured character strengths were on a significantly higher level among 8th graders compared to 9th graders. They reported higher level of gratitude (U = 3408.500, P = 0.025), hope (U = 3221.500, P = 0.006) and kindness (U = 3253.500, P = 0.008) in comparison to 9th graders. Significant gender differences were also detected, as boys had higher self-esteem than girls (U = 6011, P = 0.001), whereas girls had higher level of kindness than boys (U = 3387.50, P = 0.009). Lastly, those who filled in the questionnaire in Finnish language had higher levels of hope (U = 2117.00, P = 0.002) and gratitude (U = 2171.00, P = 0.003) than those who filled in the questionnaire in Swedish.
The strongest positive correlation was detected between positive mental health and self-esteem (r = 0.673, p < 0.001). Moderate positive correlations were also detected between positive mental health and hope (r = 0.642, p < 0.001), experience of social inclusion (r = 0.624, p < 0.001) and gratitude (r = 0.529, p < 0.001). In addition, a small positive correlation was found between positive mental health and kindness (r = 0.396, p < 0.001). All the psychological determinants of positive mental health had small to moderate correlations with each other but without evident multicollinearity (r < 0.7).
3.3 Determinants of Positive Mental Health
General Linear Model was computed to explore the individual effects of each character strength, self-esteem and experience of social inclusion as well as paternal education level, family’s financial situation and the year of birth of the participant on positive mental health. Analyses proceeded stepwise with reduction of those variables that did not show statistically significant association with positive mental health. Consequently, the final model included self-esteem, hope, kindness, experience of social inclusion and age. The strongest association was found between positive mental health and self-esteem (β = 0.789, p < 0.001, η2P = 0.174) with a medium effect size, followed by character strengths of hope and kindness as well as experience of social inclusion with small effect sizes. The overall results are described more in detail in Tab. 4.

The aim of the present study was to explore adolescents’ positive mental health and its possible determinants controlled for sociodemographic factors. Our main finding was that higher level of positive mental health was significantly associated with higher self-esteem, higher levels of character strengths of hope and kindness and experience of social inclusion. In addition, younger age associated with higher level of positive mental health. Interestingly, socioeconomic factors like parental educational level and financial situation of the family did not show significant associations with positive mental health.
In the present study, the strongest association was found between self-esteem and positive mental health. High self-esteem has indeed been found to associate with the hedonic perspective of positive mental health by higher subjective well-being [16,21]. However, not only positive mental health but also self-esteem include different domains indicating that the relation is likely to be more complex. As Orth et al. [22] have stated, self-esteem includes feelings of self-acceptance and self-respect. These feelings can be projected towards one’s psychological as well as physical characteristics. For instance, greater satisfaction of self-appearance has been associated with higher positive mental health among youth [12]. Indeed, it is suggested that, especially during adolescence, the feelings and thoughts one has regarding own physical appearance may influence strongly to the self-concept as a whole [43]. Girls tend to have more critical opinions against their appearance than boys which may partly explain that girls usually have lower levels of self-esteem than boys [44] as was in the current study as well.
Furthermore, the development of self-esteem during adolescence is highly dependent on both individual’s characteristics and social factors, such as approval and support from peers and family. It has been suggested that self-esteem would act as a motivational force that influences perceptions and coping behaviors, and that people must think positively about themselves in order to defend and to improve their positive self-perception, sometimes even by relying on overestimations and exaggerations. In addition, stress theories have indicated that high self-esteem, especially when contributed with strong social support, functions as a buffer for stressors, thus, leading to the ability to improve and maintain better mental health [21].
In the current study, also higher levels of hope and kindness were significantly associated with higher positive mental health. Gillham et al. describes that character strengths belonging to the virtue ‘transcendence’, e.g., hope, have been suggested to strengthen well-being by giving adolescents a deeper sense of purpose and connection to others. Kindness, as other-directed strength may ease building friendships increasing social support, positive experiences and happiness. Previous research has shown that especially strengths that connect people to each other are those that are more firmly connected to well-being in adolescence [30]. As hope, gratitude and kindness all correlated strongly with experience of social inclusion, it seems convincing that connection to others and sense of inclusion, might be an important link within the relation between character strengths and positive mental health.
In line with previous research [7,12,13] better financial situation of the family was found to associate with higher positive mental health in the current study. In contrast to our hypotheses, however, parental educational level was not significantly associated with positive mental health when controlled for other related factors. Results supporting this finding have been presented by Zambon et al. [20] who reported social participation having strong individual effect on adolescents’ health over social background. Guo et al. [12] have also reported that social trust associated with better positive mental health. Children and adolescents need environmental and attitudinal support for participation in activities within the community, especially when having disability of any kind [45] or less social skills to interact with other children [27]. Therefore, experiences of social participation and belonging to a community, can neither be only dependent on adolescent’s skills, personality, nor family’s background. Moreover, it should be acknowledged that social inclusion and sense of participation is influenced by individual’s characteristics and the opportunities provided by society. It should be promoted by the actions of community and enhanced by actively developing possibilities for social inclusion for all, and especially for those, who are prone to have difficulties in social interaction or who have less possibilities to engage in leisure and outside school activities due to financial difficulties of the family.
In terms of the results regarding effects of family’s financial situation on positive mental health, it seems that self-esteem, character strengths and experience of social inclusion might have stronger influence on youth mental well-being than family economics. Therefore, it should be discussed whether psychological determinants overcome the individual effect of even well acknowledged and widely studied poor socioeconomic status within the relations with positive mental health. Further studies are needed to establish these results more firmly. However, these preliminary findings are interesting as these–rather than the financial situation of the family-are determinants that can be influenced by interventions. More precisely, it could possibly mean that enhancing these determinants-self-esteem, hope, kindness and experience of social inclusion-the risk for lower positive mental health for those with poorer socioeconomic background could be to some extent compensated.
In the present study, older students reported lower levels of positive mental health in comparison to younger students. According to previous research [12,15], the crucial time with trend of decreasing positive mental health is the age period of 12 to 18. In a large Finnish school-based study by Appelqvist-Schmidlechner et al. [13], 8th graders reported lower level of positive mental health compared with students in secondary schools. It seems that positive mental health is quite sensitive to changes during adolescence due to multiple stressors that are typical for this age group, such as pressure for academic achievements, success in peer relationships and developing identity. Adolescence is a sensitive time period both for negative and positive influences and thus, enhancing positive mental health is of extreme importance specifically during early adolescence.
As presented, adolescents’ positive mental health includes various psychological and sociodemographic determinants. Some of them cannot be intervened by influencing the young themselves, i.e., age, gender and family’s financial situation. The results of the present study suggest that determinants, that can be influenced, might actually have greater role within positive mental health. Especially psychological and social determinants such as character strengths [18,19], experience of participation [27] and self-esteem [21] could be enhanced by targeted interventions on individual level and by the support of environment, like school. The results highlight the importance of mental health promotion in early adolescence, in a sensitive time period for changes in positive mental health.
Strengths and limitations
This study explored positive mental health as a multidimensional phenomenon and widened the knowledge of determinants of adolescents’ positive mental health.
However, there are some limitations regarding our study. This study is based on self-report measures and, thus, the results present a subjective perspective of the well-being of study participants. Self-reports might be especially challenging for younger adolescents as they might have difficulties in understanding concepts that are relatively abstract and, therefore, there is a risk for over-or underreporting [46]. However, we used validated measures in the current study. The character strengths were measured by using questions from the VIA Youth-96 survey but not by using the complete survey. To our knowledge, parts of this survey has not previously been used accordingly in studies exploring positive mental health. It should also be acknowledged that the Finnish version of VIA Youth-96 is not reportedly validated measure and the psychometric properties of this measure have not been reported thoroughly yet. However, internal consistencies for these variables were either good or acceptable, and thus, could be used in this manner. Though, criticism on focusing only on few character strengths at a time have been presented. Strengths are highly correlated with each other and thus when one strength predicts well-being it could actually reflect the effects of other strengths that were not explored [30]. Within a questionnaire that includes many aspects of positive mental health and thus, various questions, we evaluated that the best compliance in regard to participating in the study would be achieved by restricting the number of questions so that adolescents would not be too overwhelmed by the length of the questionnaire. Thus, only selected character strengths were included in the study. Other scales used in this study are widely used in Finland, validated and either original in Finnish or translated according to the guidelines of back translation method from the original into Finnish.
The sample size of the present study was relatively small but sufficient for the purpose of the study. Generalization of the study findings or comparison with other populations should, however, be made cautiously. Finally, due to cross-sectional and correlational nature of our study, causal relations are not indicated. Therefore, further studies are needed to deepen the understanding within these phenomena and the directions of these associations. In addition, to truly understand the mechanisms behind these associations it could be beneficial to extend the study to qualitative approach with e.g., focus group interviews of the adolescents.
The objective of this study was to explore self-esteem, hope, kindness and gratitude as well as experience of social inclusion as determinants of positive mental health among adolescents. The study showed that all of these determinants, except for gratitude, were significantly associated with positive mental health, self-esteem having the strongest effect even when controlled for sociodemographic factors. As the role of family’s financial situation on positive mental health was diminished to a non-significant level when within the analyses, the results suggest that self-esteem, hope, kindness and experience of social inclusion may overcome the effect of socioeconomic factors within the relations with positive mental health. Thus, the findings highlight the role of enhancing adolescents’ psychological and social domains as potential route for better mental well-being. More evidence with larger samples and longitudinal study designs are needed to widen the knowledge of the complex relationship between psychological and social determinants of positive mental health.
Funding Statement: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. Maughan, B., Collishaw, S. (2018). Development and psychopathology: A life course perspective. Rutter’s Child an Adolescent Psychiatry. 6th edition, Oxford, UK: John Wiley & Sons, Ltd. [Google Scholar]
2. WHO (2005). Caring for children and adolescents with mental disorders: setting WHO directions. Geneva: World Health Organization. [Google Scholar]
3. Dray, J., Bowman, J., Campbell, E., Freund, M., Wolfenden, L. et al. (2017). Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. Journal of the American Academy of Child and Adolescent Psychiatry, 56(10), 813–824. [Google Scholar]
4. Fenwick-Smith, A., Dahlberg, E., Thompson, S. C. (2018). Systematic review of resilience enhancing, universal, primary school-based mental health promotion programs. BMC Psychology, 6, 30. [Google Scholar]
5. MacKenzie, K., Williams, C. (2018). Universal, school-based interventions to promote mental and emotional well-being: What is being done in the UK and does it work? A systematic review. BMJ Open, 8(e022560), 1–14. [Google Scholar]
6. Stengård, E., Appelqvist-Schmidlechner, K. (2010). Mental health promotion in young people–An investment for the future. Copenhagen, Denmark: World Health Organization. [Google Scholar]
7. Clarke, A., Friede, T., Putz, R., Ashdown, J., Martin, S. et al. (2011). Warwick-Edinburgh Mental Well-being Scale (WEMWBSValidated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health, 11, 487. [Google Scholar]
8. Ryan, R., Deci, E. (2001). On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annual Review of Psychology, 52, 141–166. [Google Scholar]
9. Vaillant, G. E. (2012). Positive mental health: Is there a cross-cultural definition? World Psychiatry, 11(2), 93–99. [Google Scholar]
10. Huppert, F. A., So, T. T. (2013). Flourishing across Europe: Application of a new conceptual framework for defining well-being. Social Indicators Research, 110(3), 837–861. [Google Scholar]
11. Keyes, C., Eisenberg, D., Perry, G., Dube, S., Kroenke, K. et al. (2012). The relationship of level of positive mental health with current mental disorders in predicting suicidal behavior and academic impairment in college students. Journal of American College Health, 60(2), 126–133. [Google Scholar]
12. Guo, C., Tomson, G., Keller, C., Söderqvist, F. (2018). Prevalence and correlates of positive mental health in Chinese adolescents. BMC Public Health, 18, 263. [Google Scholar]
13. Appelqvist-Schmidlechner, K., Tamminen, N., Solin, P. (2019). Nuorten kokema positiivinen mielenterveys perhetaustan mukaan. Helsinki, Finland: Finnish Institute for Health and Welfare. [Google Scholar]
14. Uusitalo-Malmivaara, L. (2014a). Happiness decreases during early adolescence. Psychology, 5, 541–555. [Google Scholar]
15. Keyes, C. (2006). Mental health in adolescence: Is America’s youth flourishing? American Journal of Orthopsychiatry, 76(3), 395–402. [Google Scholar]
16. Du, H., King, R. B., Chi, P. (2017). Self-esteem and subjective well-being revisited: The roles of personal, relational, and collective self-esteem. PLoS One, 12(8), 1–17. [Google Scholar]
17. Padilla-Walker, L., Millett, M., Memmott-Elison, M. (2020). Can helping others strengthen teens? Character strengths as mediators between prosocial behavior and adolescents’ internalizing symptoms. Journal of Adolescence, 79, 70–80. [Google Scholar]
18. Park, N., Peterson, C. (2006). Moral competence and character strengths among adolescents: The development and validation of the values in action inventory of strengths for youth. Journal of Adolescence, 29, 891–909. [Google Scholar]
19. Proctor, C., Tsukayama, E., Wood, A. M., Maltby, J., Fox Eades, J. et al. (2011). Strengths gym: The impact of a character strengths-based intervention on the life satisfaction and well-being of adolescents. Journal of Positive Psychology, 6, 377–388. [Google Scholar]
20. Zambon, A., Morgan, A., Vereecken, C., Colombini, S., Boyce, W. et al. (2009). The contribution of club participation to adolescent health: Evidence from six countries. Journal of Epidemiology and Community Health, 64, 89–95. [Google Scholar]
21. Mann, M., Hosman, C., Schaalma, H., de Vries, N. (2004). Self-esteem in a broad-spectrum approach for mental health promotion. Health Education Research, 19(4), 357–372. [Google Scholar]
22. Orth, U., Robins, R. (2014). The development of self-esteem. Current Directions in Psychological Science, 23(5), 381–387. [Google Scholar]
23. Kiviruusu, O., Berg, N., Huurre, T., Aro, H., Marttunen, M. et al. (2016). Interpersonal conflicts and development of self-esteem from adolescence to mid-adulthood. A 26-year follow-up. PLoS One, 11(10), 1–17. [Google Scholar]
24. Mamatis, D., Sanford, S., Ansara, D., Roche, B. (2019). Promoting health and well-being through social inclusion in Toronto: Synthesis of International and local evidence and implications for future action. Toronto Public Health and Wellesley Institute. [Google Scholar]
25. Berry, C., Greenwood, K. (2018). Beliefs in social inclusion: Invariance in associations among hope, dysfunctional attitudes, and social inclusion across adolescence and young adulthood. Developmental Psychopathology, 30, 1403–1419. [Google Scholar]
26. Eccles, J. S., Barber, B. L., Stone, M., Hunt, J. (2003). Extracurricular activities and adolescent development. Journal of Social Issues, 59, 865–869. [Google Scholar]
27. Mahoney, J. L., Cairns, B. D., Farmer, T. W. (2003). Promoting interpersonal competence and educational success through extracurricular activity participation. Journal of Educational Psychology, 95, 409–418. [Google Scholar]
28. Appelqvist-Schmidlechner, K., Vaara, J., Häkkinen, A., Vasankari, T., Mäkinen, J. et al. (2018). Relationships between youth sports participation and mental health in young adulthood among finnish males. American Journal of Health Promotion, 32(7), 1502–1509. [Google Scholar]
29. Patton, G., Bond, L., Carlin, J., Thomas, L. (2006). Promoting social inclusion in schools: A group-randomized trial of effects on student health risk behavior and well-being. American Journal of Public Health, 96(6), 1582–1587. [Google Scholar]
30. Gillham, J., Adams-Deutsch, Z., Werner, J., Reivich, K., Coulter-Heindl, V. et al. (2011). Character strengths predict subjective well-being in adolescence. Journal of Positive Psychology, 6(1), 31–44. [Google Scholar]
31. Yeung, D., Ho, S., Mak, C. (2015). Brief report: Attention to positive information mediates the relationship between hope and psychosocial well-being of adolescents. Journal of Adolescence, 42, 98–102. [Google Scholar]
32. Peterson, C., Seligman, M. E. P. (2004). Character strengths and virtues: A handbook and classification. Washington DC: American Psychological Association and Oxford University Press. [Google Scholar]
33. Seligman, M. E. P., Rashid, T., Parks, A. C. (2006). Positive psychotherapy. American Psychologist, 61, 774–778. [Google Scholar]
34. Froh, J. J., Sefick, W. J., Emmons, R. A. (2008). Counting blessings in early adolescents: An experimental study of gratitude and subjective well-being. Journal of School Psychology, 46, 213–233. [Google Scholar]
35. Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S. et al. (2007). The Warwick-Edinburgh Mental Well-being Scale (WEMWBSDevelopment and UK validation. Health and Quality of Life Outcomes, 5, 63. [Google Scholar]
36. Taggart, F., Friede, T., Weich, S., Clarke, A., Johnson, M. et al. (2013). Cross cultural evaluation of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS)-a mixed methods study. Health and Quality of Life Outcomes, 11, 27. [Google Scholar]
37. Stewart-Brown, S., Tennant, A., Tennant, R., Platt, S., Parkinson, J. et al. (2009). Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBSA Rasch analysis using data from the Scottish Health Education Population Survey. Health and Quality of Life Outcomes, 7, 15. [Google Scholar]
38. Tamminen, N., Reinikainen, J., Appelqvist-Schmidlechner, K., Borodulin, K., Mäki-Opas, T. et al. (2020). Associations of physical activity with positive mental health: A population-based study. Mental Health and Physical Activity, 18, 1–8. [Google Scholar]
39. Uusitalo-Malmivaara, L. (2014b). VIA-vahvuusmittari lasten ja nuorten luonteenvahvuuksien kartoitukseen. NMI-Bulletin, 24(1), 42–50. [Google Scholar]
40. Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press. [Google Scholar]
41. Schmitt, D., Allik, J. (2005). Simultaneous administration of the Rosenberg Self-Esteem Scale in 53 nations: Exploring the universal and culture-specific features of global Self-Esteem. Journal of Personality and Social Psychology, 89(4), 623–642. [Google Scholar]
42. Leemann, L., Martelin, T., Koskinen, S., Härkänen, T., Isola, A. M. (2019). Development and psychometric evaluation of the experiences of social inclusion scale (Unpublished manuscript). [Google Scholar]
43. O’Dea, J. A. (2012). Body image and self-esteem. In: Cash, T. F. (eds.Encyclopedia of body image and human appearance, pp. 141–147. [Google Scholar]
44. Quatman, T., Watson, C. M. (2001). Gender differences in adolescent self-esteem: An exploration of domains. The Journal of Genetic Psychology, 162(1), 93–117. [Google Scholar]
45. Bedell, G., Coster, W., Law, M., Liljenquist, K., Kao, Y. C. et al. (2013). Community participation, supports, and barriers of school-age children with and without disabilities. Archives of Physical Medicine and Rehabilitation, 94, 315–323. [Google Scholar]
46. Moksnes, U. K., Løhre, A., Lillefjell, M., Byrne, D. G., Haugan, G. (2016). The association between school stress, life satisfaction and depressive symptoms in adolescents: Life satisfaction as a potential mediator. Social Indicators Research, 125(1), 339–357. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |